Explain me how to analyse ecg from basic to advanced with all conditions along with proper diagrams
Reading File
Finding Sources
Finding Sources
Searching the Web
ECG interpretation guide basic to advanced with diagrams all conditions
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Finding Sources
Finding Sources
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Finding Sources
I now have comprehensive content from multiple authoritative textbooks and real ECG images. Let me compile the complete guide.
Complete ECG Analysis Guide: Basic to Advanced
Sources: Medical Physiology (Boron & Boulpaep), Goldman-Cecil Medicine, Braunwald's Heart Disease, Rosen's Emergency Medicine, Frameworks for Internal Medicine, Harrison's Principles of Internal Medicine 22E, Ganong's Review of Medical Physiology
PART 1 - THE BASICS: Understanding the ECG
What is an ECG?
An ECG (electrocardiogram) provides a direct measurement of the rate, rhythm, and time-dependent electrical vector of the heart. It records the time versus amplitude of electrical projections and represents the heart's conduction system. Because different parts of the heart activate sequentially, we can attribute time-dependent changes in the electrical vector to different regions.
- P wave - atrial depolarization
- QRS complex - ventricular depolarization
- T wave - ventricular repolarization
- U wave - delayed repolarization of Purkinje fibers (may be seen in hypokalemia)
(Medical Physiology, Boron & Boulpaep)
The ECG Paper
ECG paper uses a standard grid:
- Vertical axis: 0.1 mV per mm
- Horizontal axis: 0.04 seconds per small box (1 mm), 0.2 seconds per large box (5 mm)
- 5 large boxes = 1 second
At the standard paper speed of 25 mm/s:
| Box Size | Width | Time |
|---|---|---|
| Small (1 mm) | - | 0.04 sec |
| Large (5 mm) | - | 0.20 sec |
The 12 Leads: What Each Sees
A 12-lead ECG uses 10 electrodes to generate 12 views of the heart from different angles:
Limb Leads (Frontal Plane)
| Lead | View |
|---|---|
| I | Lateral (0°) |
| II | Inferior (60°) |
| III | Inferior (120°) |
| aVR | Cavity/right (-150°) |
| aVL | Lateral (-30°) |
| aVF | Inferior (90°) |
Precordial Leads (Horizontal Plane)
| Lead | Position | View |
|---|---|---|
| V1 | Right sternal border, 4th ICS | Septal/RV |
| V2 | Left sternal border, 4th ICS | Septal |
| V3 | Between V2 and V4 | Anterior |
| V4 | Midclavicular line, 5th ICS | Anterior |
| V5 | Anterior axillary line | Lateral |
| V6 | Midaxillary line | Lateral |
Coronary territory localization:
| Leads with Changes | Territory | Artery |
|---|---|---|
| V1-V4 | Anterior | LAD |
| I, aVL, V5-V6 | Lateral | LCx |
| II, III, aVF | Inferior | RCA |
| V1-V2 (tall R, ST depression) | Posterior | RCA/LCx |
| V3R-V4R | Right ventricle | RCA |
PART 2 - THE SYSTEMATIC APPROACH (7-Step Method)
Always read every ECG using the same sequence. Never skip steps.
Step 1 - Rate
Direct method: Count seconds between two R waves (R-R interval). Heart rate = 60 / R-R interval in seconds.
Quick method (for regular rhythms):
Count large boxes between R waves and use the "300 rule":
| Large Boxes (R-R) | Heart Rate |
|---|---|
| 1 | 300 bpm |
| 2 | 150 bpm |
| 3 | 100 bpm |
| 4 | 75 bpm |
| 5 | 60 bpm |
| 6 | 50 bpm |
For irregular rhythms: Count QRS complexes in a 10-second rhythm strip and multiply by 6.
- Normal: 60-100 bpm
- Bradycardia: < 60 bpm
- Tachycardia: > 100 bpm
Step 2 - Rhythm
Ask four questions:
- Is there a P wave before every QRS?
- Is there a QRS after every P wave?
- Are P-P intervals regular?
- Are R-R intervals regular?
Normal sinus rhythm requires:
- P wave before each QRS
- P wave upright in leads II, III, aVF
- PR interval 0.12-0.20 sec
- Regular rate 60-100 bpm
Step 3 - Axis
The normal QRS axis lies between -30° and +90°.
