Fascial nerve course
Facial Nerve (CN VII) - Complete Course
Fiber Composition
- Special visceral efferent (SVE) - motor to muscles of facial expression, stapedius, stylohyoid, and posterior belly of digastric (from the motor nucleus)
- General visceral efferent (GVE) - preganglionic parasympathetic to lacrimal gland, nasal/palatal glands (via GSPN), and submandibular/sublingual glands (via chorda tympani) (from the superior salivatory nucleus)
- Special visceral afferent (SVA) - taste from anterior 2/3 of tongue via chorda tympani (cell bodies in geniculate ganglion)
- General somatic afferent (GSA) - cutaneous sensation to EAC and conchal skin
- Visceral afferent - from mucosa of nose, pharynx, palate (all afferent fibers travel in the nervus intermedius; nucleus tractus solitarius)
Segment-by-Segment Course
1. Intracranial (Cisternal) Segment
- The main motor root exits the brainstem at the pontomedullary junction, between the pons and the olive
- The nervus intermedius (sensory/parasympathetic root) emerges slightly more posteriorly, between the pons and inferior cerebellar peduncle, and joins the main trunk
- Both roots traverse the cerebellopontine angle (CPA) together with CN VIII toward the internal acoustic meatus (IAM)
- In the CPA, the nerve lies anterosuperior to CN VIII
2. Internal Acoustic Meatus (IAM)
- CN VII lies in the anterosuperior quadrant of the IAM, above the cochlear nerve
- The superior and inferior vestibular nerves lie posteriorly
- At the lateral end of the IAM, the nerve passes through the narrowest point - the meatal foramen - into the labyrinthine segment
- At this point, the nerve lacks an epineurium and associated vascular plexus, making it a vulnerable "watershed zone" between the vertebrobasilar and external carotid artery circulations
3. Intratemporal Course (Fallopian / Facial Canal)
a. Labyrinthine Segment
- The first, shortest (~4 mm), and narrowest segment
- Travels between the cochlea (anteriorly) and vestibule (posteriorly), superior to the cochlea
- Ends at the geniculate fossa, where it forms the geniculate ganglion (contains cell bodies of sensory neurons)
- The ganglion is separated from the middle fossa floor by a very thin layer of bone, dehiscent in ~25% of ears
- Branch given off: Greater superficial petrosal nerve (GSPN) - preganglionic parasympathetic to lacrimal/nasal glands; it runs anteriorly along the middle fossa floor, through the facial hiatus, to the pterygopalatine ganglion
