Hiii
Hey! How can I help you today?
I want to learn musculoskeleteal system in detail. Can you tell.me how to read to be efficent in clinical diagnosis and do not overrelg in investigation. Tell me all related clinical examination, startr from the basic to advance
Reading File
Finding Sources
Searching the Web
musculoskeletal clinical examination approach efficient diagnosis without investigations
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Here is a comprehensive, clinically oriented guide to mastering the musculoskeletal (MSK) system — built around examination-first thinking so you reduce unnecessary investigations.
🦴 Mastering the Musculoskeletal System: Clinical Examination from Basic to Advanced
Based on Harrison's Principles of Internal Medicine 22E (2025) and Sabiston Textbook of Surgery
PART 1 — How to Think & Read Efficiently
The Core Philosophy: Examine First, Investigate Second
The goal of MSK examination is to answer four questions clinically before ordering anything:
- What structure is involved? (joint, periarticular, bone, muscle, nerve)
- What is the nature of pathology? (inflammatory vs. mechanical vs. referred)
- What are the functional consequences?
- Are there systemic/extraarticular clues?
If you answer these four from the history and exam, most investigations simply confirm — they rarely change the diagnosis.
How to Read MSK Efficiently
| Study Layer | What to Learn | Resources |
|---|---|---|
| Anatomy first | Know every joint's bony landmarks, ligaments, bursae, tendons | Gray's Anatomy for Students |
| Pathology patterns | Which diseases affect which joints (DIP vs MCP vs PIP) | Harrison's Ch. 382 |
| Examination maneuvers | Sensitivity/specificity of each special test | See below |
| Clinical reasoning | Articular vs. periarticular, mono vs. poly, acute vs. chronic | Harrison's approach |
Practical tip: Learn anatomy through clinical scenarios — not in isolation. Every time you read about rotator cuff, ask: "How do I test each muscle?"
PART 2 — The Universal MSK Examination Framework
Every joint follows the same sequence: Look → Feel → Move → Special Tests
LOOK (Inspection)
- Standing: alignment, posture, muscle wasting, deformity
- Gait: antalgic (pain), Trendelenburg (hip abductor weakness), steppage (foot drop)
- Skin: erythema (inflammation/infection), pallor/ecchymosis (vascular/fracture), psoriatic plaques, tophi, nodules
- Swelling: location — articular (within joint line) vs. periarticular (beyond joint margins)
FEEL (Palpation)
- Temperature: warmth = active inflammation or infection
- Tenderness: locate precisely — joint line vs. ligament vs. tendon insertion (enthesis) vs. bursa
- Swelling character:
- Fluctuant → synovial effusion (fluid)
- Boggy/compressible like grapes → synovial hypertrophy (proliferative inflammation, e.g., RA)
- Hard as a nut → bony hypertrophy (OA)
- Crepitus: fine = normal; coarse = cartilage degeneration (OA)
- Muscle: atrophy, tenderness, trigger points
MOVE (Range of Motion)
- Active ROM first — what the patient can do voluntarily
- Passive ROM — what you can do when patient is relaxed
- Key rule: If passive > active → periarticular cause (tendon rupture, tendinitis, myopathy)
- Use a goniometer for accurate documentation
- Always compare contralaterally
Muscle Strength Grading (MRC Scale)
| Grade | Meaning |
|---|---|
| 0 | No movement |
| 1 | Visible twitch only |
| 2 | Movement with gravity eliminated |
| 3 | Movement against gravity only |
| 4 | Movement against gravity + resistance |
| 5 | Normal strength |
Assess functionally: walking, rising from chair without arms, grip strength, writing.
