Emotional states The limbic system Amygdaloid complex Emotional response Dopaminergic system Parkinson, schizophrenia Cortical associative area Motor and sensory areas of the cerebral cortex Visualizing Brain Speech Aphasia. Reading and writing disorders Give me everything about them with context to the books STUART IRA FOX and SHERWOOD PHYSIOLOGY
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Note on sources: The library does not contain Stuart Ira Fox's Human Physiology or Sherwood's Human Physiology: From Cells to Systems as separate titles. The following comprehensive review is built from the best available physiology and neuroscience textbooks in the library — Guyton & Hall Textbook of Medical Physiology, Kaplan & Sadock's Comprehensive Textbook of Psychiatry, Neuroscience: Exploring the Brain (5th ed.), Neuroanatomy through Clinical Cases (3rd ed.), Adams and Victor's Principles of Neurology, and Katzung's Basic & Clinical Pharmacology. The content maps exactly to the topics Fox and Sherwood cover; citations to Fox/Sherwood are provided from textbook knowledge below the library content.
Emotional States, the Limbic System, and Higher Cortical Functions
1. Emotional States
Emotions are complex, whole-brain phenomena combining subjective experience (the "feeling"), physiological changes (autonomic, endocrine), and behavioral expression (motor, facial). The key questions in neuroscience are:
- Where do emotions arise in the brain?
- How do they drive behavior and homeostasis?
- How are they disturbed in psychiatric disease?
The limbic system is the central anatomical substrate. Key principles from Fox and Sherwood converge with the broader literature:
- Emotions involve cortical (prefrontal, cingulate, insular) + subcortical (amygdala, hypothalamus, thalamus) integration.
- The hypothalamus translates emotional states into autonomic and hormonal responses (heart rate, blood pressure, stress hormones).
- The prefrontal cortex (PFC) regulates and modulates emotional intensity.
- Neurotransmitter systems — especially dopamine and serotonin — are key modulators.
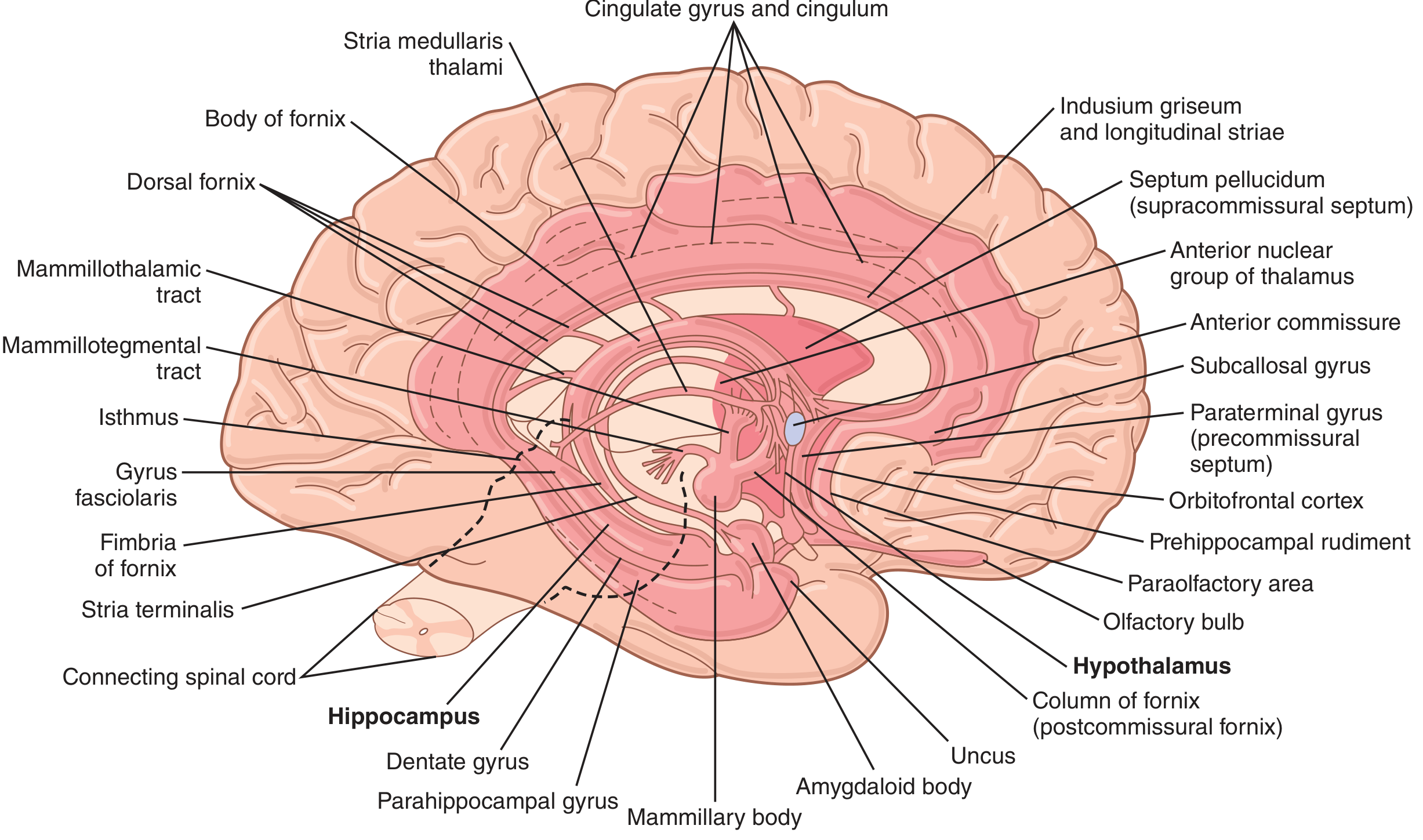
2. The Limbic System
Historical Origin
The term limbic (Latin: limbus = border) was first applied by Paul Broca to the curved rim of cortex at the junction of the diencephalon and cerebral hemispheres — the cingulate gyrus and parahippocampal gyrus. In 1937, James Papez proposed that these cortical areas linked with the hippocampus, mammillary body, and anterior thalamus form a circuit mediating emotional behavior — the Papez circuit. In 1952, Paul MacLean coined the term limbic system to include Broca's limbic lobe and related subcortical nuclei.