- First genu: At the geniculate ganglion, the nerve makes an acute turn posteriorly and slightly inferiorly into the tympanic segment
- Surgical landmark: Vertical crest (Bill's bar) in the IAC
b. Tympanic (Horizontal) Segment
- Runs along the medial wall of the middle ear (anterior attic), above the promontory
- Passes superior to the cochleariform process and forms the superior wall of the oval window niche
- The most common site of congenital dehiscence of the bony canal, especially above the oval window
- At the pyramidal eminence, the nerve makes the second genu, turning inferiorly
- The second genu is located just anteroinferior to the lateral semicircular canal and anterior to a line through the short process of the incus
- Surgical landmarks: cochleariform process, oval window, pyramidal eminence
c. Mastoid (Vertical) Segment
- Descends vertically within the mastoid bone, posterior to the external auditory canal
- Most variable segment in its path
- Branches given off:
- Nerve to stapedius - via a tiny canaliculus from the pyramidal eminence, innervates the stapedius muscle
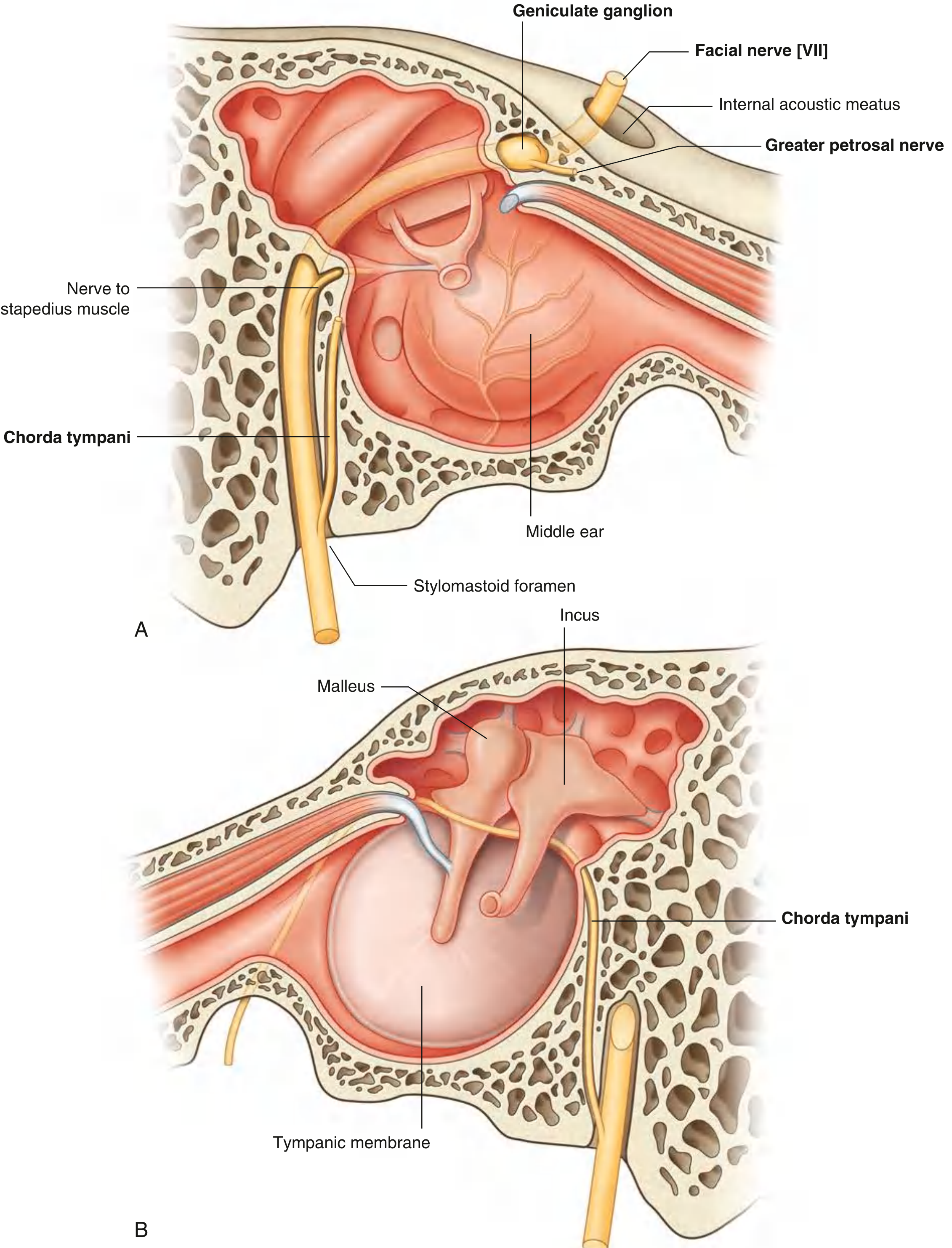
- Chorda tympani - given off in the lower part of this segment; re-enters the middle ear, crosses the tympanic membrane medial surface, passes between the malleus and incus, exits via the petrotympanic fissure; carries taste from anterior 2/3 tongue and preganglionic parasympathetic fibers to submandibular/sublingual glands
- The nerve exits the fallopian canal at the stylomastoid foramen (now a purely motor nerve)
- Surgical landmark: aponeurosis of the posterior belly of digastric is closely applied at the stylomastoid foramen
| Segment | Surgical Landmark |
|---|---|
| Labyrinthine | Vertical crest (Bill's bar) |
| Geniculate ganglion | Retrograde dissection of GSPN (middle fossa) |
| Tympanic segment | Supratubal recess; cochleariform process |
| Second genu | Oval window |
| Mastoid segment | Pyramidal eminence; short process of incus; chorda tympani |
| Stylomastoid foramen | Posterior digastric aponeurosis |
4. Extracranial Course
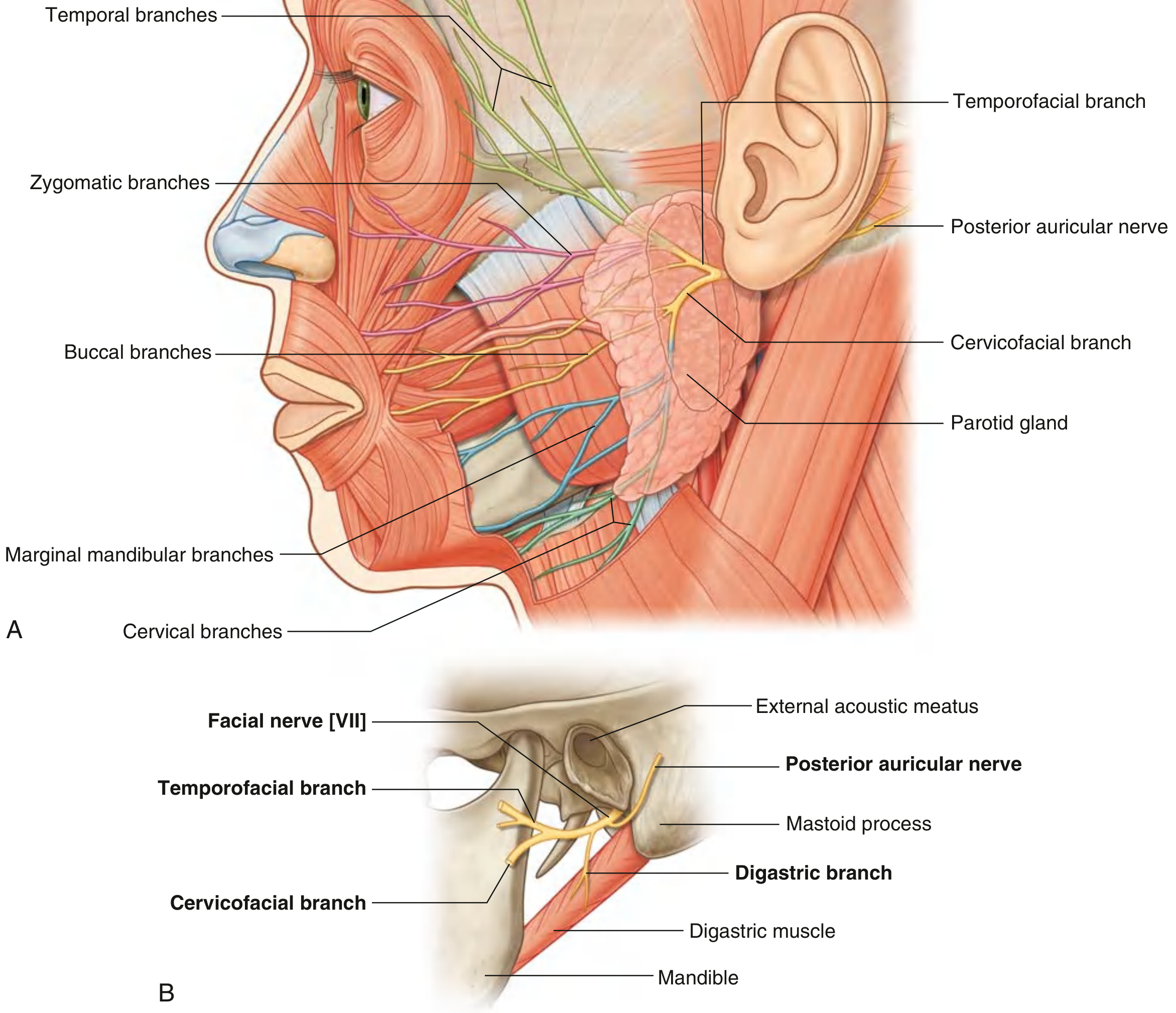
- Posterior auricular nerve - given off immediately; supplies the occipital belly of occipitofrontalis and the auricular muscles
- Branch to posterior belly of digastric and stylohyoid muscle