PART 3 — Regional MSK Examination
🖐️ HAND & WRIST
Pattern recognition — this alone guides your diagnosis:
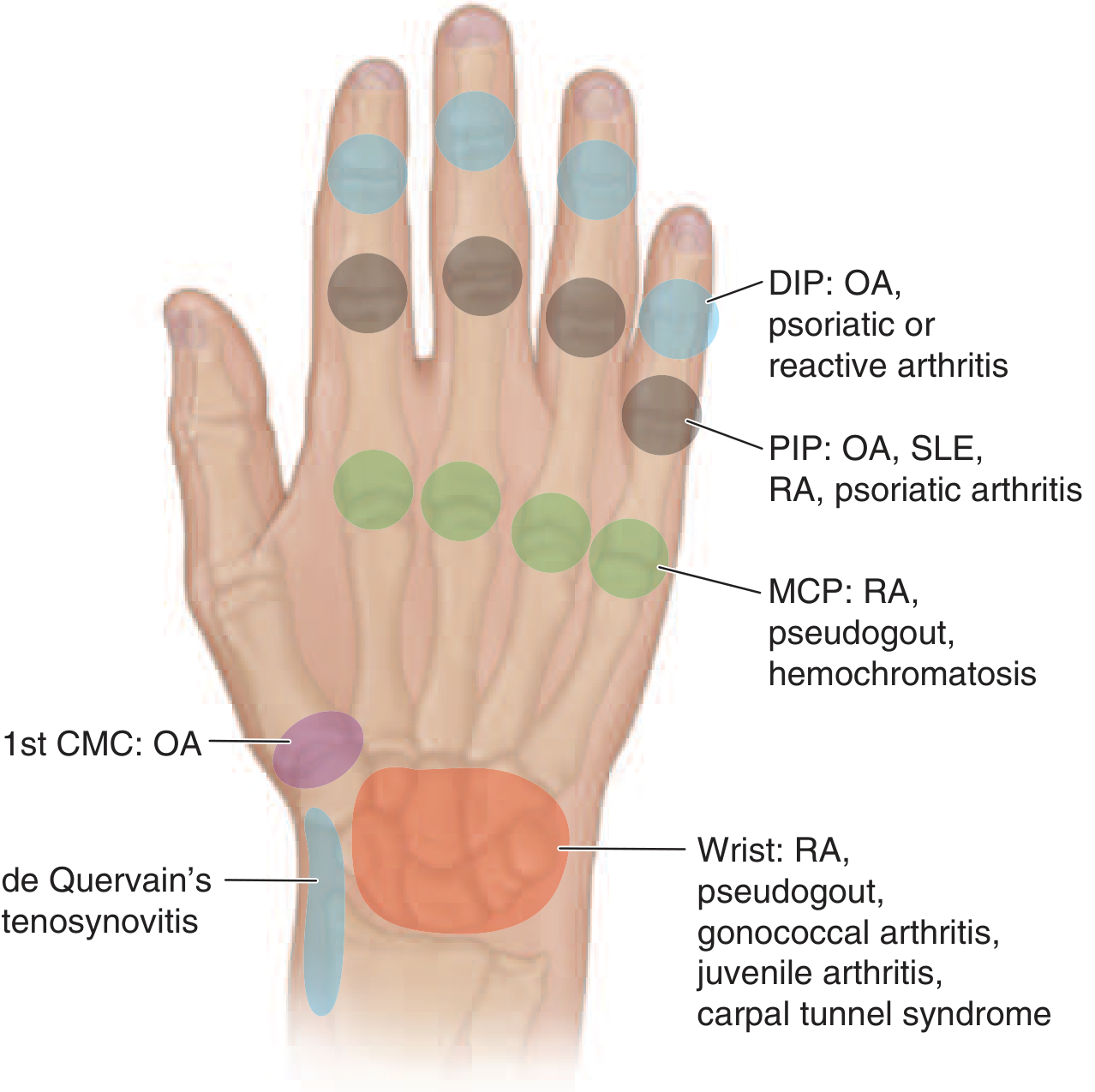
| Joint | Classic Disease |
|---|---|
| DIP | OA (Heberden's nodes), Psoriatic arthritis, Reactive arthritis |
| PIP | OA (Bouchard's nodes), RA, SLE, Psoriatic arthritis |
| MCP | RA, Pseudogout, Hemochromatosis |
| 1st CMC | OA (base of thumb pain) |
| Wrist | RA, Pseudogout, Gonococcal arthritis, Carpal tunnel syndrome |
Three screening movements (also assesses tendons + neurological):
- Make a fist → tests all finger flexors
- Thumbs-up → thumb abduction + extension (APL, EPB)
- A-OK sign → thumb opposition + intrinsic function
Key Special Tests:
| Test | What it Tests | Technique | Positive Finding |
|---|---|---|---|
| Finkelstein | De Quervain tenosynovitis | Thumb in palm, fingers wrap around, ulnar deviate wrist | Sharp radial-sided pain |
| Thumb CMC Grind | 1st CMC OA | Axial load + circumduction of thumb | Crepitus/grittiness at CMC |
| Watson Test | Scapholunate instability | Thumb over scaphoid tubercle + move wrist ulnar→radial deviation | Painful "clunk" as scaphoid subluxes |
| Tinel's Sign | Carpal tunnel (median nerve) | Tap over carpal tunnel at wrist | Tingling in median nerve distribution |
| Durkan's Test | Carpal tunnel (more sensitive) | Sustained compression over carpal tunnel for 30 sec | Paraesthesia in thumb, index, middle fingers |
Tenodesis test (for uncooperative/unconscious patients): passively extend the wrist → digits should flex automatically. Passively flex wrist → digits extend. Loss of cascade = tendon injury.
💪 SHOULDER
The shoulder has the greatest ROM of any joint — this makes it vulnerable and complex. Most "shoulder pain" is periarticular, not articular.
Key anatomy landmarks to palpate:
- Acromioclavicular (AC) joint — top of shoulder
- Bicipital groove (anterior) — biceps tendon
- Greater tuberosity — supraspinatus insertion
- Coracoid process — anterior, just below clavicle
Rotator Cuff Testing (SITS muscles):
| Muscle | Test | Technique | Positive |
|---|---|---|---|
| Supraspinatus | Empty can test (Jobe's) | Arm at 90° abduction, 30° forward, thumb down → resist downward force | Pain/weakness |
| Infraspinatus + Teres minor | External rotation lag test | Elbow at 90°, resist external rotation | Weakness = infraspinatus tear |
| Subscapularis | Lift-off test (Gerber) | Hand behind back, push away from lumbar spine | Inability = subscapularis tear |
