Muscles of shoulder region rotator cuff muscles and intermuscular spaces. Explain the topic with respect to anatomy ms-1 level
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Loading Image
Finding Sources
I now have all the information needed to write a complete, well-illustrated MS-1 level anatomy explanation. Let me compile the comprehensive answer:
Muscles of the Shoulder Region, Rotator Cuff, and Intermuscular Spaces
Sources: Gray's Anatomy for Students; General Anatomy and Musculoskeletal System (THIEME Atlas); Rockwood and Green's Fractures in Adults
Overview
The shoulder region can be divided into two main areas:
- The shoulder (scapular) region - including the superficial layer and the posterior scapular region
- The glenohumeral joint - stabilized critically by the rotator cuff
Part 1: Superficial Muscles of the Shoulder
Trapezius
| Feature | Details |
|---|---|
| Origin | Superior nuchal line, external occipital protuberance, medial margin of ligamentum nuchae, spinous processes CV II - T XII |
| Insertion | Superior edge of crest of spine of scapula, acromion, posterior border of lateral 1/3 of clavicle |
| Innervation | Motor: Accessory nerve (CN XI); Sensory (proprioception): anterior rami C3, C4 |
| Action | Powerful elevator of scapula; rotates scapula during abduction above horizontal; middle fibers retract; lower fibers depress scapula |
Deltoid
| Feature | Details |
|---|---|
| Origin | Inferior edge of crest of spine of scapula, lateral margin of acromion, anterior border of lateral 1/3 of clavicle |
| Insertion | Deltoid tuberosity of humerus |
| Innervation | Axillary nerve (C5, C6) |
| Action | Major abductor of arm; clavicular fibers flex; posterior fibers extend the arm |
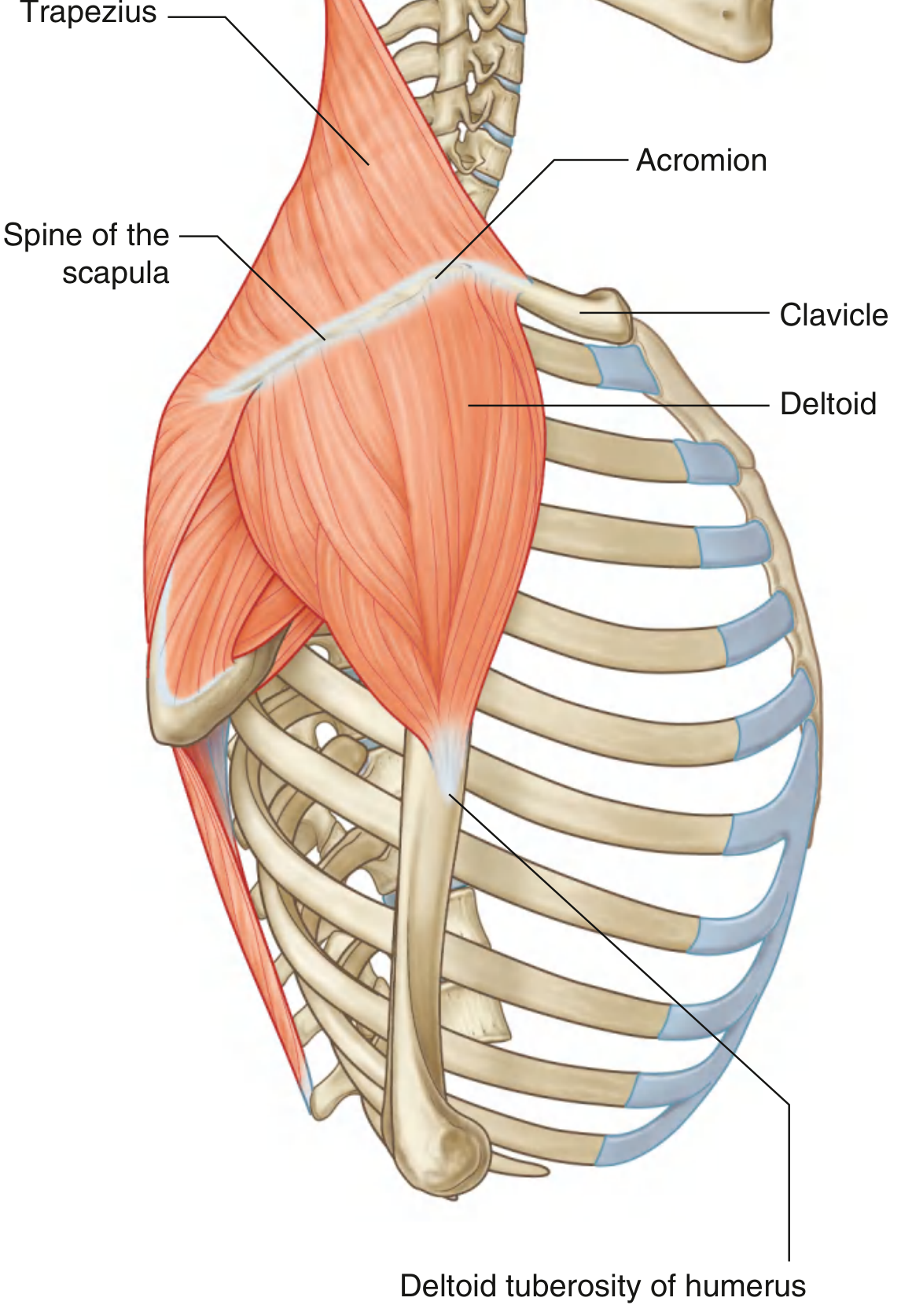
Key point: The trapezius attaches the scapula and clavicle to the trunk, while the deltoid attaches the scapula and clavicle to the humerus. Together, they provide the characteristic contour of the shoulder. Both attach to opposing surfaces and margins of the spine of scapula, acromion, and clavicle.