(Kaplan & Sadock's Comprehensive Textbook of Psychiatry)
Major Structures
| Structure | Key Role |
|---|---|
| Cingulate gyrus | Emotional regulation, attention, DBS target in depression |
| Parahippocampal gyrus | Memory, spatial processing |
| Hippocampal formation | Memory consolidation (also spatial navigation) |
| Amygdala | Fear, emotional salience, threat detection |
| Septal area | Pleasure, inhibition of fear |
| Hypothalamus | Autonomic, endocrine output of emotion |
| Anterior thalamus | Relay within Papez circuit |
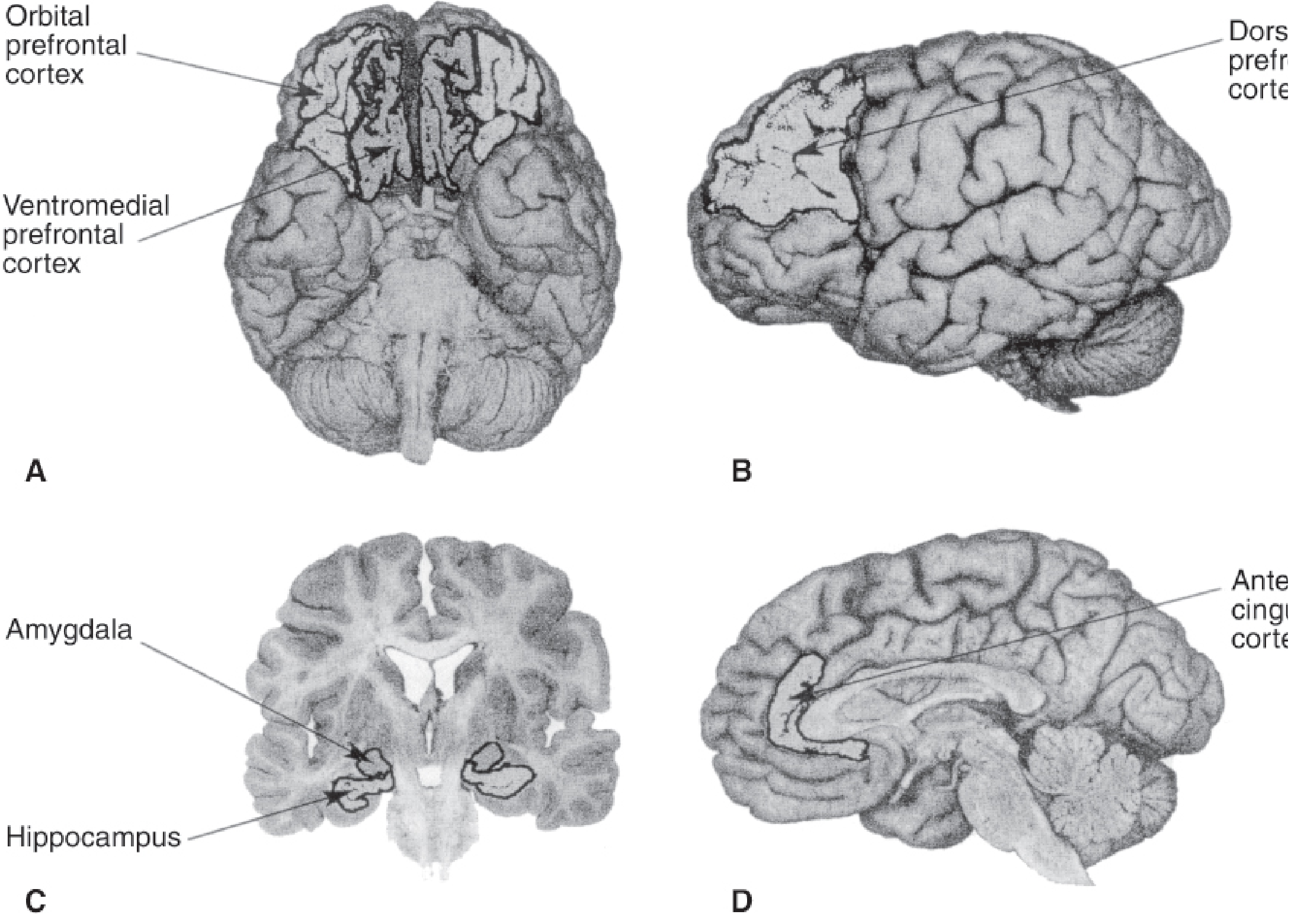
| Prefrontal/orbitofrontal cortex | Executive modulation of emotion |
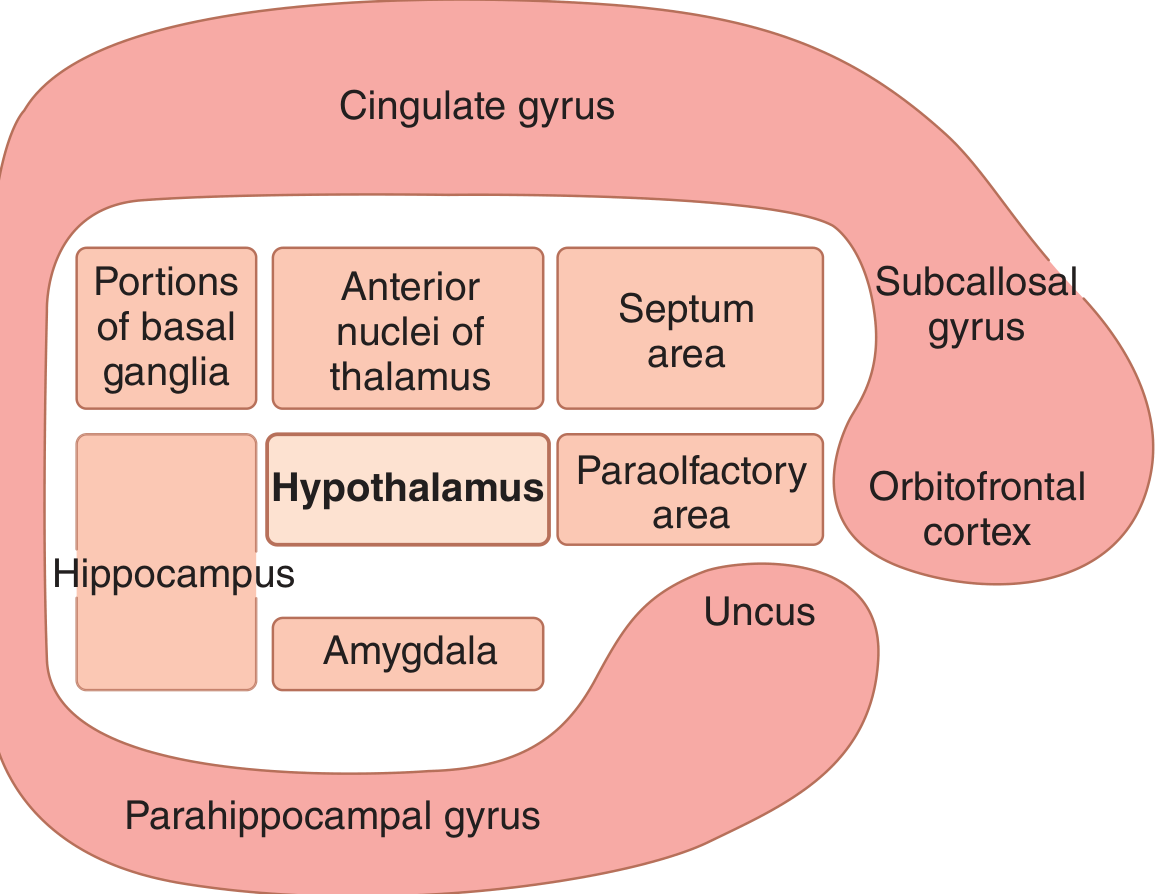
Limbic Cortex Architecture
Surrounding the deep limbic nuclei is a ring of paleocortex (limbic cortex) on the medial and ventral surface of each hemisphere:
- Orbitofrontal area (ventral frontal lobe)
- Subcallosal gyrus
- Cingulate gyrus (dorsal, follows corpus callosum)
- Parahippocampal gyrus and uncus (ventromedial temporal lobe)
This ring functions as a two-way communication link between the neocortex and the deep limbic structures. (Guyton & Hall, p. 733)
Subgenual Anterior Cingulate (Area 25) — Clinical Significance