Quick method - look at leads I and aVF:
| Lead I | aVF | Axis |
|---|---|---|
| Positive (up) | Positive (up) | Normal (0° to +90°) |
| Positive (up) | Negative (down) | Left axis deviation (LAD) |
| Negative (down) | Positive (up) | Right axis deviation (RAD) |
| Negative (down) | Negative (down) | Extreme (Northwest) axis |
Causes of LAD: LBBB, left anterior fascicular block, inferior MI, LVH, WPW
Causes of RAD: RBBB, left posterior fascicular block, RVH, lateral MI, PE, WPW
Step 4 - Intervals
| Interval | Normal | Meaning |
|---|---|---|
| PR interval | 0.12-0.20 sec (3-5 small boxes) | AV conduction time |
| QRS duration | < 0.12 sec (< 3 small boxes) | Ventricular depolarization |
| QT interval | Varies with rate; corrected QTc < 450 ms (men), < 470 ms (women) | Ventricular action potential duration |
| QTc formula | QT / √(R-R interval in seconds) | Bazett's formula |
Step 5 - P Waves and Atrial Enlargement
Normal P wave: < 0.12 sec wide, < 2.5 mm tall, upright in I and II, biphasic in V1
| Finding | Meaning |
|---|---|
| Tall peaked P > 2.5 mm in II | Right atrial enlargement ("P pulmonale") |
| Wide notched P > 0.12 sec in II | Left atrial enlargement ("P mitrale") |
| Biphasic P in V1 with large terminal negative component | Left atrial enlargement |
Step 6 - QRS Complex
Normal Q waves: Small septal q waves in I, aVL, V5-V6 (< 1 small box wide, < 25% height of R wave)
Pathological Q waves: > 1 mm wide OR > 1/3 height of QRS = old infarction (not in III and aVR where Q waves can be normal)
R wave progression: R waves should grow from V1 to V5/V6 (poor R-wave progression = anterior MI or LVH)
Step 7 - ST Segment and T Waves
| Finding | Meaning |
|---|---|
| ST elevation > 1 mm in 2+ contiguous leads | STEMI, pericarditis, Prinzmetal's angina, LV aneurysm |
| ST depression | Ischemia (NSTEMI/UA), reciprocal changes, digitalis effect |
| T wave inversion | Ischemia, strain pattern, PE, Wellens' syndrome |
| Tall peaked T waves | Hyperkalemia, hyperacute STEMI |
| Flat/inverted T waves | Hypokalemia, ischemia |
PART 3 - ARRHYTHMIAS
3.1 Sinus Arrhythmias
| Arrhythmia | Rate | Rhythm | P waves | PR | QRS |
|---|---|---|---|---|---|
| Normal sinus rhythm | 60-100 | Regular | Upright in II, before QRS | 0.12-0.20 | Normal |
| Sinus tachycardia | >100 | Regular | Normal | Normal | Normal |
| Sinus bradycardia | <60 | Regular | Normal | Normal | Normal |
| Sinus arrhythmia | 60-100 | Irregular (varies with breathing) | Normal | Normal | Normal |
| Sinus pause/arrest | Variable | Pause | Missing P | - | Missing QRS |