Muscles Deep to Trapezius (Scapulothoracic Muscles)
Three muscles connect the scapula to the vertebral column:
Levator Scapulae
- Origin: Transverse processes of C1-C2, posterior tubercles of C3-C4 transverse processes
- Insertion: Posterior surface of medial border of scapula (superior angle to root of spine)
- Innervation: Dorsal scapular nerve + direct branches from C3, C4
- Action: Elevates the scapula
Rhomboid Minor
- Origin: Lower ligamentum nuchae, spinous processes CVII and TI
- Insertion: Smooth triangular area at root of spine of scapula (posterior surface)
- Innervation: Dorsal scapular nerve (C5)
- Action: Retracts and elevates the scapula
Rhomboid Major
- Origin: Spinous processes TII-TV + supraspinous ligaments
- Insertion: Posterior surface of medial border of scapula (root of spine to inferior angle)
- Innervation: Dorsal scapular nerve (C4, C5)
- Action: Retracts and elevates the scapula
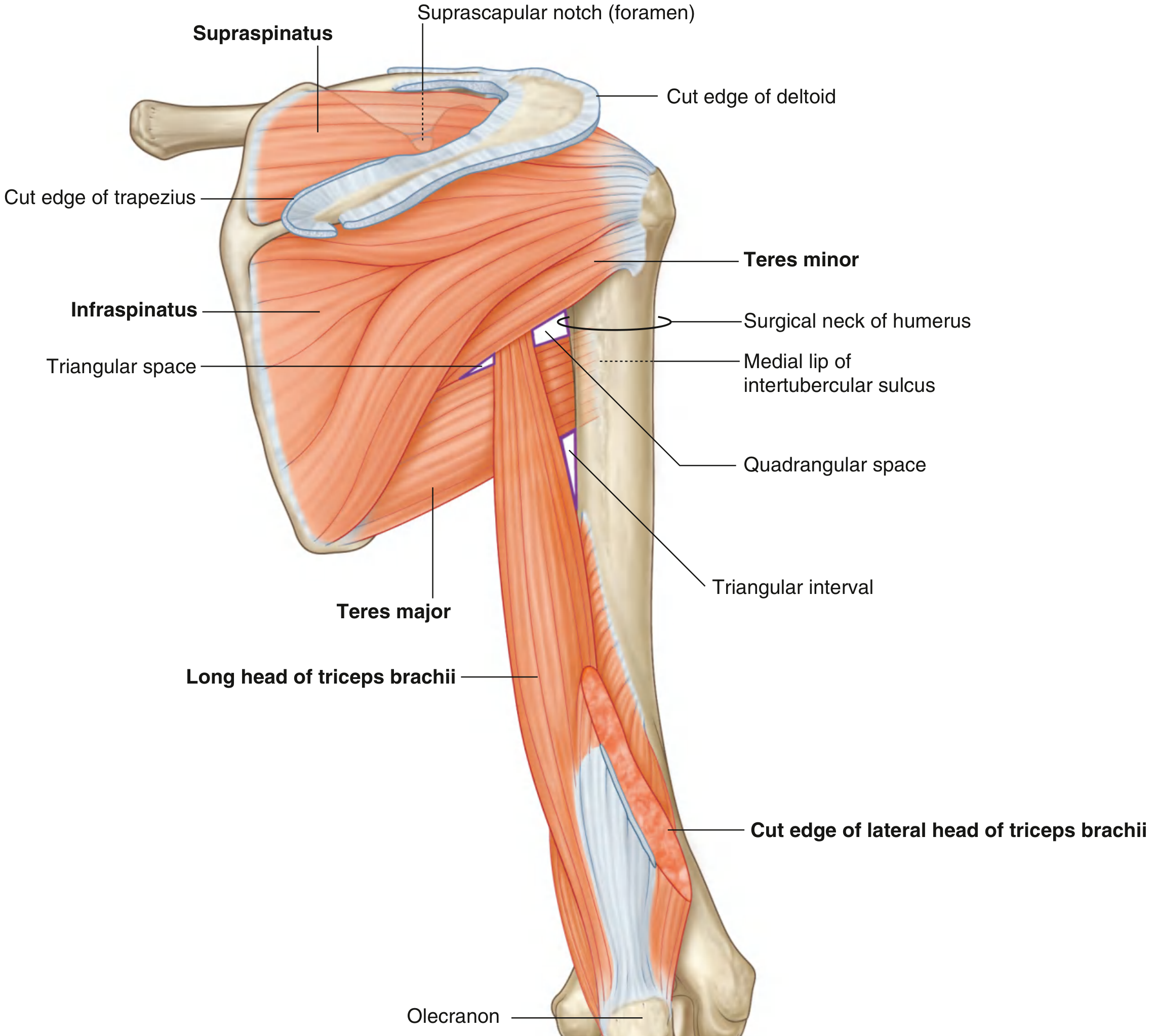
Part 2: The Posterior Scapular Region
The posterior scapular region lies deep to the trapezius and deltoid. It contains four muscles passing between the scapula and proximal humerus:
- Supraspinatus
- Infraspinatus
- Teres minor
- Teres major
The long head of triceps brachii also passes through this region and participates in forming intermuscular spaces.