- The main trunk swings forward and laterally, entering the parotid gland (passing between its superficial and deep lobes)
In the Parotid Gland
- The nerve divides into upper (temporofacial) and lower (cervicofacial) divisions
- Further branching and anastomosis occur within the gland
- Five terminal groups emerge from the borders of the parotid:
| Branch | Exit | Muscles Supplied |
|---|---|---|
| Temporal | Superior border | Frontalis, orbicularis oculi (superior), corrugator |
| Zygomatic | Anterior/superior border | Orbicularis oculi (inferior), zygomaticus |
| Buccal | Anterior border | Buccinator, upper lip muscles, nasalis; follows parotid duct |
| Marginal mandibular | Inferior/anterior border | Lower lip, mentalis, depressor anguli oris |
| Cervical | Inferior border | Platysma |
Clinical note: Injuries lateral to a vertical line through the lateral canthus of the eye are potentially repairable with nerve stimulation identification. Injuries medial to this line are unlikely to cause significant permanent deficits due to distal arborisation and cross-innervation. The buccal branch closely follows the parotid duct and may be simultaneously transected in cheek lacerations.
Blood Supply to the Facial Nerve
- Labyrinthine/cisternal segment: Labyrinthine arteries from AICA (vertebrobasilar)
- Intratemporal segment (tympanic/mastoid): Petrosal branch of the middle meningeal artery (external carotid)
- Stylomastoid region and extratemporal: Stylomastoid artery (from posterior auricular artery, branch of ECA)
Key Clinical Correlates
| Location of Lesion | Deficits |
|---|---|
| Motor nucleus/brainstem | Ipsilateral LMN facial palsy + other cranial nerve signs |
| CPA (e.g., acoustic neuroma) | Facial palsy + hearing loss + vertigo |
| Geniculate ganglion (e.g., Ramsay Hunt) | Facial palsy + loss of taste anterior 2/3 tongue + hyperacusis + reduced lacrimation |
| Distal to geniculate but proximal to stapedius branch | Facial palsy + loss of taste + hyperacusis (lacrimation intact) |
| Distal to stapedius but proximal to chorda tympani | Facial palsy + loss of taste (no hyperacusis) |
| Distal to chorda tympani (at/below stylomastoid foramen) | Pure motor facial palsy only |
| Parotid/extratemporal | Selective branch palsies |
From which book .. you took this answer
1. 📘 Cummings Otolaryngology Head and Neck Surgery
- Primary source for the intratemporal course