3.2 Atrial Arrhythmias
Below is a classic textbook ECG showing atrial extrasystole, atrial tachycardia, atrial flutter, and atrial fibrillation side by side:
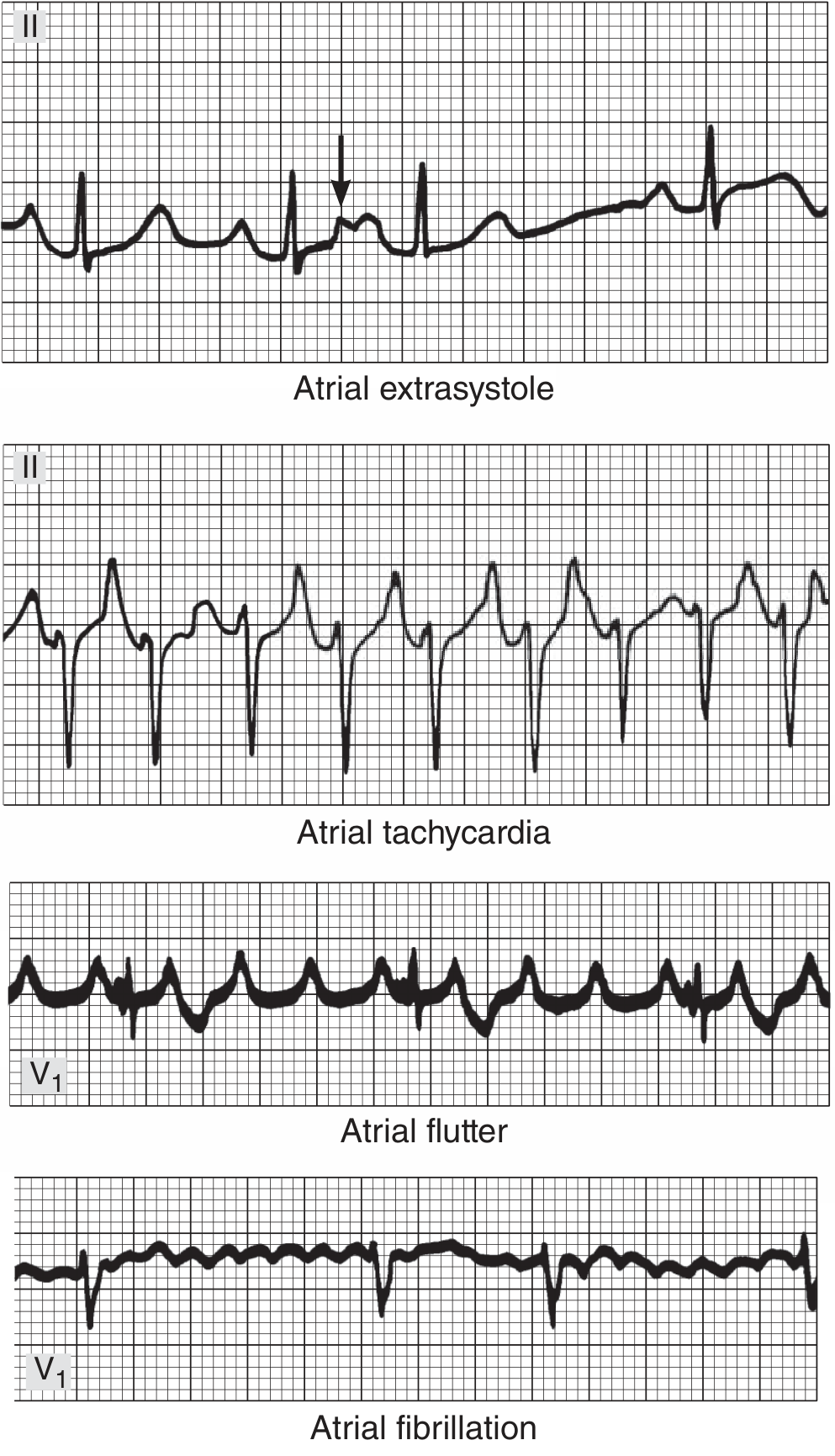
FIGURE - Atrial arrhythmias. Top to bottom: atrial extrasystole (arrow = abnormal P buried in preceding T wave); atrial tachycardia; atrial flutter with 4:1 AV block (sawtooth pattern); atrial fibrillation with totally irregular ventricular rate. (Ganong's Review of Medical Physiology)
Atrial Extrasystoles (PACs)
- Abnormal P wave morphology (ectopic atrial focus)
- QRST usually normal (same ventricular activation)
- Followed by a compensatory or non-compensatory pause
- Clinically benign in most individuals
Atrial Tachycardia
- Rate: 150-220 bpm from a single atrial focus
- P waves present but different morphology from sinus
- May have AV block (especially in digitalis toxicity)
Atrial Flutter
- Atrial rate: 200-350 bpm, typically ~300 bpm
- Classic sawtooth "flutter waves" at 300/min in leads II, III, aVF (negative) and V1 (positive)
- Usually 2:1 AV block → ventricular rate ~150 bpm (always suspect flutter when rate is exactly 150)
- Mechanism: large counterclockwise reentrant circuit in right atrium around cavo-tricuspid isthmus
The stress test below shows the natural progression from sinus tachycardia → rapid AF → 2:1 atrial flutter → AF → sinus rhythm:
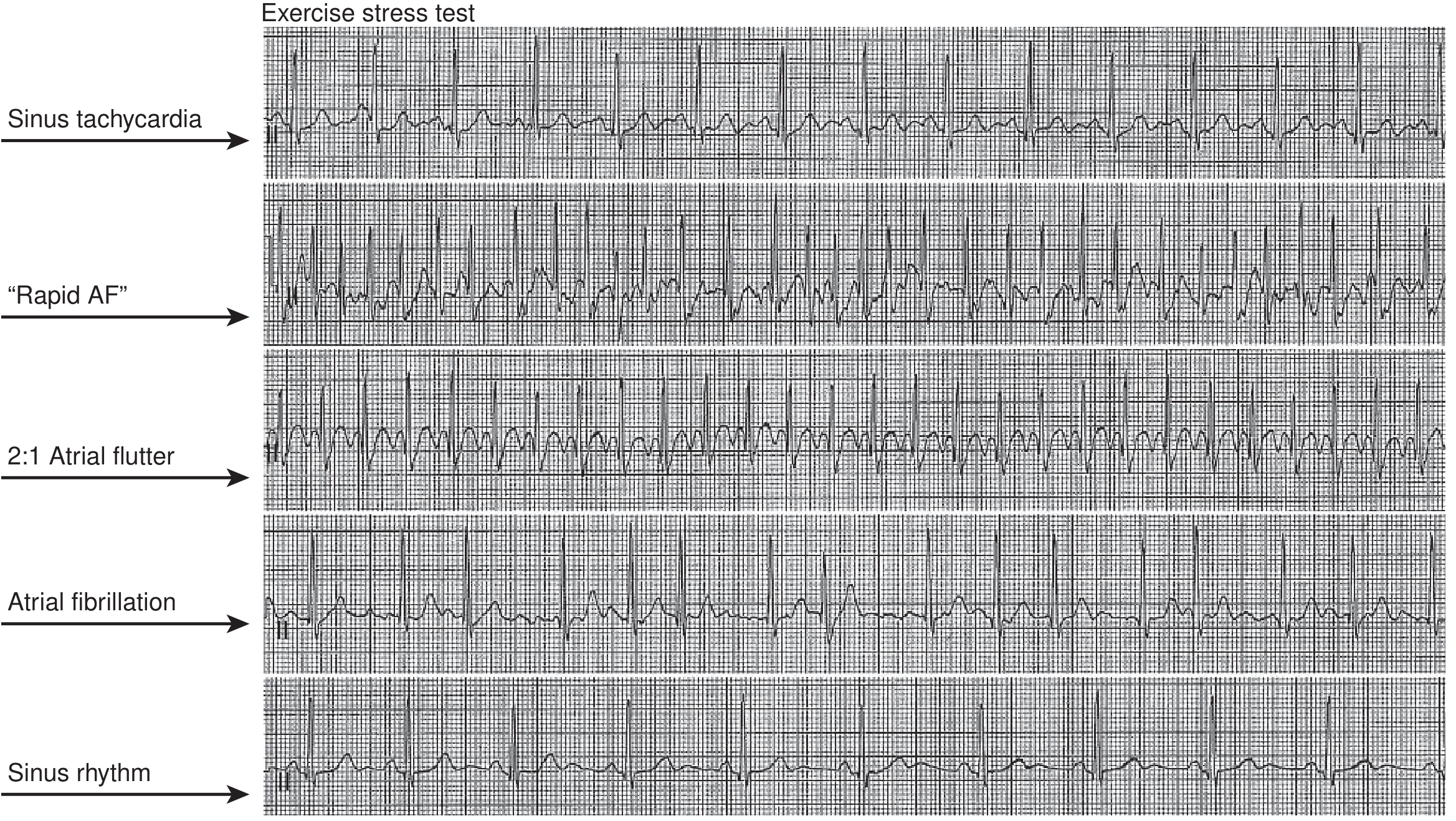
FIGURE - Exercise stress test showing sinus tachycardia, rapid AF, 2:1 atrial flutter, AF, and spontaneous return to sinus rhythm. (Braunwald's Heart Disease)
Atrial Fibrillation (AF)
- Atrial rate: 300-500/min, completely irregular and disorganized
- No distinct P waves - replaced by fibrillatory baseline
- Irregularly irregular R-R intervals (pathognomonic)
- Ventricular rate: 80-160 bpm
- Mechanism: multiple concurrent reentrant excitation waves in both atria; some paroxysmal AF from ectopic foci in pulmonary veins (Ganong's Review of Medical Physiology)
3.3 AV Nodal Arrhythmias
AVNRT (AV Nodal Reentrant Tachycardia)
- Most common SVT
- Rate: 150-250 bpm, regular
- P waves buried in or just after QRS (retrograde P, pseudo-R' in V1, pseudo-S in inferior leads)
- Narrow QRS (unless aberrant)
- Terminates with vagal maneuvers or adenosine
AVRT (AV Reentrant Tachycardia) - WPW
- Accessory pathway connects atria and ventricles
- Delta wave on baseline ECG: slurred upstroke of QRS, short PR (<0.12 sec), wide QRS
- Orthodromic AVRT: narrow complex (down accessory, up normal)
- Antidromic AVRT: wide complex (down normal, up accessory) - looks like VT!
