Posterior interosseous nerve
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a thorough, well-illustrated answer.
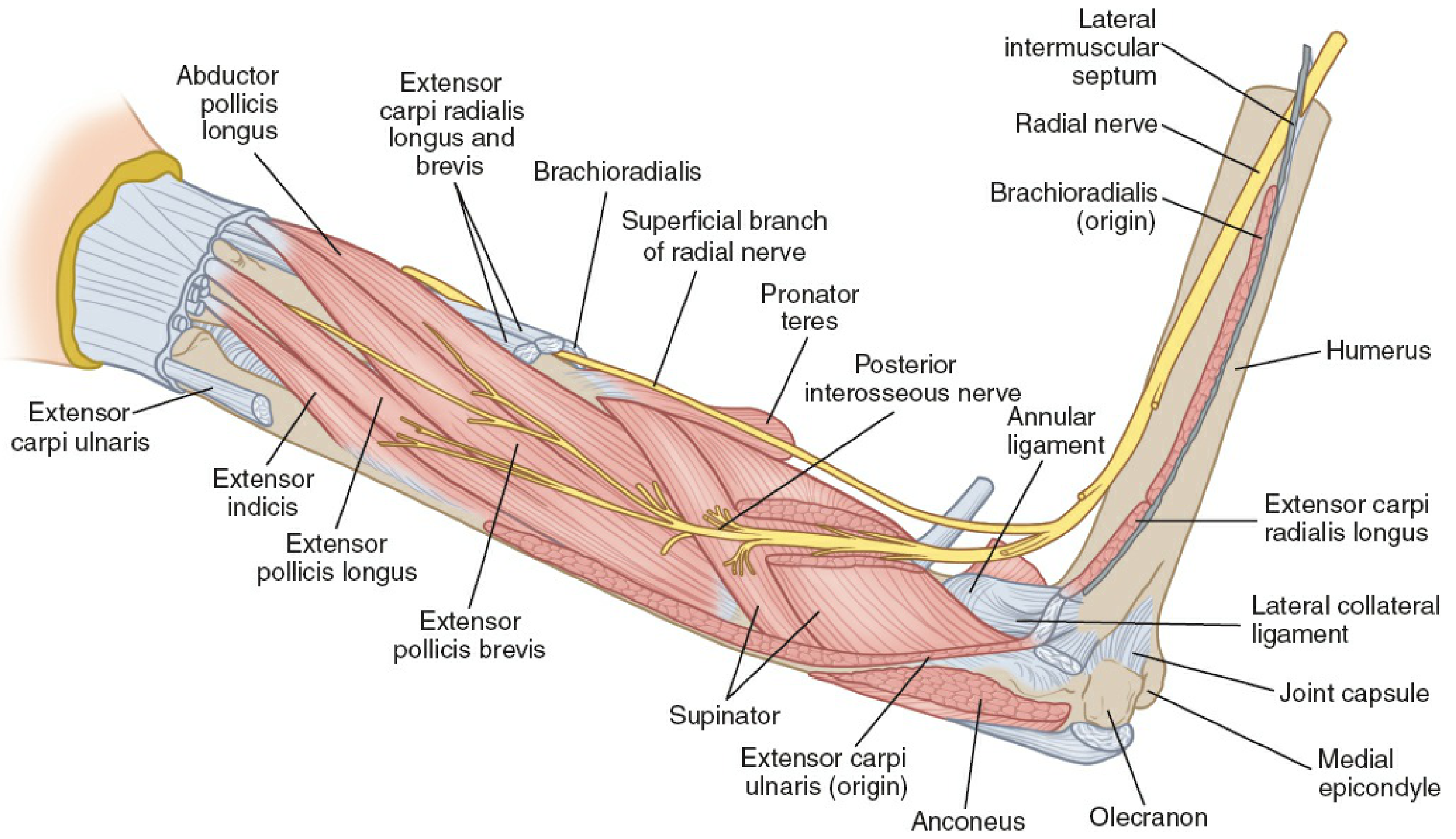
Posterior Interosseous Nerve (PIN)
Origin and Root Value
The PIN is the deep motor terminal branch of the radial nerve (C5-C8, T1). The radial nerve arises from the posterior cord of the brachial plexus, spirals around the humerus in the radial groove, pierces the lateral intermuscular septum, and enters the anterior compartment of the arm. Just proximal to the lateral epicondyle it divides into two terminal branches:
- Superficial branch - purely sensory, supplies dorsum of lateral hand and first 3.5 digits
- Deep branch - purely motor, which becomes the PIN after traversing the supinator muscle
Course
The deep branch of the radial nerve passes anterior to the radial head, through the arcade of Frohse (a fibrous arch at the proximal border of the supinator), traverses the two layers of the supinator muscle, and emerges at the distal border of supinator as the posterior interosseous nerve proper. It then courses along the dorsal surface of the interosseous membrane to reach the wrist, where it terminates as a pseudo-ganglion innervating the dorsal wrist joint capsule and the four radial metacarpophalangeal joints.