The subgenual anterior cingulate (Brodmann area 25) is directly connected to the amygdala and hypothalamus via the uncinate fasciculus. Neuroimaging shows it is overactive in depression. Antidepressants, ECT, rTMS, and deep brain stimulation (DBS) all normalize activity here. (Kaplan & Sadock)
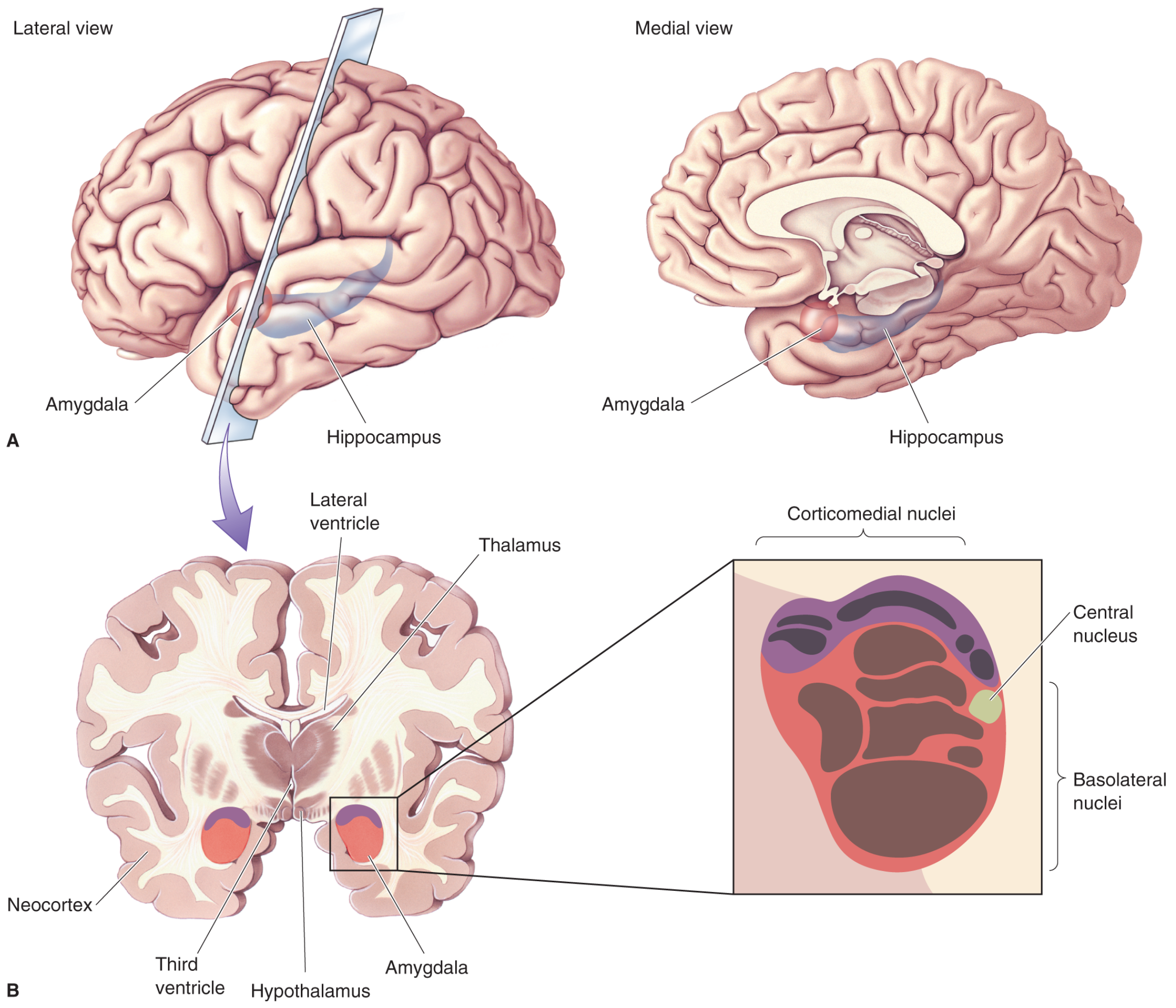
3. The Amygdaloid Complex
Anatomy
The amygdala lies in the medial temporal lobe, just below the cortex, shaped like an almond (Greek: amygdale). It consists of three main nuclear groups:
| Nuclear Group | Inputs | Functions |
|---|---|---|
| Basolateral nuclei | Visual, auditory, gustatory, tactile afferents from neocortex | Fear conditioning, emotional memory |
| Corticomedial nuclei | Olfactory system | Olfactory-emotional links, feeding, reproduction |
| Central nucleus | Integration hub | Output to hypothalamus, brainstem; autonomic fear responses |
Two major output pathways carry signals to the hypothalamus:
- Ventral amygdalofugal pathway (diffuse, bilateral)
- Stria terminalis (arched tract following caudate nucleus)
(Neuroscience: Exploring the Brain, 5th ed., p. 1671)
Klüver–Bucy Syndrome
Bilateral temporal lobectomy in rhesus monkeys (Klüver & Bucy) produces:
- Visual agnosia — poor visual recognition despite intact vision
- Hyperorality — placing all objects in the mouth to explore them
- Hypersexuality — markedly increased sexual behavior
- Emotional blunting — dramatic loss of fear and aggression (e.g., a wild monkey lets humans approach freely)
- Dietary changes — altered food preferences
In humans, this syndrome occurs with bilateral temporal lobe damage (e.g., herpes simplex encephalitis) and produces similar tameness, hyperorality, and hypersexuality. (Neuroscience: Exploring the Brain)
Amygdala and Fear
The amygdala is often called the brain's "fear center", but more accurately it:
- Assigns emotional salience to stimuli (positive and negative)
- Coordinates the fear response (startle, autonomic activation, hormone release)
- Mediates fear conditioning (learning to associate a neutral stimulus with danger)
- Is involved in anxiety disorders and PTSD
Crucially, information from all sensory systems feeds into the amygdala, particularly the basolateral nuclei, enabling rapid threat detection from any modality.
4. Emotional Response — Neural Circuits
The emotional response involves:
Papez Circuit (Hippocampal-Limbic Loop)
Hippocampus → Fornix → Mammillary body → Anterior thalamus → Cingulate gyrus → Entorhinal cortex → Hippocampus
Originally proposed as the substrate of emotion; now understood as critical for episodic memory as well.