3.4 Heart Blocks (AV Blocks)
The three general types are first-degree, second-degree, and third-degree AV block.
First-Degree AV Block
ECG finding: PR interval > 200 ms (> 1 large box), every P conducts to QRS
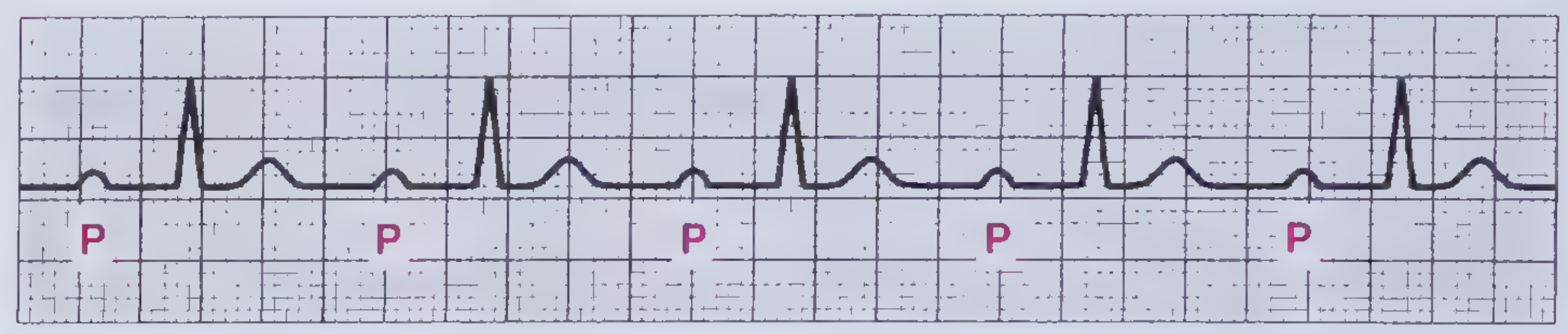
FIGURE - First-degree AV block. The PR interval is >200 ms in duration. (Frameworks for Internal Medicine)
- Generally benign
- Causes: inferior MI, increased vagal tone, digoxin, electrolyte abnormalities
- No treatment needed for isolated first-degree block
Second-Degree AV Block - Mobitz Type I (Wenckebach)
ECG findings: Progressively lengthening PR intervals until a QRS is dropped, then the cycle resets.
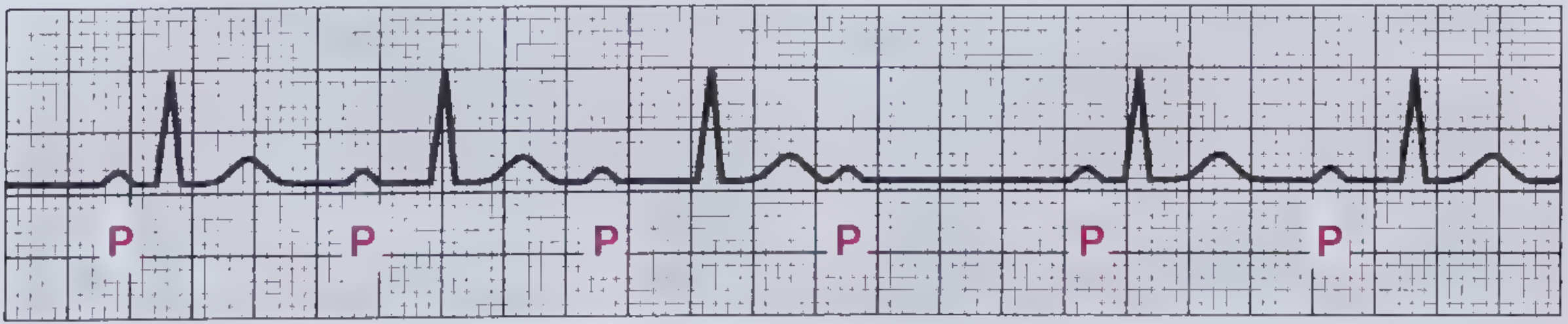
FIGURE - Mobitz I second-degree AV block. The P-wave rate is constant, but PR interval progressively lengthens until a QRS is completely blocked (after the 4th P wave). (Frameworks for Internal Medicine)
- Level of block: AV node
- Associated with: right coronary artery territory MI (inferior leads II, III, aVF)
- Usually benign, may be transient
- Rarely requires pacing
Second-Degree AV Block - Mobitz Type II
ECG findings: Constant PR interval with sudden unexpected drop of a QRS (no progressive PR lengthening).