Muscles Innervated
Branches given off before entering supinator (from the radial nerve/deep branch itself):
- Extensor carpi radialis longus (ECRL) - directly from radial nerve
- Extensor carpi radialis brevis (ECRB) - often before PIN proper
Muscles innervated by the PIN (from THIEME Atlas / Rockwood & Green):
| Muscle | Function |
|---|---|
| Supinator | Forearm supination |
| Extensor digitorum communis (EDC) | Extension of fingers (MCP) |
| Extensor digiti minimi (EDM) | Extension of small finger |
| Extensor carpi ulnaris (ECU) | Wrist extension (ulnar) |
| Abductor pollicis longus (APL) | Thumb abduction |
| Extensor pollicis brevis (EPB) | Thumb extension (MCP) |
| Extensor pollicis longus (EPL) | Thumb extension (IP) |
| Extensor indicis proprius (EIP) | Index finger extension |
Note: ECRL and ECRB branch off proximal to the PIN (before/at the arcade of Frohse), so they are spared in PIN lesions.
Key Anatomical Relationships
- The arcade of Frohse is the most important site of potential compression - a fibrous arch at the proximal free edge of the superficial head of supinator
- Four potential compression points in the radial tunnel (Campbell's):
- Origin of ECRB (fibrous tendinous margin)
- Adhesions around the radial head
- The radial recurrent arterial fan (leash of Henry)
- The arcade of Frohse - most common
PIN Syndrome (Entrapment Neuropathy)
Clinical features (Rheumatology, 2-Volume Set):
- Forearm pain ± weakness
- No sensory loss (purely motor nerve)
- No reflex changes
- Wrist deviates radially on attempted extension (ECU paralyzed, ECRL/ECRB intact)
- Inability to extend MCP joints ("drop finger" without true wrist drop - wrist can still extend radially)
- Difficulty extending the thumb (EPL, EPB) and abducting the thumb (APL)
- If compression is at the distal supinator border only: isolated "drop-thumb"
Causes:
- Arcade of Frohse compression (most common)
- Rheumatoid synovitis of the elbow joint
- Ganglion cysts, lipomas, or other space-occupying lesions
- Radial head fracture-dislocation
- Volkmann ischemic contracture
- Aneurysms, enlarged bursae
Spinner's classification (Campbell's Operative Orthopaedics):
- Type 1: Complete paralysis of all PIN-supplied muscles
- Type 2: Partial (one or a few muscles affected)
Important nuance (Localization in Clinical Neurology): PIN syndrome is not always caused by focal compression at the supinator. Research shows ~84% of cases may involve partial fascicular lesions of the radial nerve trunk at the upper arm level, following a somatotopic pattern - the fascicles destined to form the PIN are selectively damaged more proximally. This explains why neuroimaging (MRI neurography) should be considered as a complementary diagnostic tool.
Differential Diagnosis
- Lateral epicondylitis (pain without weakness)
- Radial tunnel syndrome (pain-dominant without true motor loss)
- Posterior cord brachial plexus lesion (broader motor/sensory deficit)
- Central lesion causing wrist/finger drop
- Focal myopathy mimicking PIN syndrome
Diagnosis
- Electrodiagnostic studies (EMG/NCS)
- MRI or ultrasound of the elbow/forearm to identify structural compression
- Diagnostic corticosteroid injection
Treatment
- Conservative: splinting, activity modification, NSAIDs, corticosteroid injection
- Surgical: decompression of the radial tunnel (releasing the arcade of Frohse and other compressive structures) when conservative measures fail, or when a compressive lesion (tumor, ganglion) is identified
Sources: Rheumatology 2-Volume Set (Elsevier 2022), p. 2870-2922 | Localization in Clinical Neurology 8e, p. 121-122 | Campbell's Operative Orthopaedics 15e (2026), p. 8890-8930 | Rockwood & Green's Fractures in Adults 10e (2025) | THIEME Atlas of Anatomy, General & Musculoskeletal System, p. 388
This is a shared conversation. Sign in to Orris to start your own chat.