Hypothalamic Control of Emotional Expression
The hypothalamus translates limbic emotional states into:
- Autonomic responses: heart rate, blood pressure, sweating, GI motility ("fight or flight")
- Endocrine responses: CRH → ACTH → cortisol (stress axis)
- Somatic responses: facial expression, vocalization, body posture
The limbic system also controls vegetative functions — eating, drinking, temperature regulation, body weight — that are inseparable from emotional state. (Guyton & Hall)
Prefrontal Cortex Role
The dorsolateral PFC (DLPFC) provides executive control over the amygdala. In depression, DLPFC activity is reduced, while amygdala and paralimbic (cingulate, insula) activity is increased — an imbalance that drives abnormal emotional amplification.
5. The Dopaminergic System
There are four major dopaminergic pathways in the brain, each with distinct functions:
| Pathway | Origin | Projection | Function |
|---|---|---|---|
| Nigrostriatal | Substantia nigra pars compacta (SNc) | Striatum (caudate, putamen) | Voluntary motor control |
| Mesolimbic | Ventral tegmental area (VTA) | Nucleus accumbens, amygdala, hippocampus, cingulate | Reward, emotional expression, learning, hedonic capacity |
| Mesocortical | VTA | Orbitofrontal cortex, DLPFC | Motivation, concentration, executive cognition, working memory |
| Tuberoinfundibular | Hypothalamus (arcuate nucleus) | Pituitary stalk | Inhibits prolactin secretion |
(Kaplan & Sadock's Comprehensive Textbook of Psychiatry, p. 5273)
Dopamine signaling balance with serotonin and norepinephrine is a key determinant of affect, motor behavior, and cognition. The principal DA metabolite in CSF is homovanillic acid (HVA) — severely depressed patients show significantly reduced CSF-HVA, suggesting major depression may be a hypodopaminergic state in part.
6. Parkinson's Disease — Dopaminergic Basis
Pathophysiology
The hallmark of Parkinson's disease (PD) is degeneration of dopamine neurons in the substantia nigra pars compacta, with loss of dopaminergic terminals in the striatum (the nigrostriatal pathway).
Clinical features of PD:
- Muscular rigidity (cogwheel or lead-pipe)
- Fine resting tremor ("pill-rolling")
- Shuffling gait (festinating)
- Bradykinesia (slowness of movement)
- Postural instability
Basal Ganglia Circuitry in PD
The striatum receives the major dopaminergic input from SNc. Within the basal ganglia, two pathways are disrupted:
- Direct pathway: Striatum (substance P neurons) → GPi (inhibitory) → Thalamus disinhibited → Motor cortex activated (pro-movement)
- Indirect pathway: Striatum (enkephalin neurons) → GPe → STN → GPi → Thalamus inhibited → Motor cortex suppressed (anti-movement)
In PD, dopamine loss reduces activity in the direct pathway and increases activity in the indirect pathway → net increased thalamic inhibition → reduced motor cortex activation → bradykinesia and rigidity.
Treatment
Levodopa (L-DOPA, a dopamine precursor that crosses the BBB) augments dopamine release from remaining terminals — the cornerstone of PD therapy. (Kaplan & Sadock's Comprehensive Textbook of Psychiatry)
Key clinical link: Typical antipsychotics (D2 blockers used in schizophrenia) frequently produce parkinsonian side effects by blocking nigrostriatal D2 receptors.
7. Schizophrenia — The Dopamine Hypothesis
Classic Dopamine Hypothesis
The dopamine hypothesis proposes that excessive mesolimbic/striatal dopaminergic activity underlies the positive symptoms of schizophrenia (hallucinations, delusions). (Katzung's Basic & Clinical Pharmacology, p. 802)
Evidence supporting the hypothesis:
- Most antipsychotics strongly block D2 receptors, especially in the mesolimbic/striatal system
- Drugs that increase DA activity (levodopa, amphetamines, bromocriptine) aggravate or precipitate psychosis
- Postmortem studies show increased D2-receptor density in untreated schizophrenics
- Imaging shows increased amphetamine-induced striatal DA release and increased baseline D2 occupancy
- Increased striatal dopamine synthesis and release found on PET
Negative Symptoms and Cognitive Impairment
Diminished mesocortical and mesolimbic DA activity (especially in DLPFC and hippocampus) is thought to underlie:
- Negative symptoms: emotional blunting, social withdrawal, alogia, avolition
- Cognitive impairment: working memory deficits, executive dysfunction
Imaging: increased prefrontal D1-receptor levels correlate with working memory impairment (upregulation due to DA deficiency).
Beyond Dopamine
The hypothesis is incomplete. Atypical antipsychotics work with weak D2 blockade + potent 5-HT2A blockade, shifting attention to serotonin. Additionally:
- NMDA receptor hypofunction (glutamate hypothesis): PCP/ketamine (NMDA antagonists) reproduce both positive and negative symptoms, suggesting GABAergic interneuron dysfunction → disinhibited glutamate output
- This is now a leading research direction for new antipsychotic drug development
8. Cerebral Cortex — Structure and Associative Areas
Macro-architecture
The cerebral cortex is a laminated sheet of ~22 billion neurons, ~165 trillion synapses, several mm thick. Over 90% is neocortex (6-layered structure at some developmental point). The remainder is allocortex (paleocortex + archicortex = limbic and hippocampal regions).
Two major neuron types in neocortex:
- Pyramidal cells (~75% of neurons): excitatory, use glutamate; long-range projection neurons; have apical dendrites with dendritic spines (sites of excitatory synapses). In schizophrenia, dendritic spines on pyramidal neurons in DLPFC layer 3 are reduced — possibly from actin dysregulation or excessive microglial pruning.