Part 3: The Rotator Cuff (SITS Muscles)
The rotator cuff is a group of four muscles whose tendons blend with the glenohumeral joint capsule, forming a cuff that stabilizes the humeral head within the glenoid cavity. The acronym SITS is a useful mnemonic:
| Letter | Muscle | Action | Nerve |
|---|---|---|---|
| S | Supraspinatus | Initiates abduction; stabilizes | Suprascapular (C5, C6) |
| I | Infraspinatus | Lateral rotation; stabilizes | Suprascapular (C5, C6) |
| T | Teres minor | Lateral rotation; stabilizes | Axillary (C5, C6) |
| S | Subscapularis | Medial rotation; stabilizes | Upper + lower subscapular (C5, C6) |
Individual Muscle Details
1. Supraspinatus
- Origin: Medial 2/3 of supraspinous fossa + deep fascia covering the muscle
- Insertion: Most superior facet of greater tubercle of humerus
- Innervation: Suprascapular nerve (C6) - passes through suprascapular foramen
- Action: Initiates abduction of glenohumeral joint (first 15°); stabilizes head of humerus in glenoid cavity
Clinical note: The supraspinatus tendon passes beneath the acromion and acromioclavicular ligament through a fixed-dimension space. This makes it the most commonly impinged and torn rotator cuff tendon. Blood supply is relatively poor, making it susceptible to degenerative change, calcium deposition, and partial/full-thickness tears. - Gray's Anatomy for Students, p.831
2. Infraspinatus
- Origin: Medial 2/3 of infraspinous fossa + deep fascia
- Insertion: Middle facet on posterior surface of greater tubercle of humerus
- Innervation: Suprascapular nerve (C6) - passes through greater scapular (spinoglenoid) notch
- Action: Lateral rotation of arm at glenohumeral joint; stabilizes joint
3. Teres Minor
- Origin: Upper 2/3 of a narrow strip on the posterior surface of the lateral border of scapula
- Insertion: Lowest (inferior) facet of greater tubercle of humerus
- Innervation: Axillary nerve (C5, C6)
- Action: Lateral rotation of arm; stabilizes glenohumeral joint
4. Subscapularis (the "S" on the anterior side)
- Origin: Medial 2/3 of subscapular fossa (anterior/costal surface of scapula)
- Insertion: Lesser tubercle of humerus (and capsule of glenohumeral joint)
- Innervation: Upper and lower subscapular nerves (C5, C6)
- Action: Medial rotation of arm; stabilizes glenohumeral joint
- This muscle is located anterior to the shoulder joint, forming much of the posterior wall of the axilla
Key concept: The four rotator cuff tendons blend with and reinforce the glenohumeral joint capsule. Contribution to stability occurs through: (1) joint compression, (2) barrier effect (the tendons physically block displacement), and (3) dynamic ligament-like effect. - Rockwood and Green's Fractures in Adults
Part 4: Teres Major (not a rotator cuff muscle)
While not part of the rotator cuff, teres major is important for defining the intermuscular spaces:
- Origin: Oval area on posterior surface of inferior angle of scapula
- Insertion: Medial lip of the intertubercular sulcus (bicipital groove) of humerus
- Innervation: Lower subscapular nerve (C5, C6)
- Action: Medial rotation and extension of arm; adducts the arm ("little lat")
Part 5: Intermuscular Spaces
Three intermuscular spaces are formed in the posterior scapular region by the borders of the teres minor, teres major, long head of triceps brachii, and the surgical neck of humerus. These spaces serve as conduits for neurovascular structures.
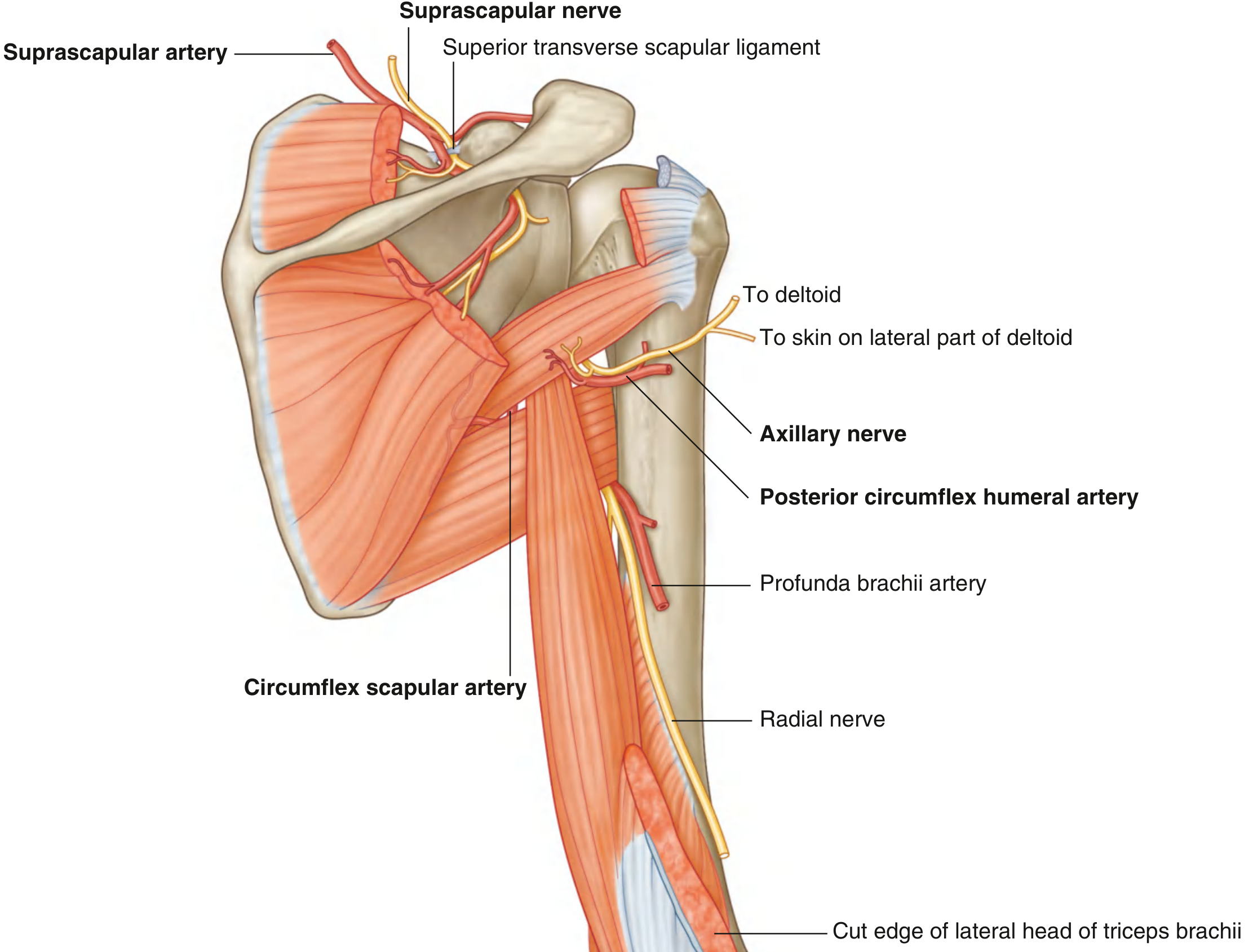
1. Quadrangular Space (Quadrilateral Space)
Boundaries:
- Superior: Inferior margin of teres minor
- Inferior: Superior margin of teres major
- Medial: Lateral margin of long head of triceps brachii
- Lateral: Surgical neck of humerus
Contents:
- Axillary nerve (posterior cord, C5, C6)
- Posterior circumflex humeral artery (and vein)
Clinical significance: Quadrilateral space syndrome - compression of the axillary nerve and posterior circumflex humeral artery within this space, most commonly by a fibrous band between teres major and minor. Presents with pain and paresthesia in the shoulder, worsened by abduction and external rotation.