- Provided the detailed segment-by-segment description (labyrinthine, tympanic, mastoid segments), the surgical landmarks table, blood supply, and vulnerability of each segment
- Blocks used:
block28andblock30
2. 📘 Scott-Brown's Otorhinolaryngology Head & Neck Surgery - Vol 2
- Provided the intracranial (cisternal) and IAM course, the position of CN VII relative to CN VIII in the IAM, and the extracranial branches after the stylomastoid foramen
- Block used:
block12
3. 📘 Gray's Anatomy for Students
- Provided the extratemporal and parotid gland course, the division into upper and lower trunks, and the five terminal branches
- Block used:
block4
4. 📘 Bailey and Love's Short Practice of Surgery (28th Edition)
- Provided clinical context on facial nerve injury assessment, the lateral canthus rule for repairability, and the relationship of the buccal branch to the parotid duct
- Block used:
block4andblock7
Y not vishram singh
| Book | Type |
|---|---|
| Gray's Anatomy for Students | Standard anatomy reference |
| Netter's Atlas of Human Anatomy | Atlas |
| THIEME Atlas - General Anatomy & Musculoskeletal System | Atlas |
| Color Atlas of Human Anatomy (Vols 1, 2, 3) | Atlas |
| Neuroanatomy through Clinical Cases | Neuro-focused |
| Imaging Anatomy (Bones, Joints, Vessels, Nerves) | Imaging-based |
Fascial nerve course
Facial Nerve [VII] Course
Source: Gray's Anatomy for Students
Fiber Types
| Fiber Type | Function |
|---|---|
| BE (Branchial Efferent) | Motor to muscles of facial expression, stapedius, stylohyoid, posterior belly of digastric |
| GVE (Parasympathetic) | Secretomotor to lacrimal gland, submandibular & sublingual glands, nasal & palatal mucous glands |
| SA (Special Afferent) | Taste from anterior 2/3 of tongue |
| GSA (General Somatic Afferent) | Sensation from part of external acoustic meatus and deeper parts of auricle |
The Two Roots
- Large motor root - carries the BE (branchial motor) fibers
- Smaller sensory root = Nervus Intermedius - carries SA (taste), GVE (parasympathetic), and GSA fibers
Step-by-Step Course
1. Posterior Cranial Fossa
- Both roots cross the posterior cranial fossa
- They leave the cranial cavity through the internal acoustic meatus (IAM) together with CN VIII (vestibulocochlear) and the labyrinthine artery
2. Inside the Petrous Temporal Bone
- After entering the facial canal in the petrous part of the temporal bone, the two roots fuse to form a single facial nerve