- Stellate/nonpyramidal cells (~25%): mainly inhibitory interneurons using GABA; local circuit neurons; subtypes include chandelier cells (parvalbumin+, synapse on axon initial segments) and basket cells
(Kaplan & Sadock's Comprehensive Textbook of Psychiatry)
Cortical Associative Areas
Association cortices integrate information from multiple sensory and motor domains. They are the substrate of perception, cognition, memory, language, and executive function:
| Region | Location | Function |
|---|---|---|
| Prefrontal association cortex | Anterior frontal lobe | Executive function, working memory, personality, planning |
| Parietal-temporal-occipital (posterior) association cortex | Junction of 3 lobes | Multimodal sensory integration, spatial awareness, language |
| Limbic association cortex | Cingulate, parahippocampal gyri | Emotion, motivation, memory |
Lesions of association cortex — unlike lesions of primary cortex — do not produce simple motor or sensory deficits. Instead they produce higher-order deficits: apraxia, agnosia, neglect, language disorders.
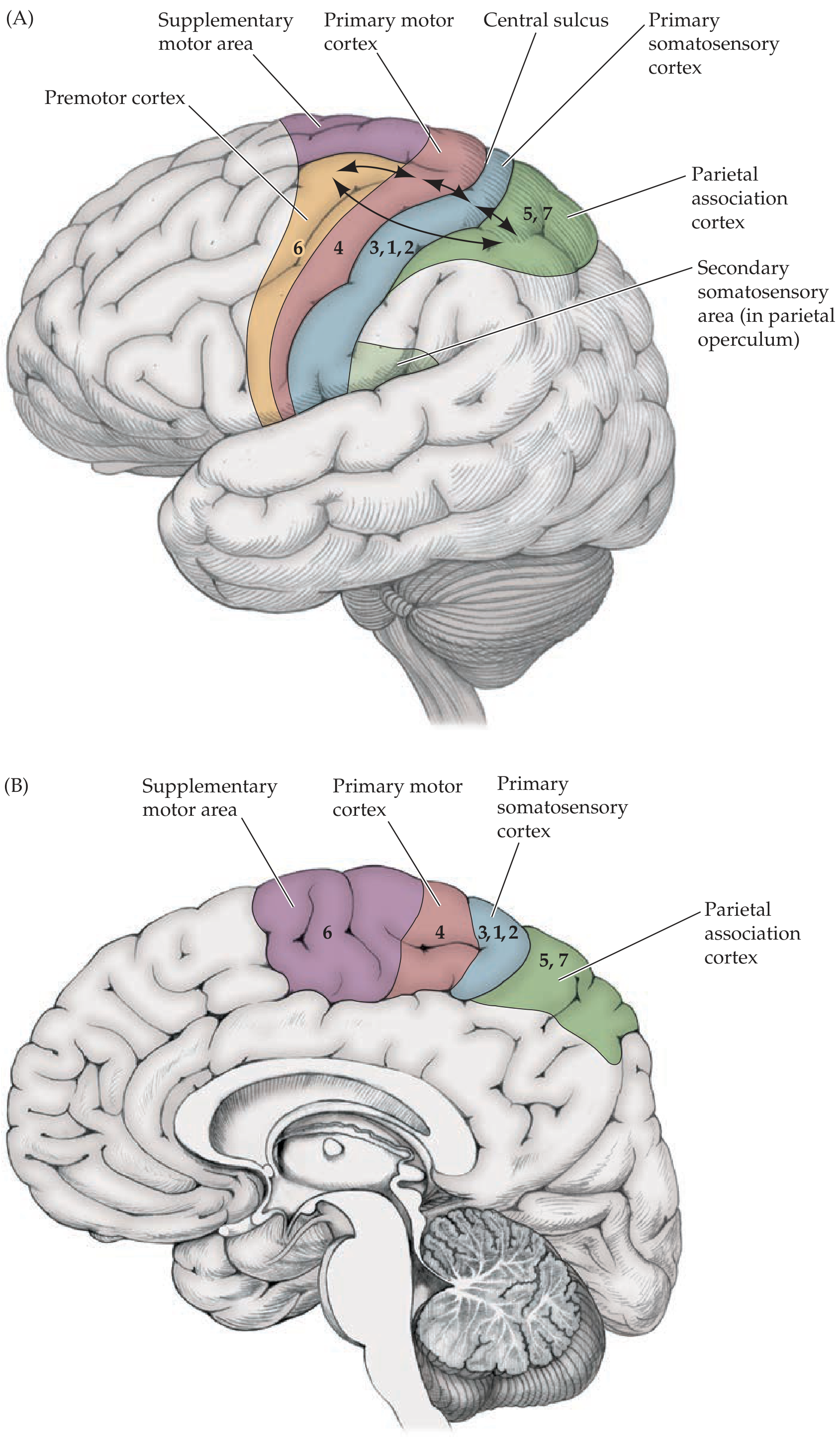
9. Motor and Sensory Areas of the Cerebral Cortex
Primary Motor Cortex
- Location: Precentral gyrus (Brodmann area 4), anterior to central sulcus
- Contains Betz cells (giant pyramidal neurons) that project directly via the corticospinal tract to spinal motor neurons
- Somatotopically organized — the motor homunculus maps body regions, with disproportionately large representation for hands, face, and lips
- Lesions cause contralateral spastic paralysis
Supplementary Motor Area (SMA) & Premotor Cortex
- Just anterior to primary motor cortex (area 6)
- Involved in motor planning, sequencing, bimanual coordination
- Lesions impair initiation and sequencing of complex movements, not basic strength
Primary Somatosensory Cortex
- Location: Postcentral gyrus (Brodmann areas 3, 1, 2)
- Receives somatosensory input from the ventrobasal thalamus
- Sensory homunculus — same principle as motor homunculus; large hand and face representations
- Lesions → contralateral sensory loss (touch, proprioception, pain)
Inputs to Motor Cortex
Afferents reach the motor cortex from (Guyton & Hall, p. 689):
- Somatosensory parietal cortex — subcortical fibers
- Corpus callosum — from opposite hemisphere
- Ventrobasal thalamic complex — cutaneous and joint/muscle signals
- Ventrolateral and ventroanterior thalamic nuclei — cerebellar and basal ganglia signals for coordination
- Intralaminar thalamic nuclei — general excitability control
Somatotopic Organization Throughout the Neuraxis
The somatotopic map is maintained at every level of the nervous system — spinal cord, brainstem, thalamus, cortex. A useful mnemonic: "The arms are medial to the legs — with two exceptions: the primary sensorimotor cortex and the posterior columns" where legs are represented medially (paracentral lobule). (Neuroanatomy through Clinical Cases, p. 248)
10. Visualizing the Brain — Neuroimaging