- Level of block: His-Purkinje system (below AV node)
- High risk of progression to complete heart block
- Permanent pacemaker usually required (Frameworks for Internal Medicine)
Second-Degree AV Block - 2:1 Block

FIGURE - Second-degree AV block with 2:1 AV conduction. There are twice as many P waves as QRS complexes - every other atrial impulse is blocked. (Frameworks for Internal Medicine)
- Every other P wave is non-conducted
- Cannot distinguish Mobitz I from II electrocardiographically in pure 2:1 block
- PR interval of conducted beats helps: prolonged = more likely Mobitz I; normal = more likely Mobitz II
Third-Degree (Complete) AV Block
ECG findings: Complete AV dissociation - P waves and QRS complexes are completely independent.
- Atrial rate (P waves) is faster than the ventricular rate (QRS)
- Escape rhythm: junctional (narrow QRS, 40-60 bpm) or ventricular (wide QRS, 20-40 bpm)
- Causes: inferior MI (transient), anterior MI (permanent), Lyme disease, digoxin toxicity, fibrosis
- Treatment: atropine acutely; permanent pacemaker for persistent cases (Goldman-Cecil Medicine)
3.5 Bundle Branch Blocks
| Feature | RBBB | LBBB |
|---|---|---|
| QRS duration | ≥ 0.12 sec | ≥ 0.12 sec |
| V1 morphology | rSR' ("rabbit ears"/ M-shaped) | Broad rS or QS |
| V6 morphology | qRS with wide S | Broad monophasic R, no Q |
| Mnemonic | WiLLiaM MaRRoW (W in V1, M in V6 = LBBB; M in V1, W in V6 = RBBB) | Same mnemonic |
| ST/T changes | Discordant (opposite to QRS direction) | Discordant |
| Axis | Normal or RAD | Normal or LAD |
| Significance | Often benign; new RBBB can indicate PE, RV strain | Significant - rules out STEMI interpretation; new LBBB = possible ACS |
Memory trick - "WiLLiaM MaRRoW":
- LBBB: W in V1, M in V6 (= "WilLiam")
- RBBB: M in V1, W in V6 (= "MaRRow")
3.6 Ventricular Arrhythmias
Premature Ventricular Contractions (PVCs)
- Wide, bizarre QRS (> 0.12 sec), not preceded by a P wave
- Followed by full compensatory pause (SA node not reset)
- T wave opposite in polarity to QRS
- If PVCs appear every other beat = bigeminy; every 3rd beat = trigeminy; consecutive pairs = couplets
Ventricular Tachycardia (VT)
- Rate: > 100 bpm (usually 140-250), wide QRS (> 0.12 sec)
- AV dissociation (P waves march through independently) = diagnostic of VT
- Fusion beats (sinus + ventricular = hybrid QRS) = diagnostic of VT