- The nerve then enlarges to form the geniculate ganglion - a sensory ganglion containing cell bodies of sensory neurons (equivalent to a spinal ganglion)
- At the geniculate ganglion, the nerve bends posteriorly and laterally (first bend), traveling between the internal ear and middle ear
- It then turns sharply downward (second bend) and runs in an almost vertical direction
- It exits through the stylomastoid foramen
Branches Given Off Inside the Temporal Bone
i. Greater Petrosal Nerve (at the Geniculate Ganglion)
- First branch of the facial nerve
- Carries preganglionic parasympathetic (GVE) fibers
- Leaves the geniculate ganglion, travels anteromedially through the temporal bone
- Emerges through the hiatus for the greater petrosal nerve on the anterior surface of the petrous bone
- Travels to the pterygopalatine ganglion → postganglionic fibers supply the lacrimal gland and nasal/palatal glands
ii. Nerve to Stapedius
- Given off near the beginning of the vertical descent
- Innervates the stapedius muscle in the middle ear
iii. Chorda Tympani
- Given off just before the nerve exits the skull
- Does NOT immediately exit - instead ascends back into the middle ear through its posterior wall
- Passes near the upper aspect of the tympanic membrane, running between the malleus and incus
- Exits the middle ear through a canal to the petrotympanic fissure
- Joins the lingual nerve in the infratemporal fossa
- Carries: taste (SA) from anterior 2/3 of tongue + preganglionic parasympathetic fibers to the submandibular ganglion (→ submandibular and sublingual glands)
Diagram (Gray's Anatomy for Students, Fig. 8.136)
Extracranial Course (After Stylomastoid Foramen)
- Exits through the stylomastoid foramen
- Passes into the parotid gland
- Divides into upper and lower trunks inside the gland
- Further branching and anastomosis occur within the parotid
Five Terminal Groups emerge from the borders of the parotid gland:
| Branch | Emerges From | Supplies |
|---|---|---|
| Temporal | Upper border | Muscles of forehead and upper face |
| Zygomatic | Upper/anterior border | Muscles around eye |
| Buccal | Anterior border | Cheek and upper lip muscles |
| Marginal Mandibular | Lower/anterior border | Lower lip and chin muscles |
| Cervical | Lower border | Platysma |
Clinical note (Gray's): The intimate relationship between CN VII and the parotid gland means that surgical removal of the parotid gland is a difficult dissection if all branches are to be spared.