| Subscapularis | Bear hug test | Hand on opposite shoulder, resist lift-off | Weakness = subscapularis |
Impingement Tests:
| Test | Technique | Positive |
|---|---|---|
| Neer sign | Passive forward flexion with arm pronated | Pain in anterior shoulder |
| Hawkins-Kennedy | Elbow at 90°, internally rotate while in 90° forward flexion | Pain = subacromial impingement |
AC Joint: Crossed-arm adduction test — bring arm across chest, AC pain = AC joint pathology.
Instability: Apprehension test — abduct and externally rotate arm, push humeral head anteriorly. Apprehension/pain = anterior instability.
🦵 KNEE
The knee is the most commonly examined large joint. Think in compartments: anterior, medial, lateral, posterior.
Effusion detection:
- Bulge sign (small effusion): Milk fluid from medial pouch proximally, tap lateral side → medial bulge visible
- Patella Ballottement (large effusion): Press patella downward — it "bounces" back
Ligament Testing:
| Test | Ligament | Technique | Positive |
|---|---|---|---|
| Anterior Drawer | ACL | Knee flexed 90°, foot stabilized, pull tibia anteriorly | >5mm anterior displacement |
| Posterior Drawer | PCL | Same position, push tibia posteriorly | Posterior displacement |
| Lachman test | ACL (more sensitive) | 30° knee flexion, stabilize femur, translate tibia anteriorly | Soft endpoint, anterior shift |
| Valgus stress | MCL | Knee slightly flexed, apply valgus force | Pain/laxity = MCL injury |
| Varus stress | LCL | Apply varus force | Pain/laxity = LCL injury |
Meniscus Testing:
| Test | Technique | Positive |
|---|---|---|
| McMurray | Flex knee to 90°, extend while rotating tibia medially (lateral meniscus) or laterally (medial meniscus) | Painful click |
| Joint line tenderness | Palpate medial/lateral joint line with knee flexed 90°, foot on table | Localized tenderness |
| Thessaly test | Patient stands on one leg, knee bent 20°, rotates body medially/laterally | Medial/lateral pain = meniscus |
Patellofemoral:
- Clarke's test: Press patella distally while patient contracts quads → pain = chondromalacia patellae
- J-sign: Watch patellar tracking during knee extension — lateral deviation = maltracking
Bursae (commonly missed!):
- Prepatellar bursa: Anterior to patella ("housemaid's knee")
- Infrapatellar bursa: Below patellar ligament
- Pes anserine bursa: Medial proximal tibia — often missed; tender in obese patients + OA + fibromyalgia
🦴 HIP
The hip is deceptive — "hip pain" is frequently not from the hip joint.