- Capture beats (sinus impulse successfully captures ventricle = narrow QRS amid wide ones) = diagnostic of VT
The algorithm below - from Goldman-Cecil Medicine - is the definitive clinical tool for distinguishing wide-QRS tachycardia VT from SVT with aberrancy:
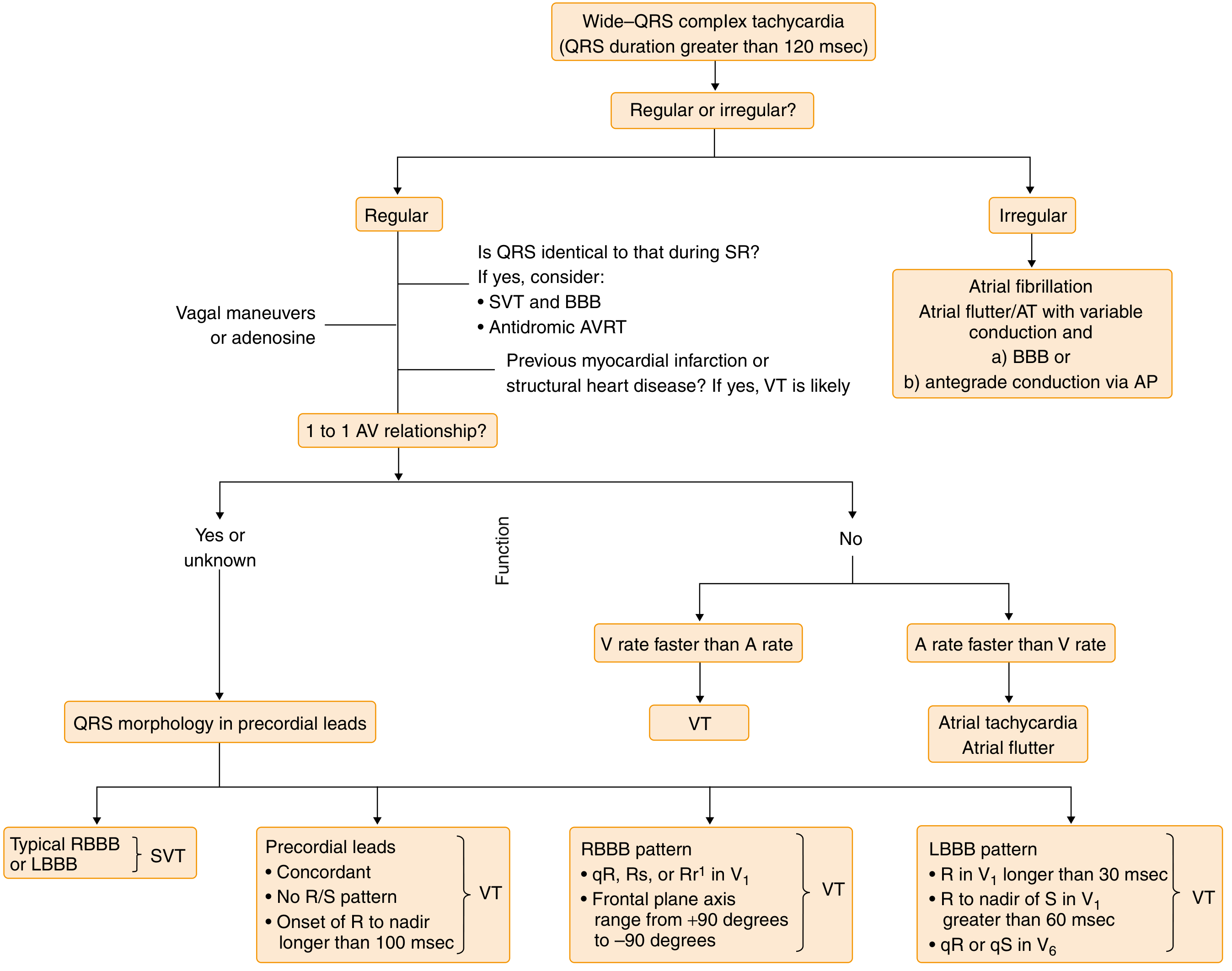
FIGURE - ECG algorithm for diagnosis of wide-complex tachycardias. Key decision points: regularity, AV relationship, QRS morphology in precordial leads. (Goldman-Cecil Medicine)
Ventricular Fibrillation (VF)
- Completely chaotic, disorganized electrical activity
- No identifiable QRS complexes, P waves, or T waves
- "Coarse" VF = larger amplitude; "fine" VF = nearly flat
- Immediately life-threatening; requires immediate defibrillation
PART 4 - ISCHEMIA AND INFARCTION
4.1 The ECG Progression of STEMI
Ischemia → Injury → Infarction follows a predictable ECG sequence:
Stage 1 (Minutes): Hyperacute T waves
- Tall, peaked, symmetric T waves (often first sign)
Stage 2 (Hours): ST elevation
- Convex ("tombstone") ST elevation ≥ 1 mm in limb leads, ≥ 2 mm in precordial leads in ≥ 2 contiguous leads
- Reciprocal ST depression in opposite leads
Stage 3 (Hours-Days): Q waves develop
- Pathological Q waves: > 1 mm wide or > 25% of QRS height
Stage 4 (Days-Weeks): T-wave inversion
- T waves invert in the leads showing ST elevation
Stage 5 (Weeks-Months): Normalization or persistent Q waves
- Q waves may persist indefinitely (scar)
4.2 STEMI by Territory
Below is a real 12-lead ECG of an anterior STEMI (Rosen's Emergency Medicine):
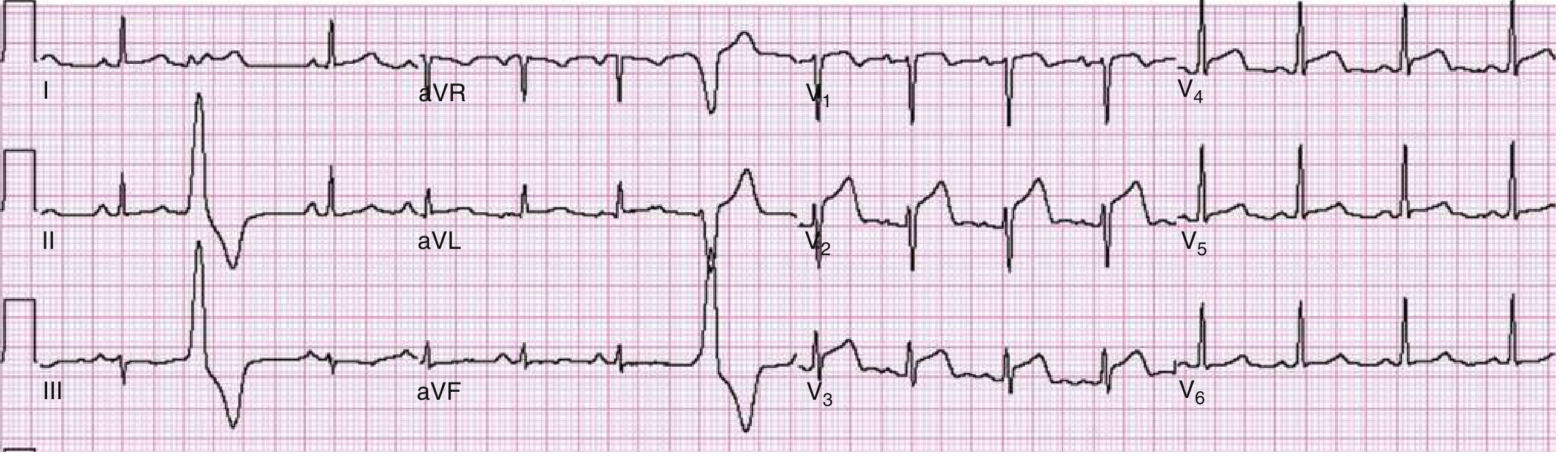
FIGURE - Anterior wall STEMI. ST elevation in V1-V4 with straight/oblique morphology. 90% LAD stenosis confirmed on catheterization. (Rosen's Emergency Medicine)
And an anterolateral STEMI involving V2-V6, I, and aVL:
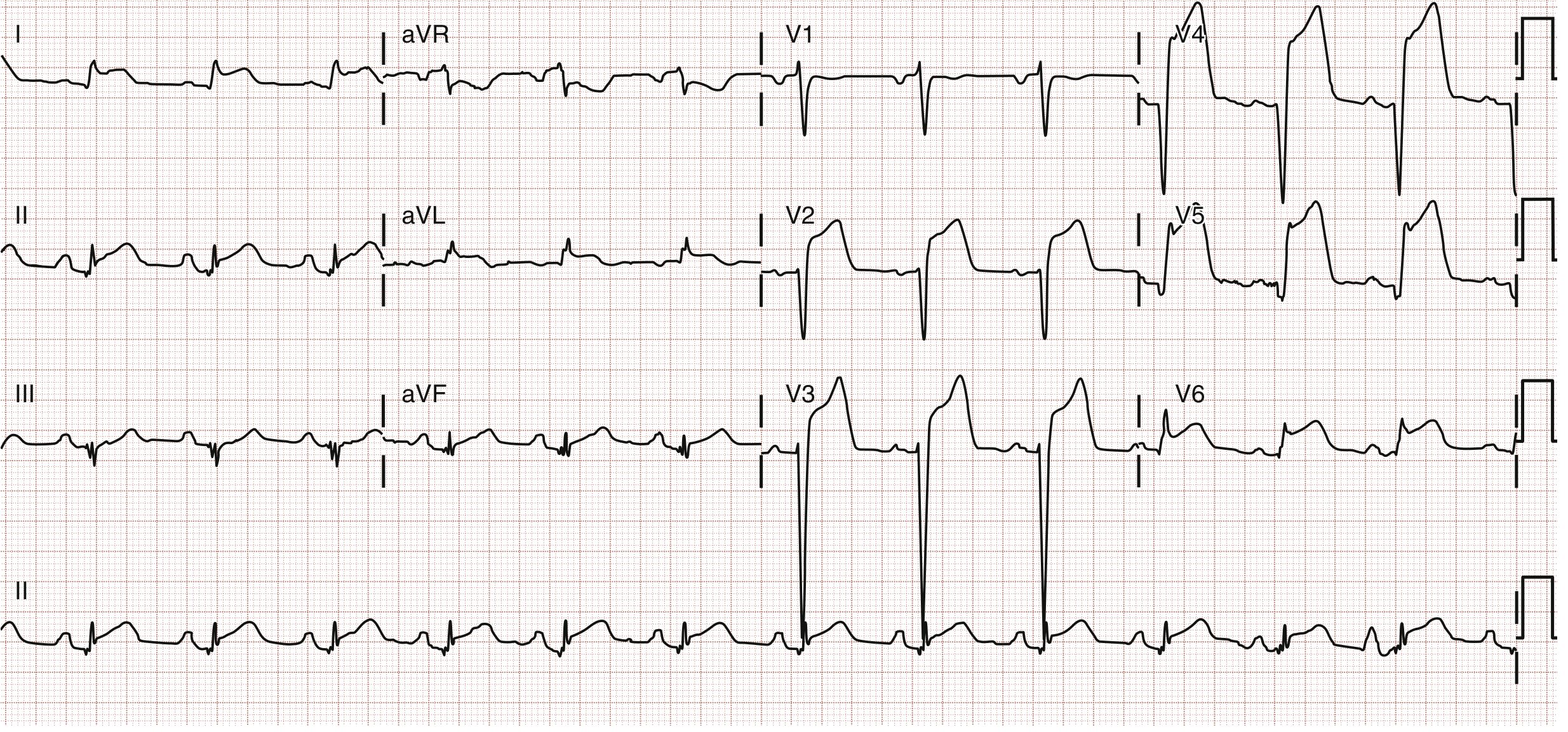
FIGURE - Anterolateral STEMI. STE in V2-V6, I, and aVL. 100% in-stent LAD thrombosis on catheterization. (Rosen's Emergency Medicine)
| Infarct Location | Leads with Changes | Artery |
|---|---|---|
| Anterior | V1-V4 | LAD |
| Anterolateral | V1-V6, I, aVL | LAD or LCx |
| Lateral | I, aVL, V5-V6 | LCx |
| Inferior | II, III, aVF | RCA (80%) / LCx |
| Posterior | Tall R and ST depression V1-V2 (mirror test) | RCA or LCx |
| Right ventricular | ST elevation in V3R-V4R, inferior ST elevation | RCA proximal |
| Left main/proximal LAD | ST elevation in aVR + diffuse ST depression | Left main or proximal LAD |