Lesion Localization (Gray's Anatomy)
| Site of Lesion | Effect |
|---|---|
| Above the motor nucleus (UMN) | Contralateral lower face weakness only (upper face spared - bilateral cortical input) |
| At/below the motor nucleus (LMN - e.g. Bell's palsy) | Ipsilateral whole face weakness |
| At geniculate ganglion | Facial palsy + loss of taste + reduced lacrimation + hyperacusis |
| At/below stylomastoid foramen | Pure motor facial palsy only |
Make it short and send just like a flow chart
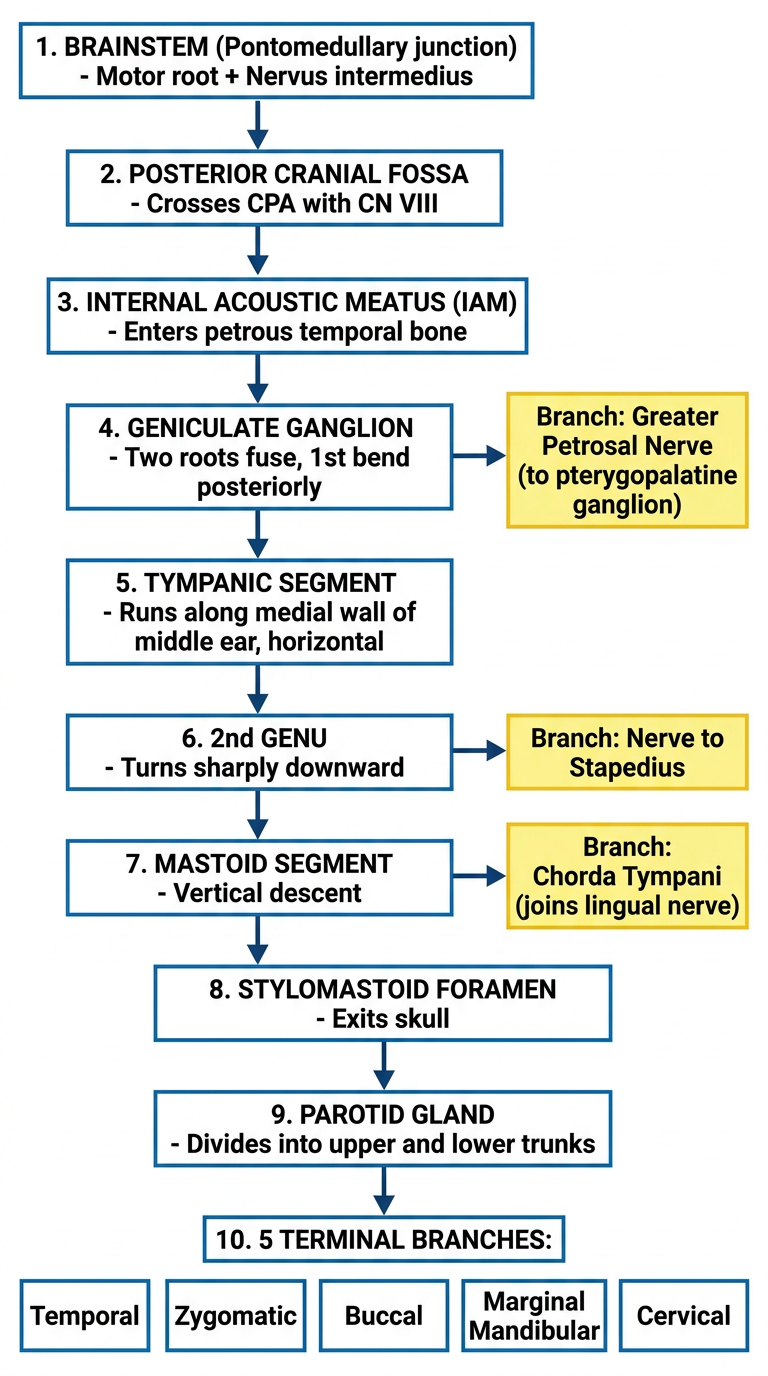
A clean vertical flowchart showing the course of the Facial Nerve (CN VII) with the following steps connected by downward arrows: 1. BRAINSTEM (Pontomedullary junction) - Motor root + Nervus intermedius 2. POSTERIOR CRANIAL FOSSA - Crosses CPA with CN VIII 3. INTERNAL ACOUSTIC MEATUS (IAM) - Enters petrous temporal bone 4. GENICULATE GANGLION - Two roots fuse, 1st bend posteriorly → Branch: Greater Petrosal Nerve (to pterygopalatine ganglion) 5. TYMPANIC SEGMENT - Runs along medial wall of middle ear, horizontal 6. 2nd GENU - Turns sharply downward → Branch: Nerve to Stapedius 7. MASTOID SEGMENT - Vertical descent → Branch: Chorda Tympani (joins lingual nerve) 8. STYLOMASTOID FORAMEN - Exits skull 9. PAROTID GLAND - Divides into upper and lower trunks 10. 5 TERMINAL BRANCHES: Temporal | Zygomatic | Buccal | Marginal Mandibular | Cervical Use a white background, bold dark text, blue boxes for main steps, yellow side boxes for branches, clean sans-serif font, simple arrow connectors. Medical education style.