2. Triangular Space (Medial Triangular Space)
Boundaries (viewed from posterior):
- Lateral (and inferior): Medial margin of long head of triceps brachii
- Superior: Inferior margin of teres minor
- Inferior: Superior margin of teres major
Contents:
- Circumflex scapular artery (and vein) - branch of subscapular artery
- This space communicates between the axilla and posterior scapular region
3. Triangular Interval (Lower Triangular Space / Lateral Triangular Space)
Boundaries:
- Medial: Lateral margin of long head of triceps brachii
- Superior: Inferior margin of teres major
- Lateral: Shaft of humerus
Contents:
- Radial nerve
- Profunda brachii artery (deep artery of arm) and associated veins
Because this space lies below the inferior margin of teres major (which marks the inferior boundary of the axilla), the triangular interval serves as a passageway between the anterior and posterior compartments of the arm and between the posterior arm and axilla.
Summary Table: Intermuscular Spaces
| Space | Boundaries | Contents | Clinical Relevance |
|---|---|---|---|
| Quadrangular | Teres minor (sup), Teres major (inf), Long head triceps (medial), Surgical neck humerus (lateral) | Axillary nerve, Posterior circumflex humeral artery | Quadrilateral space syndrome; axillary nerve injury in shoulder dislocation |
| Triangular (medial) | Long head triceps (lateral), Teres minor (sup), Teres major (inf) | Circumflex scapular artery | Surgical access to posterior scapular region |
| Triangular Interval (lateral) | Long head triceps (medial), Teres major (sup), Humeral shaft (lateral) | Radial nerve, Profunda brachii artery | Radial nerve injury (Saturday night palsy) |
Summary: Rotator Cuff Muscles at a Glance
| Muscle | Origin | Insertion | Nerve | Action |
|---|---|---|---|---|
| Supraspinatus | Supraspinous fossa | Superior facet, greater tubercle | Suprascapular (C5,C6) | Abduction (initiates); stabilizes |
| Infraspinatus | Infraspinous fossa | Middle facet, greater tubercle | Suprascapular (C5,C6) | Lateral rotation; stabilizes |
| Teres minor | Lateral border of scapula | Inferior facet, greater tubercle | Axillary (C5,C6) | Lateral rotation; stabilizes |
| Subscapularis | Subscapular fossa | Lesser tubercle | Subscapular (C5,C6) | Medial rotation; stabilizes |
Key MS-1 Exam Points
- Rotator cuff = SITS (Supraspinatus, Infraspinatus, Teres minor, Subscapularis)
- All four insert at or near the tubercles of the humerus and blend with the joint capsule
- Supraspinatus is the most commonly injured - passes through the tight subacromial space
- All three posterior rotator cuff muscles insert on the greater tubercle (sup to inf: Supraspinatus > Infraspinatus > Teres minor); subscapularis inserts on the lesser tubercle
- Quadrangular space carries the axillary nerve and posterior circumflex humeral artery
- Triangular space carries the circumflex scapular artery
- Triangular interval carries the radial nerve and profunda brachii artery
- The long head of triceps is the key muscle that separates the triangular space (medial to it) from the triangular interval (lateral to it)
- The axillary nerve wraps around the surgical neck of humerus - at risk in proximal humeral fractures and shoulder dislocations
- Suprascapular nerve passes under the superior transverse scapular ligament (artery passes over it - "army over the bridge") to reach supraspinatus, then through spinoglenoid notch to infraspinatus
Explain the topic nerve fibres their properties and classification, nerve degeneration and regeneration and neuropathy and synapse w.r.t. Guyton & Hall or Sherlock. MS1 level.
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
I now have all the material I need for a thorough MS-1 level explanation. Let me compile the full answer:
Nerve Fibres: Properties, Classification, Degeneration, Regeneration, Neuropathy, and Synapse
Primary source: Guyton and Hall Textbook of Medical Physiology (14th Ed); supplemented by Bradley and Daroff's Neurology, Morgan and Mikhail's Clinical Anesthesiology, and Bradley's Neurology in Clinical Practice
Part 1: Nerve Fibres - Structure and Properties
Basic Structure of a Peripheral Nerve Fibre
A nerve fibre consists of:
- Axon - the conducting process of the neuron
- Myelin sheath (in myelinated fibres) - formed by Schwann cells in the PNS (oligodendrocytes in CNS)
- Nodes of Ranvier - gaps in the myelin sheath at 1-2 mm intervals
- Endoneurium - connective tissue surrounding each fibre
- Perineurium - surrounds a fascicle (bundle of fibres)
- Epineurium - surrounds the entire nerve
Key Properties of Nerve Fibres
| Property | Myelinated | Unmyelinated |
|---|---|---|
| Conduction | Saltatory (node-to-node) | Continuous |
| Velocity | Fast (up to 120 m/s) | Slow (0.5-2 m/s) |
| Energy | Less (fewer ion movements) | More |
| Diameter | Larger | Smaller |
| Examples | Motor, touch, proprioception | Pain (slow), autonomic |
Saltatory conduction in myelinated fibres: The action potential "jumps" from one node of Ranvier to the next, which is both faster and more energy-efficient than continuous conduction because Na+/K+ exchange only occurs at the nodes.
Part 2: Classification of Nerve Fibres
There are two systems in common use.