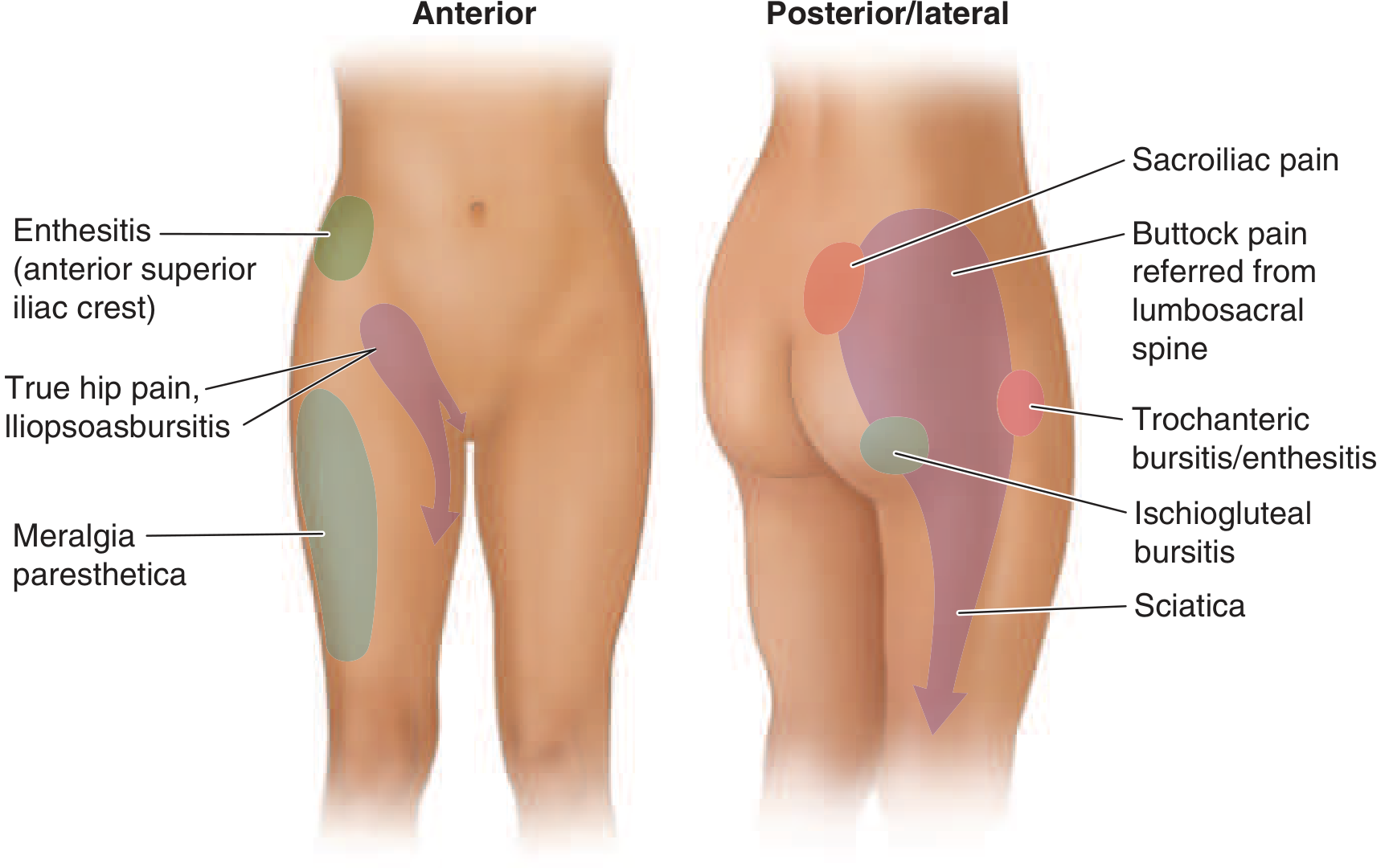
Localizing hip pain clinically:
| Location | Likely Source |
|---|---|
| Groin / anteromedial thigh | True hip joint (OA), iliopsoas bursitis |
| Lateral thigh below greater trochanter | Trochanteric bursitis / IT band |
| Posterior gluteal → posterolateral leg → foot | Sciatica (L4-S1), lumbosacral disk disease |
| Anterior lateral thigh (burning/numbness) | Meralgia paresthetica (lateral femoral cutaneous nerve) |
| Sitting pain (ischium) | Ischiogluteal bursitis |
| Buttock + morning stiffness + age <40 | Sacroiliac joint (ankylosing spondylitis) |
Key Hip Tests:
| Test | What it Tests | Technique | Positive |
|---|---|---|---|
| FABER (Patrick's test) | Hip joint, SI joint | Flex, Abduct, Externally Rotate hip (figure-4 position) | Groin pain = hip; posterior pain = SI joint |
| FADIR | Impingement / labral tear | Flex, ADduct, Internally Rotate | Groin pain = femoroacetabular impingement |
| Trendelenburg test | Hip abductor weakness (gluteus medius) | Patient stands on one leg; observe contralateral pelvis | Contralateral pelvis drops = positive |
| Thomas test | Hip flexion contracture | Patient supine, flex one hip to chest; observe opposite thigh | If opposite thigh rises off table = flexion contracture |
| Log roll test | Hip joint irritability | Rotate leg internally/externally | Pain in groin = intraarticular pathology |
🔙 SPINE (Low Back)
Observation + neurological level is the key, not imaging.
Lumbar Exam:
- Inspect: loss of lordosis, scoliosis, muscle spasm
- Palpate: spinous processes, paraspinal muscles, SI joints