Pontomedullary Junction
↓
Posterior Cranial Fossa (with CN VIII)
↓
Internal Acoustic Meatus (IAM)
↓
Geniculate Ganglion → Greater Petrosal Nerve
↓
Tympanic Segment (medial wall of middle ear)
↓
2nd Genu → Nerve to Stapedius
↓
Mastoid Segment (vertical) → Chorda Tympani
↓
Stylomastoid Foramen (exits skull)
↓
Parotid Gland (upper + lower trunks)
↓
5 Terminal Branches:
Temporal | Zygomatic | Buccal | Marginal Mandibular | Cervical
Distribution of fascial nerve
Distribution of the Facial Nerve [VII]
A. Branches INSIDE the Temporal Bone
| Branch | Origin | Distribution |
|---|---|---|
| Greater Petrosal Nerve | Geniculate ganglion (1st branch) | Preganglionic parasympathetic → pterygopalatine ganglion → lacrimal gland, nasal & palatal glands |
| Nerve to Stapedius | Start of vertical/mastoid segment | Stapedius muscle (middle ear) |
| Chorda Tympani | Just before stylomastoid foramen | Taste from anterior 2/3 of tongue + preganglionic parasympathetic → submandibular ganglion → submandibular & sublingual glands |
B. Branches AFTER Stylomastoid Foramen (Extracranial)
Immediate branches (before entering parotid):
| Branch | Supplies |
|---|---|
| Posterior Auricular Nerve | Occipital belly of occipitofrontalis + posterior auricular muscle |
| Branch to Digastric & Stylohyoid | Posterior belly of digastric + stylohyoid muscle |
Terminal branches (from Parotid Plexus) - "Ten Zebras Brought My Cat"
| Branch | Exits From | Area Supplied | Muscles |
|---|---|---|---|
| Temporal | Superior border of parotid | Temple, forehead, supra-orbital area | Frontalis, orbicularis oculi (upper), corrugator supercilii |
| Zygomatic | Anterosuperior border | Infra-orbital area, lateral nose, upper lip | Orbicularis oculi (lower), zygomaticus |
| Buccal | Anterior border | Cheek, upper lip, corner of mouth | Buccinator, orbicularis oris, nasalis |
| Marginal Mandibular | Anteroinferior border | Lower lip and chin | Depressor anguli oris, depressor labii, mentalis |
| Cervical | Inferior border | Neck | Platysma |
Summary Flowchart
FACIAL NERVE [VII]
│
├── Inside Temporal Bone
│ ├── Greater Petrosal Nerve → Lacrimal & nasal glands
│ ├── Nerve to Stapedius → Stapedius muscle
│ └── Chorda Tympani → Taste (ant. 2/3 tongue) + submandibular/sublingual glands
│
├── At Stylomastoid Foramen
│ ├── Posterior Auricular Nerve → Occipitofrontalis + auricular muscles
│ └── Digastric branch → Post. belly digastric + stylohyoid
│
└── Parotid Gland (5 terminal branches)
├── Temporal → Forehead, upper face
├── Zygomatic → Infra-orbital, nose
├── Buccal → Cheek, lip
├── Marginal Mandibular → Lower lip, chin
└── Cervical → Platysma
Mnemonic for 5 terminal branches: To Zanzibar By Motor Car = Temporal, Zygomatic, Buccal, Marginal mandibular, Cervical
Clinical correlation of fascial nerve
Clinical Correlations of the Facial Nerve [VII]
1. Lesion Localization - The Key Concept
"A series of lesions may affect the nerve along its course, and it is possible, with good clinical expertise, to determine the exact site of the lesion in relation to the course of the nerve."