System 1: Erlanger-Gasser Classification (A, B, C) - used for all fibres
| Fibre Type | Modality | Diameter (µm) | Velocity (m/s) | Myelinated? |
|---|---|---|---|---|
| Aα | Motor efferent; Proprioception | 12-20 | 70-120 | Yes |
| Aβ | Touch, pressure | 5-12 | 30-70 | Yes |
| Aγ | Motor (muscle spindle - fusimotor) | 3-6 | 15-30 | Yes |
| Aδ | Pain (fast/sharp), Temperature, Touch | 2-5 | 12-30 | Yes (thinly) |
| B | Preganglionic autonomic | <3 | 3-14 | Lightly |
| C (dorsal root) | Pain (slow/burning), Temperature | 0.4-1.2 | 0.5-2 | No |
| C (sympathetic) | Postganglionic sympathetic | 0.3-1.3 | 0.7-2.3 | No |
Source: Morgan and Mikhail's Clinical Anesthesiology, Table 16-1
Key Rule: Larger diameter = faster conduction velocity = less sensitive to local anaesthetics (compared to same type). Exception: small unmyelinated C fibres are relatively resistant to local anaesthetics compared to larger myelinated fibres.
System 2: Numerical Classification (I, II, III, IV) - used for sensory fibres only
| Number | Same as | Sensory Modality |
|---|---|---|
| Ia | Aα | Muscle spindle primary afferents (annulospiral endings) |
| Ib | Aα | Golgi tendon organs |
| II | Aβ | Muscle spindle secondary afferents; touch, pressure |
| III | Aδ | Sharp pain, cold temperature, crude touch |
| IV | C | Dull/burning pain, warm temperature, itch |
Mnemonic for speed order: Aα > Aβ > Aγ > Aδ > B > C
Part 3: Nerve Degeneration
Three patterns of peripheral nerve degeneration occur in response to injury or disease:
1. Segmental (Focal) Demyelination
- Occurs with mild compressive or traction force
- The axon is intact - only the myelin sheath of one or more internodes is damaged
- Segments distal and proximal to injury are not affected
- Result: widened node of Ranvier → slowing of conduction velocity across the segment
- May cause asynchronous conduction → paresthesia, loss of vibration sense, reduced reflexes
- More severe compression → conduction block → weakness or sensory loss
- Recovery: Full remyelination by Schwann cell division within weeks to months; new sheath is thinner with more internodes
2. Wallerian Degeneration
Follows axonotmesis (grade II-V injuries: axon is cut but connective tissue sheath may be intact). Named after Augustus Waller (1850).
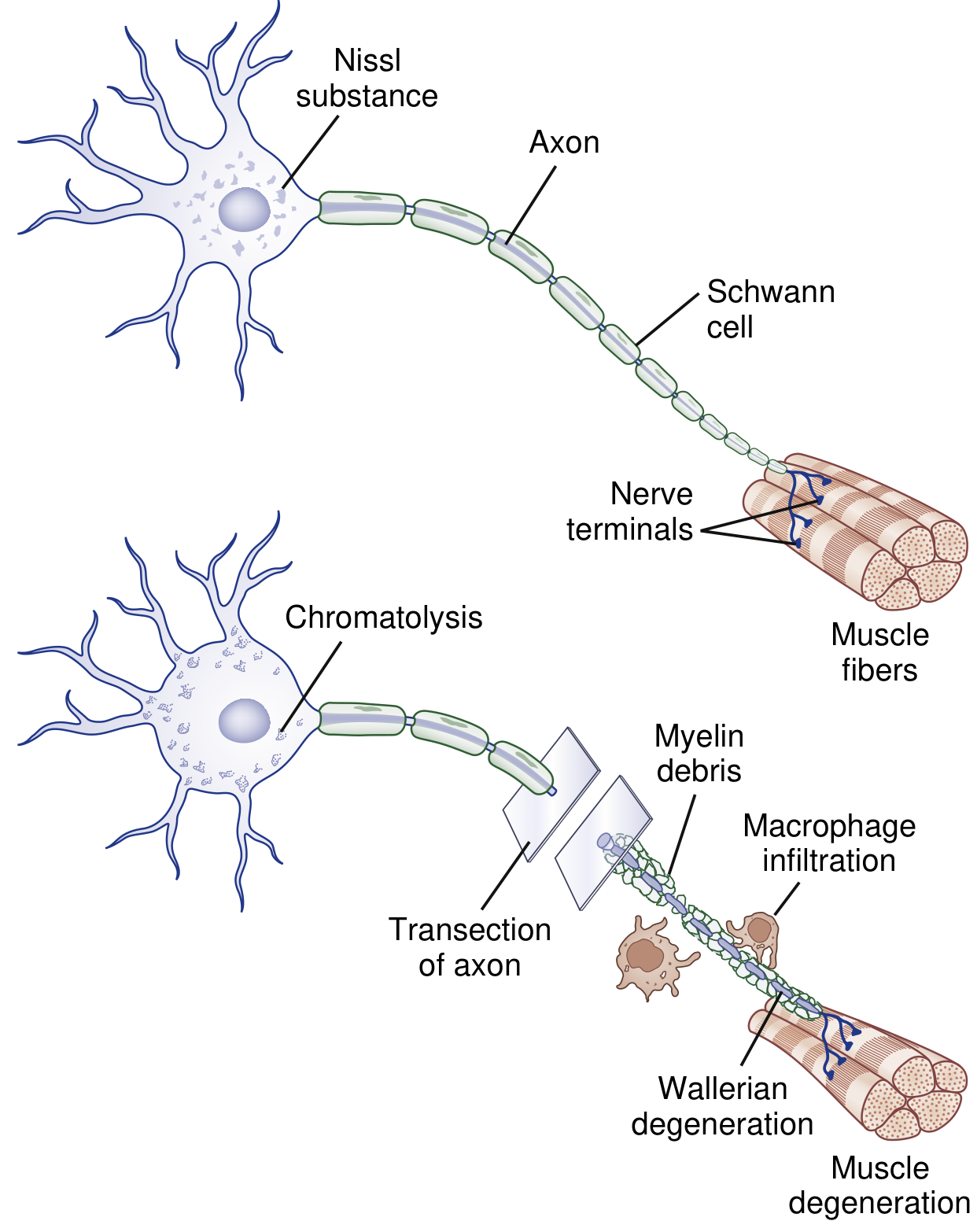
Changes DISTAL to the injury:
- Day 1-2: Disruption of retrograde and anterograde axonal flow; influx of Ca²+ and Na+ through damaged axonal membrane activates proteolytic cascades
- Day 3: Schwann cells retract from nodes of Ranvier; activated Schwann cells and macrophages begin digesting myelin
- ~1 week: Complete degeneration of the distal axon and its myelin ("myelin debris") - the entire process takes approximately 1 week
- Denervated muscle begins to atrophy
Changes PROXIMAL to the injury:
- Limited degree of axon breakdown up to the first node of Ranvier
- The cell body undergoes chromatolysis: dissolution and dispersal of Nissl substance (rough ER), eccentric displacement of nucleus, increased protein synthesis
- Chromatolysis represents a switch from axon maintenance to axon regeneration mode
3. Axonal Degeneration (Dying-Back Neuropathy)
- More characteristic of metabolic and toxic disorders (e.g., diabetes mellitus, renal failure, alcoholism)
- Degeneration begins at the distal end of the axon and progresses proximally ("dying back")