4.3 Special STEMI Patterns
de Winter Pattern (proximal LAD occlusion without classic STE):
- Upsloping ST depression with tall, peaked T waves in precordial leads V1-V6
- ST elevation in aVR
- Treat as STEMI equivalent
Wellens' Syndrome (proximal LAD critical stenosis, pain-free):
- Type A: Biphasic T waves (upright then inverted) in V2-V3
- Type B: Deep symmetric T wave inversions in V2-V3
- Do NOT stress test; high risk for massive anterior MI
Sgarbossa Criteria (STEMI in LBBB):
- Concordant ST elevation ≥ 1 mm in leads with positive QRS (+5 points)
- Concordant ST depression ≥ 1 mm in V1-V3 (+3 points)
- Discordant ST elevation ≥ 5 mm (+2 points)
- Score ≥ 3 = high specificity for acute MI
PART 5 - HYPERTROPHY
Left Ventricular Hypertrophy (LVH)
Voltage criteria (any one sufficient with appropriate clinical context):
- Sokolow-Lyon: S in V1 + R in V5 or V6 > 35 mm
- Cornell: R in aVL + S in V3 > 28 mm (men) or > 20 mm (women)
- R in aVL > 11 mm
- Strain pattern: ST depression and T-wave inversion in V5-V6, I, aVL (lateral "strain")
Right Ventricular Hypertrophy (RVH)
- Tall R wave in V1 (R > S in V1)
- Right axis deviation (> +90°)
- ST depression and T-wave inversion in V1-V4 (right "strain")
- Causes: pulmonary hypertension, cor pulmonale, severe pulmonary stenosis, PE (acute)
PART 6 - METABOLIC AND DRUG CHANGES
Hyperkalemia (progressive changes with rising K+)
| K+ Level | ECG Changes |
|---|---|
| 5.5-6.5 mEq/L | Tall, peaked, "tented" T waves |
| 6.5-7.5 mEq/L | Widened QRS, prolonged PR, flattened P waves |
| > 7.5 mEq/L | Absent P waves, "sine wave" pattern |
| > 9 mEq/L | VF or asystole |
Hypokalemia
- Flattened T waves
- U waves become prominent (U > T in same lead)
- ST depression
- Prolonged QU interval (often misread as long QT)
Hypercalcemia
- Shortened QT interval
- Short ST segment
Hypocalcemia
- Prolonged QT interval (long ST segment)
Digoxin effect (not toxicity)
- "Reverse tick" or "sagging" ST depression (scooped ST depression)
- Shortened QT
- T-wave flattening or inversion
Digoxin toxicity
- Any arrhythmia, especially PAT with block, junctional tachycardia, bidirectional VT
- PVCs (bigeminy very common)
PART 7 - OTHER IMPORTANT CONDITIONS
Pericarditis
Stage I (acute): Diffuse concave ("saddle-shaped") ST elevation in nearly all leads except aVR and V1 (where ST is depressed). PR depression is pathognomonic.