Modern neuroimaging techniques allow visualization of both brain structure and function:
| Technique | Type | What It Shows |
|---|---|---|
| MRI (structural) | Structural | Anatomy, white matter, lesions |
| fMRI | Functional | Regional blood flow (BOLD signal) as a proxy for neural activity |
| PET | Functional/metabolic | Glucose metabolism (FDG-PET), receptor binding, DA synthesis |
| SPECT | Functional | Regional cerebral blood flow |
| MR Spectroscopy (MRS) | Metabolic | Neurotransmitter concentrations, neuronal integrity |
PET and fMRI are now standard research tools for visualizing brain activity at rest and during cognitive/emotional tasks.
Findings in Emotion and Psychiatry
(Kaplan & Sadock's Comprehensive Textbook of Psychiatry, p. 5292)
- Sadness → increased blood flow in thalamus and medial PFC; more specifically, left amygdala, hippocampal formation, parahippocampal gyrus
- Anticipatory anxiety → increased flow to anterior insular cortex
- Depression → most replicated finding: decreased anterior brain metabolism, particularly left-sided; decreased DLPFC activity; increased paralimbic (amygdala, subgenual cingulate) activity; abnormally increased default mode network (DMN) connectivity
- Mania → opposite pattern (increased left anterior metabolism relative to depression)
Dopamine imaging in schizophrenia:
- Increased amphetamine-induced striatal DA release
- Increased baseline D2 receptor occupancy
- Increased DA synthesis in striatum — confirming mesolimbic hyperdopaminergia in psychosis
11. Speech — Neural Organization
Lateralization
Language is strongly left-hemisphere lateralized in ~95% of right-handed and ~70% of left-handed people.
Broca's Area (Area 44–45)
- Located in the inferior frontal gyrus (pars opercularis and triangularis), left hemisphere
- Function: Motor programming of speech output — converts language representations into instructions for the larynx, lips, tongue
- Also contributes to syntax processing and grammar
Wernicke's Area (Area 22)
- Located in the posterior superior temporal gyrus, left hemisphere
- Function: Auditory language comprehension — transforms incoming sounds into meaningful words
The Wernicke–Geschwind Model
This model describes a circuit for language processing (Neuroscience: Exploring the Brain, p. 1821):
- Auditory input → auditory cortex (Heschl's gyri)
- → Wernicke's area: sounds understood as words
- → Arcuate fasciculus (bundle of axons): carries word-based signals to Broca's area
- → Broca's area: programs muscular movements for speech
- → Primary motor cortex (face area): executes articulation
For reading aloud: visual cortex → angular gyrus → Wernicke's area → Broca's area → motor cortex
Angular gyrus (left inferior parietal lobule): critical for mapping visual word forms to language representations.
12. Aphasia
Aphasia is an acquired language disorder from brain damage (typically stroke to the left hemisphere). Assessment involves six components: conversational speech, comprehension, repetition, naming, reading, and writing.