- Produces a length-dependent pattern: symptoms start in the feet and ascend (stocking-glove distribution)
- This is the basis of most peripheral neuropathies
Part 4: Nerve Regeneration
After Segmental Demyelination (Grade I - Neurapraxia)
- Schwann cell divides and initiates remyelination
- Recovery within weeks to a few months
- New myelin is thinner with more internodes per original internode
After Wallerian Degeneration (Grade II-V)
Two mechanisms operate:
A. Collateral Sprouting (when partial nerve injury)
- Intact adjacent axons send sprouts to reinnervate denervated muscle/skin
- Sprouts arise from nodes of Ranvier (nodal sprouts) or nerve terminals (terminal sprouts) as early as 4 days after injury
- Enlarges surviving motor units
- Clinical recovery: 3-6 months
B. Proximal-to-Distal Regeneration (after complete transection)
- Regenerating sprouts grow from the proximal stump guided by Schwann cell tubes (bands of Büngner) - Schwann cells proliferate within the endoneurial tube and align to form a scaffold
- Upregulation of c-Jun protein in Schwann cells switches them from myelination to repair mode
- Growth rate: approximately 1-3 mm/day (rule of thumb: 1 inch/month)
- New myelination occurs once the axon reaches its target
- Regeneration requires endoneurial tube continuity; neurotrophins (NGF, BDNF) guide the growing cone
- If the nerve gap is too large or connective tissue is disrupted, a neuroma forms
Rate of Regeneration and Prognosis
| Factor | Favors Recovery | Against Recovery |
|---|---|---|
| Injury grade | Grade I, II | Grade IV, V |
| Gap distance | Short (<1 cm) | Long (>3 cm) |
| Age | Young | Old |
| Injury type | Sharp laceration | Crush, avulsion |
| Time elapsed | Early | Delayed (>6 months) |
Part 5: Neuropathy
Definition
Neuropathy refers to pathological dysfunction of peripheral nerves. It may be classified by:
By Pattern:
- Mononeuropathy - single nerve affected (e.g., carpal tunnel = median nerve)
- Mononeuritis multiplex - multiple individual nerves (e.g., vasculitis, diabetes)
- Polyneuropathy - diffuse, usually symmetric (most common)
By Fibre Type Affected:
- Large fibre neuropathy - loss of vibration, proprioception, deep tendon reflexes (e.g., B12 deficiency, CIDP)
- Small fibre neuropathy - pain, temperature, autonomic dysfunction (e.g., diabetes, HIV)
By Pathology:
- Demyelinating - conduction velocity slowed (e.g., Guillain-Barré syndrome, CIDP, Charcot-Marie-Tooth type 1)
- Axonal - reduced amplitude on nerve conduction study (e.g., most toxic/metabolic neuropathies)
Common Causes (Mnemonic: DANG THERAPIST):
D - Diabetes, B - B12 deficiency, A - Alcohol, N - Neoplasm (paraprotein), G - Guillain-Barré / Genetics, T - Trauma / Toxins, H - Hereditary (CMT), E - Endocrine (hypothyroid), R - Renal failure, A - Amyloid, P - Porphyria, I - Inflammatory (vasculitis), S - Systemic (sarcoid), T - Thiamine deficiency
Electrodiagnostic Features:
| Parameter | Axonal | Demyelinating |
|---|---|---|
| Conduction velocity | Normal or mildly reduced | Significantly reduced (<70% normal) |
| Amplitude | Reduced | Normal or mildly reduced |
| Distal latency | Normal | Prolonged |
| F-waves | Normal | Prolonged |
Part 6: The Synapse
(Primary source: Guyton and Hall, Chapter 46)
Definition
The synapse is the junction point from one neuron to the next. It determines the direction signals spread through the nervous system and performs selective amplification, blocking, or channeling of signals.