Key differentiator from STEMI: In pericarditis, STE is diffuse (not in a single vascular territory), concave (not convex), and PR depression is present.
Stage II-IV: ST normalizes → T-wave inversion → normalization.
Pulmonary Embolism
Classic (but not universal) ECG findings:
- S1Q3T3: S wave in lead I, Q wave and T-wave inversion in lead III
- Sinus tachycardia (most common finding)
- New RBBB or right heart strain pattern
- T-wave inversions in V1-V4
- Right axis deviation
Brugada Syndrome
- Type 1 (diagnostic): Coved ST elevation ≥ 2 mm with T-wave inversion in V1-V2 (unprovoked or with sodium channel blockers)
- Type 2: Saddle-back ST elevation in V1-V2 (not diagnostic alone)
- Associated with sudden cardiac death from VF in structurally normal hearts
- More common in males, South/Southeast Asians
Long QT Syndrome
- QTc > 450 ms (men), > 470 ms (women), or > 500 ms (high risk)
- Risk of torsades de pointes (polymorphic VT)
- Causes: congenital (LQTS1, 2, 3) or acquired (drugs - quinidine, sotalol, erythromycin, antipsychotics; hypokalemia, hypomagnesemia)
Hypothermia
- Osborn (J) wave: Positive deflection at the J-point (junction of QRS and ST segment), best seen in inferior and lateral leads
- Shivering artifact
- Bradycardia, prolonged intervals
- Osborn wave size correlates with depth of hypothermia
PART 8 - QUICK REFERENCE SUMMARY TABLE
| Condition | Rate | Rhythm | P Waves | PR | QRS | ST/T |
|---|---|---|---|---|---|---|
| Normal sinus | 60-100 | Regular | Upright, before each QRS | 0.12-0.20 | Narrow <0.12 | Normal |
| Sinus tachycardia | >100 | Regular | Normal | Normal | Normal | Normal |
| AF | Variable | Irregularly irregular | No P (fibrillatory baseline) | None | Narrow (usually) | Variable |
| Atrial flutter | ~150 (with 2:1) | Regular or variable | Sawtooth 300/min | Variable | Narrow | Variable |
| SVT/AVNRT | 150-250 | Regular | Buried/retrograde | None visible | Narrow | Normal |
| 1st-degree AV block | Normal | Regular | Normal | >0.20 sec | Normal | Normal |
| Mobitz I (Wenckebach) | Normal | Regularly irregular | Normal | Progressive lengthening then drop | Normal | Normal |
| Mobitz II | Normal | Regularly irregular | Normal | Constant, then QRS drops | Normal/wide | Normal |
| 3rd-degree block | Slow | Regular (but dissociated) | Normal atrial rate | Completely dissociated | Wide (escape) or narrow | Normal |
| RBBB | Normal | Regular | Normal | Normal | ≥0.12, rSR' in V1, wide S in V6 | Discordant T |
| LBBB | Normal | Regular | Normal | Normal | ≥0.12, broad R in V6, QS in V1 | Discordant T |
| STEMI | Variable | Any | Normal | Normal | May have Q waves | ST elevation, convex |
| NSTEMI/UA | Variable | Any | Normal | Normal | Normal | ST depression/T inversion |
| LVH | Normal | Regular | May be enlarged | Normal | Tall voltage | Lateral strain |
| Hyperkalemia | Slow if severe | Variable | Tall peaked T first, then P disappears | Prolonged | Widened | Tall T, then sine wave |
| VT | >100 | Regular | Dissociated | None | Wide ≥0.12 | Discordant |
| VF | - | Chaotic | None | None | No QRS | Chaotic |
PART 9 - CLINICAL MEMORY AIDS
Rate calculation: 300 ÷ (number of large boxes between R waves) = rate in bpm
Axis quick rule: "If I and aVF are both up → normal axis. I up, aVF down → LAD. I down, aVF up → RAD."
Bundle branch block mnemonic: WiLLiaM MaRRoW - LBBB = W in V1, M in V6; RBBB = M in V1, W in V6
AV blocks mnemonic: "1st degree = PR prolonged, everyone gets through. 2nd degree = some are dropped. 3rd degree = none get through."
STEMI localization: "Inferior = II, III, aVF; Anterior = V1-V4; Lateral = I, aVL, V5-V6"
Hyperkalemia progression: "Peaked T → Wide QRS → No P → Sine wave → Death"
Key reference for further reading: The step-by-step approach above is derived from Boron & Boulpaep's Medical Physiology, Braunwald's Heart Disease, Goldman-Cecil Medicine, Rosen's Emergency Medicine, and Frameworks for Internal Medicine. For video-based learning, this Ninja Nerd lecture is an excellent companion:
This is a shared conversation. Sign in to Orris to start your own chat.