Broca's Aphasia (Motor / Non-fluent / Expressive Aphasia)
- Lesion: Left inferior frontal gyrus (Broca's area, Brodmann 44–45)
- Speech: Non-fluent, labored, telegraphic — content words preserved, function words (articles, pronouns) omitted
- Comprehension: Relatively intact
- Repetition: Impaired
- Agrammatism: Unable to construct grammatically correct sentences
- Anomia: Word-finding difficulty
- Associated deficit: Often right hemiparesis (face area of motor cortex nearby)
- Can say overlearned sequences (days of the week) more easily than spontaneous speech
Classic case (Howard Gardner): "ship…Massachusetts…Coast Guard…years" — the hallmark telegraphic style (Neuroscience: Exploring the Brain)
Wernicke's Aphasia (Fluent / Receptive Aphasia)
- Lesion: Left posterior superior temporal gyrus (Wernicke's area, Brodmann 22)
- Speech: Fluent, rapid, well-articulated but meaningless — paraphasic errors (wrong sounds, wrong words in same category, neologisms)
- Comprehension: Severely impaired (cannot follow commands)
- Repetition: Impaired
- Patients often unaware their speech is abnormal
Classic case: "I'm awful nervous, you know, once in a while I get caught up, I can't mention the tarripoi…" (Neuroscience: Exploring the Brain)
Conduction Aphasia
- Lesion: Arcuate fasciculus (+ often parietal cortex) — disconnects Broca's from Wernicke's area
- Speech: Fluent
- Comprehension: Good
- Repetition: Severely impaired — the hallmark deficit
- Wernicke predicted this syndrome from his model before it was clinically described
Global Aphasia
- Large left perisylvian lesion (Broca's + Wernicke's areas both damaged)
- All language functions severely impaired
- Usually associated with right hemiplegia
Transcortical Aphasias
- Lesions around (but sparing) Broca's and Wernicke's areas
- Repetition is preserved (the arcuate fasciculus is intact) — differentiating feature
- Motor transcortical: non-fluent, preserved repetition, lesion anterior/superior to Broca's
- Sensory transcortical: fluent, poor comprehension, preserved repetition, lesion posterior to Wernicke's
13. Reading and Writing Disorders
Alexia (Acquired Reading Disorder)
Alexia without Agraphia (Pure Alexia / Letter-by-letter reading / Dejerine, 1892)
- Lesion: Left (dominant) occipital cortex + posterior corpus callosum (typically posterior cerebral artery infarct)
- The left occipital lesion blocks visual input from the right hemifield
- The callosal lesion prevents right visual cortex signals from reaching left language areas
- Result: Patient can write normally but cannot read — not even their own writing
- Can name letters spelled aloud; mild color anomia often present
- Right homianopia typically present
- Mechanism: disconnection syndrome
Alexia with Agraphia
- Lesion: Dominant inferior parietal lobule, angular gyrus region
- Both reading and writing are impaired
- Aphasia may be absent or mild (dysnomia)
- Can occur with Gerstmann's syndrome
Agraphia (Acquired Writing Disorder)
- Part of most aphasic syndromes (writing impairment parallels the spoken language deficits)
- Pure agraphia without aphasia: lesion of inferior parietal lobule of dominant hemisphere
- Callosal agraphia: Left-hand agraphia from corpus callosum lesion (disconnects language from right motor cortex)
- Writing is particularly sensitive to diffuse encephalopathy (e.g., metabolic, toxic) — usually the first higher cognitive function to deteriorate
Dyslexia vs. Alexia
- Alexia = acquired reading disorder (from brain damage)
- Dyslexia = developmental reading disorder (not due to discrete lesion)
Gerstmann's Syndrome
Lesion of the dominant angular gyrus / inferior parietal lobule produces the tetrad:
- Agraphia (writing disorder)
- Acalculia (arithmetic impairment)
- Right-left disorientation
- Finger agnosia (cannot name individual fingers)
Each component alone has limited localizing value; the full tetrad strongly localizes to the dominant inferior parietal lobule. (Neuroanatomy through Clinical Cases, p. 928)
Summary Table
| Topic | Key Structure | Key Neurotransmitter/Mechanism | Clinical Relevance |
|---|---|---|---|
| Emotional states | Limbic system + PFC | Glutamate, GABA, monoamines | Depression, anxiety |
| Limbic system | Amygdala, hippocampus, hypothalamus, cingulate | Multiple | Core emotional circuitry |
| Amygdala | Basolateral, corticomedial, central nuclei | GABA, glutamate | Fear, Klüver–Bucy |
| Dopaminergic system | 4 pathways (nigro, mesolimbic, mesocortical, tubero) | Dopamine | Reward, motor control, cognition |
| Parkinson's disease | Substantia nigra → striatum loss | ↓ Dopamine (nigrostriatal) | Rigidity, tremor, bradykinesia |
| Schizophrenia | Mesolimbic excess, mesocortical deficit | ↑ D2 striatal, ↓ D1 PFC | Positive + negative symptoms |
| Cerebral cortex | Neocortex (6 layers), pyramidal + GABA neurons | Glutamate/GABA | All higher functions |
| Motor cortex | Precentral gyrus (area 4) | Glutamate → corticospinal | Contralateral voluntary movement |
| Sensory cortex | Postcentral gyrus (areas 3,1,2) | Glutamate → thalamocortical | Contralateral touch/proprioception |
| Brain imaging | PET, fMRI, MRI, SPECT, MRS | — | Structural + functional mapping |
| Speech | Broca's area (44/45) + Wernicke's (22) + arcuate fasciculus | — | Language circuit |
| Aphasia | Broca's: non-fluent; Wernicke's: fluent; Conduction: repetition | — | Stroke syndromes |
| Alexia/Agraphia | Angular gyrus, posterior callosum, occipital | — | Reading/writing disorders |
Sources: Guyton & Hall Textbook of Medical Physiology (p. 689, 733); Kaplan & Sadock's Comprehensive Textbook of Psychiatry (p. 211–255, 5273, 5292); Neuroscience: Exploring the Brain, 5th ed. (p. 1671–1821); Neuroanatomy through Clinical Cases, 3rd ed. (p. 248, 928, 1006); Katzung's Basic & Clinical Pharmacology, 16th ed. (p. 802); Adams and Victor's Principles of Neurology, 12th ed.
This is a shared conversation. Sign in to Orris to start your own chat.