Types of Synapses
1. Chemical Synapses (predominant in the human CNS)
2. Electrical Synapses
- Adjacent cells connected by gap junctions (clusters of ion channels)
- Allow free movement of ions from one cell to another
- Bidirectional transmission (unlike chemical synapses)
- Useful for coordinating large groups of neurons (synchronous firing)
- Found in visceral smooth muscle, cardiac muscle, some hypothalamic neurons
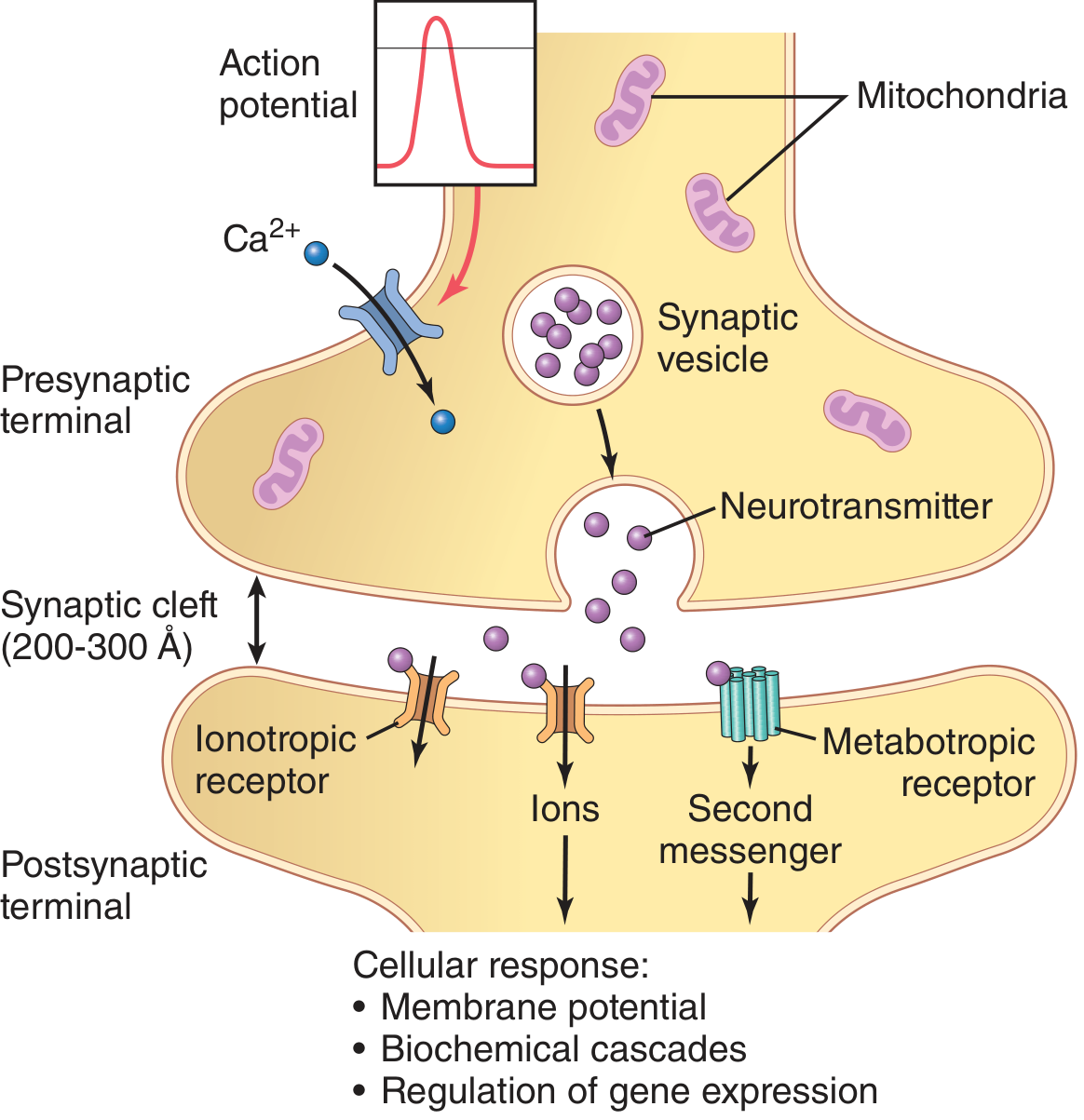
Structure of the Chemical Synapse
Presynaptic terminal (synaptic knob/bouton/end-feet):
- Separated from the postsynaptic membrane by the synaptic cleft: 200-300 Å wide
- Contains two key structures:
- Synaptic vesicles - contain neurotransmitter
- Mitochondria - provide ATP for neurotransmitter synthesis
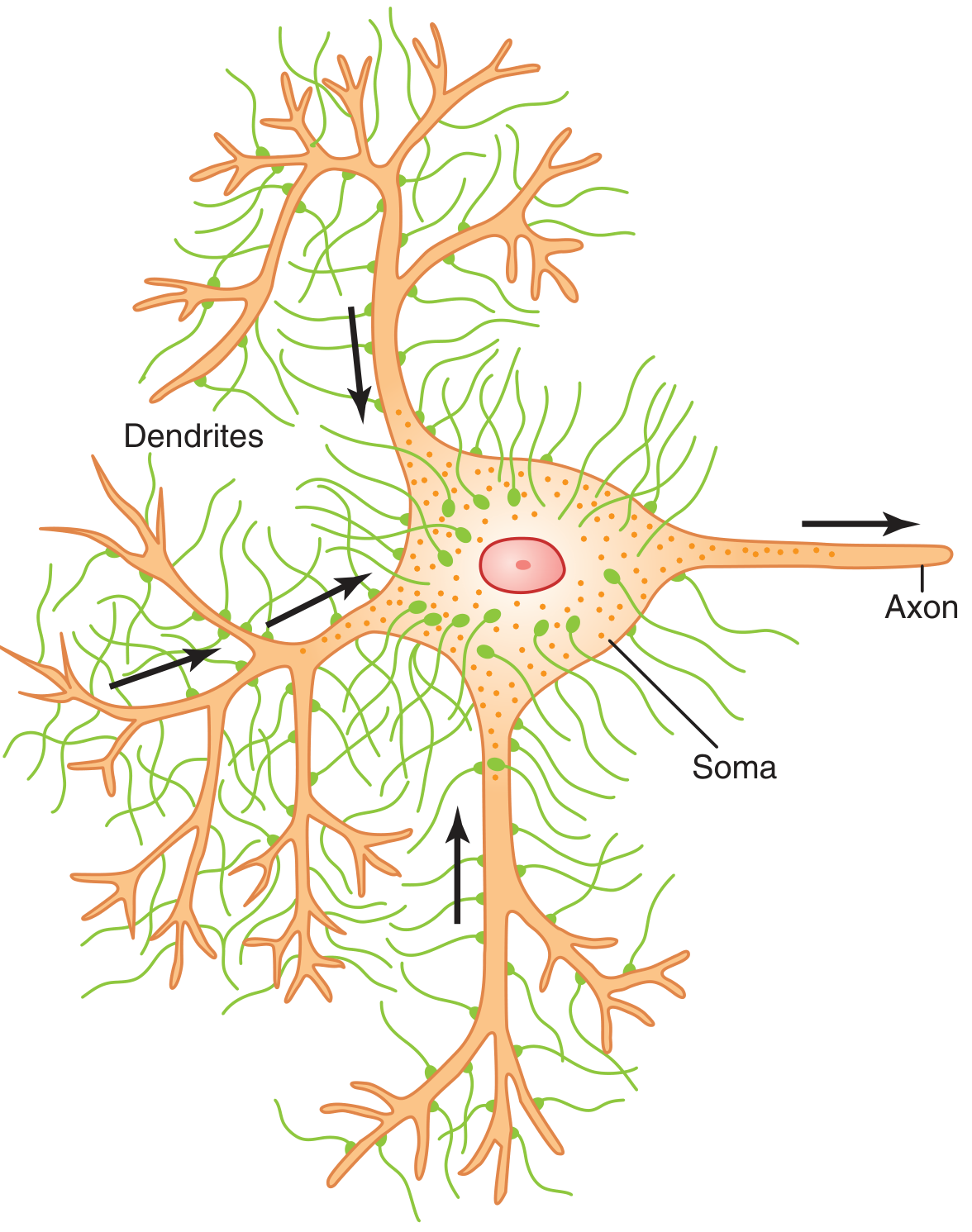
- A single anterior motor neuron can receive 10,000 to 200,000 presynaptic terminals
- 80-95% are on dendrites, only 5-20% on the soma
Mechanism of Synaptic Transmission (Step by Step)
- Action potential arrives at presynaptic terminal
- Depolarization opens voltage-gated Ca²+ channels in presynaptic membrane
- Ca²+ influx → triggers SNARE protein complex → vesicle fusion with presynaptic membrane
- Exocytosis → neurotransmitter released into synaptic cleft
- Neurotransmitter diffuses across the cleft (200-300 Å)
- Binds to postsynaptic receptors (ionotropic or metabotropic)
- Produces EPSP or IPSP depending on transmitter and receptor type
Neurotransmitters
Over 50 neurotransmitters identified. Key ones (Guyton):
- Acetylcholine (ACh) - NMJ, parasympathetic, basal forebrain
- Norepinephrine - sympathetic postganglionic, locus coeruleus
- Dopamine - substantia nigra, VTA (reward, motor control)
- Serotonin - raphe nuclei (sleep, mood)
- GABA - major inhibitory transmitter (CNS)
- Glycine - inhibitory (spinal cord)
- Glutamate - major excitatory transmitter (CNS)
- Histamine - hypothalamus (wakefulness)
Small-molecule transmitters (e.g., glutamate, ACh): stored in clear round vesicles, released rapidly.
Neuropeptide transmitters (e.g., substance P, enkephalins): synthesized in cell body, stored in dense-core vesicles, 1000x more potent, longer-lasting effects (can alter gene expression for days to months).
Postsynaptic Receptors
| Type | Mechanism | Onset | Duration | Example |
|---|---|---|---|---|
| Ionotropic | Directly opens ion channel | Fast (ms) | Brief | NMDA, AMPA, nACh receptor, GABA-A |