- ROM: flexion (touch toes), extension, lateral flexion, rotation
Nerve Root Testing:
| Root | Motor | Reflex | Sensory |
|---|---|---|---|
| L3 | Knee extension (quads) | Knee jerk | Anterior thigh |
| L4 | Ankle dorsiflexion | Knee jerk | Medial lower leg |
| L5 | Hallux extension (EHL) | None reliable | Dorsum of foot |
| S1 | Plantar flexion (walk on toes) | Ankle jerk | Lateral foot |
Key Tests:
| Test | Technique | Positive |
|---|---|---|
| Straight Leg Raise (SLR) | Leg straight, dorsiflex foot, raise to 30–70° | Lancinating pain below knee = nerve root compression (L4-S1) |
| Crossed SLR | Raise opposite leg | Pain on symptomatic side = large central/paracentral disk herniation |
| Femoral Stretch Test | Prone, flex knee → extend hip | Anterior thigh pain = L2-L4 nerve root |
| FABER | As above | Posterior pain = SI joint |
| Schober's test | Mark L5 + 10cm above; measure on forward flexion | <15cm total = restricted lumbar flexion (ankylosing spondylitis) |
PART 4 — Articular vs. Periarticular: The Critical Distinction
This single distinction saves the most investigations:
| Feature | Articular | Periarticular |
|---|---|---|
| Pain distribution | Diffuse, all around joint | Focal, one side |
| Swelling | Within joint margins | Extends beyond joint |
| ROM limitation | Active AND passive | Active > Passive |
| Examples | OA, RA, gout, septic | Tendinitis, bursitis, enthesitis |
Rule: If passive ROM is full and pain-free but active ROM is limited/painful → the problem is periarticular (tendon, bursa, muscle). Investigations for joint pathology will be unhelpful.