| Metabotropic | G-protein → second messenger cascade | Slow (sec-min) | Prolonged | mGluR, GABA-B, muscarinic, adrenergic |
Excitatory and Inhibitory Postsynaptic Potentials
EPSP (Excitatory Postsynaptic Potential):
- Produced by opening of Na+/K+ channels or closing of K+ channels
- Depolarizes the postsynaptic membrane (makes it less negative)
- Resting membrane potential of motor neuron soma = -65 mV (Guyton)
- If depolarization reaches threshold (~-45 mV), an action potential fires
IPSP (Inhibitory Postsynaptic Potential):
- Produced by opening of Cl- channels (GABA-A) or K+ channels
- Hyperpolarizes the membrane (more negative) - moves it away from threshold
- Prevents action potential generation
Summation
Since a single EPSP is usually insufficient to trigger an action potential, summation is required:
| Type | Mechanism |
|---|---|
| Spatial summation | Multiple presynaptic terminals fire simultaneously on the same neuron |
| Temporal summation | Same presynaptic terminal fires rapidly; successive EPSPs add up before the previous one decays |
"One-Way" Conduction at Chemical Synapses
Chemical synapses transmit signals only from presynaptic → postsynaptic neuron. This is because vesicles and neurotransmitter receptors are on specific sides only. This directional property allows signals to be directed toward specific targets.
Synaptic Fatigue and Facilitation
- Facilitation: Repeated stimulation → synapses become more capable of transmitting the same signal (basis of short-term memory)
- Synaptic fatigue: Depletion of neurotransmitter with rapid stimulation → declining EPSP
Summary: Key Exam Points (MS-1)
| Topic | Key Fact |
|---|---|
| Fastest nerve fibre | Aα (70-120 m/s, proprioception + motor) |
| Slowest nerve fibre | C fibres (0.5-2 m/s, dull pain) |
| Pain fibres | Aδ (sharp/fast pain) and C (slow/burning pain) |
| Saltatory conduction | Myelinated fibres only, at nodes of Ranvier |
| Chromatolysis | Cell body response to axonal injury: Nissl dissolution, eccentric nucleus |
| Wallerian degeneration | Distal to injury; complete in ~1 week |
| Regeneration rate | ~1 mm/day (1 inch/month) |
| Synaptic cleft width | 200-300 Å |
| Ca²+ in synaptic transmission | Triggers vesicle exocytosis |
| Major excitatory NT | Glutamate |
| Major inhibitory NT | GABA |
| Threshold for AP in motor neuron | ~-45 mV (resting: -65 mV per Guyton) |
| Presynaptic terminals on motor neuron | 10,000-200,000; 80-95% on dendrites |
This is a shared conversation. Sign in to Orris to start your own chat.