PART 5 — Inflammatory vs. Mechanical: The Second Key Distinction
| Feature | Inflammatory | Mechanical |
|---|---|---|
| Morning stiffness | >60 minutes | <30 minutes |
| Rest | Worsens pain (gelling) | Relieves pain |
| Activity | Improves pain | Worsens pain |
| Systemic features | Fatigue, fever, weight loss | Absent |
| Joint findings | Warm, boggy, symmetric | Cool, bony, asymmetric |
PART 6 — When to Investigate (and When NOT to)
Investigate ONLY when the exam cannot answer the question:
| Clinical Scenario | Warranted Investigation |
|---|---|
| Acute monoarthritis → septic arthritis suspected | Arthrocentesis (synovial fluid) — mandatory |
| Inflammatory polyarthritis, new onset | RF, anti-CCP, ANA, ESR, CRP |
| Red flag back pain (fever, weight loss, age >50, night pain) | X-ray spine, ESR, PSA, SPEP |
| Cruciate ligament tear suspected | MRI knee (after clinical diagnosis established) |
| True hip joint OA suspected | X-ray pelvis (AP + lateral) |
Do NOT investigate when:
- Clinical exam clearly identifies a periarticular cause (tendinitis, bursitis) → treat first
- Chronic mechanical low back pain without neurological signs → imaging rarely changes management
- Effusion is small and clearly reactive → aspirate only if septic arthritis cannot be excluded
PART 7 — The 28-Joint Count (For Inflammatory Arthritis)
Harrison's recommends examining these 28 joints to quantify active inflammation in RA monitoring:
- 10 PIPs (fingers 2–5, bilateral)
- 10 MCPs (fingers 1–5, bilateral)
- 2 Wrists
- 2 Elbows
- 2 Shoulders
- 2 Knees
Score = number of tender + swollen joints (each counted separately, max 28 each).
PART 8 — Study Roadmap (Basic → Advanced)
LEVEL 1 (Basic)
├── Anatomy: bones, joints, muscles per region (Gray's)
├── Screening: GALS (Gait, Arms, Legs, Spine) screen
└── Vocabulary: articular vs. periarticular, mono vs. poly, acute vs. chronic
LEVEL 2 (Intermediate)
├── Regional examination: Hand, Shoulder, Knee, Hip, Spine
├── Special tests: learn 2-3 per joint with sensitivity/specificity
└── Pattern recognition: which diseases affect which joints
LEVEL 3 (Advanced)
├── Combined maneuvers + clinical reasoning
├── Neurological correlation (nerve roots, entrapments)
├── Systemic MSK disease (RA, SpA, crystal arthropathies, vasculitis)
└── Functional assessment + outcome measures (VAS, HAQ, DAS28)
Quick Reference: Red Flags in MSK
🚨 Never miss these:
- Hot, swollen, single joint → Septic arthritis until proven otherwise (arthrocentesis)
- Back pain + night sweats + weight loss → Malignancy / TB spine
- Hip pain in child + fever + limp → Septic arthritis / Perthe's disease
- Acute joint pain after intercourse in young adult → Gonococcal arthritis
- Jaw claudication + scalp tenderness + ESR >50 → Giant cell arteritis (temporal arteritis)
Sources: Harrison's Principles of Internal Medicine, 22nd Ed. (2025), McGraw-Hill — Chapter 382 (Musculoskeletal Examination and Regional Rheumatic Complaints); Sabiston Textbook of Surgery (Hand & Wrist Examination)
Ok now provide the content to study level i.e. baiscs of anatomy
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Searching Images
types of synovial joints classification hinge ball socket pivot
Loading Image
Searching Images
bone structure compact spongy periosteum cortex medullary cavity
You've run out of free credits. Sign up for a free account to continue using Orris.
This is a shared conversation. Sign in to Orris to start your own chat.