2. Central Lesions (Above the Motor Nucleus - UMN)
- Lesion above the facial nucleus (e.g., cortical stroke)
- Results in contralateral lower face weakness ONLY
- Upper face is SPARED - because the upper part of the facial nucleus receives bilateral cortical input (from both hemispheres)
- Key point: UMN lesion → forehead sparing
3. Brainstem Lesion (At the Motor Nucleus - LMN)
- Affects ipsilateral whole face (upper + lower)
- May be associated with other cranial nerve signs
4. Lesion at/around the Geniculate Ganglion
| Lost Function | Reason |
|---|---|
| Motor - whole ipsilateral face | Proximal to all motor branches |
| Taste - anterior 2/3 tongue | Proximal to chorda tympani |
| Lacrimation (dry eye) | Proximal to greater petrosal nerve |
| Salivation (submandibular/sublingual) | Proximal to chorda tympani |
| Hyperacusis | Proximal to nerve to stapedius |
Example: Herpes zoster oticus (Ramsay Hunt Syndrome) - viral inflammation at geniculate ganglion
5. Lesion at/around the Stylomastoid Foramen (Most Common!)
"Lesions at and around the stylomastoid foramen are the COMMONEST abnormality of the facial nerve [VII] and usually result from a viral inflammation of the nerve within the bony canal before exiting through the stylomastoid foramen."
- Bell's Palsy is the classic example
- Ipsilateral loss of motor function of the WHOLE side of the face
- Produces unusual appearance + complicates chewing
- Lacrimation and taste may NOT be affected if the lesion is distal to the greater petrosal nerve and chorda tympani (which originate deep in the temporal bone)
6. Lesion Within the Parotid Gland
- Damage to branches within the parotid (e.g., parotid tumour, parotidectomy)
- Causes selective or complete facial muscle paralysis depending on which branches are injured
- Taste is PRESERVED - because chorda tympani leaves the facial nerve proximal to the parotid gland and joins the lingual nerve before reaching the gland
- Clinical case from Gray's: A patient undergoing parotidectomy developed mild right-side facial paralysis post-op, but taste to anterior 2/3 tongue was fully preserved
7. Corneal (Blink) Reflex
| Component | Nerve |
|---|---|
| Afferent (sensation) | Trigeminal nerve [V] |
| Efferent (eye closure) | Facial nerve [VII] - orbicularis oculi |
- Facial nerve palsy → cannot close the eye → corneal ulceration → secondary infection
- Loss of orbicularis oculi innervation → lower eyelid droops away (ectropion) → loss of tears → dry, ulcerated conjunctiva
Summary Table: Lesion Localization
LESION SITE MOTOR TASTE LACRIMATION HYPERACUSIS
─────────────────────────────────────────────────────────────────
UMN (above nucleus) Lower ✗ ✗ ✗
face
only
(contra)
Brainstem nucleus Whole ✗ ✗ ✗
face
(ipsi)
Geniculate Whole LOST LOST LOST
ganglion face
At nerve to Whole LOST LOST LOST
stapedius face
At chorda tympani Whole LOST Intact Intact
Stylomastoid Whole Intact Intact Intact
foramen face
(Bell's palsy)
Parotid gland Selective Intact Intact Intact
branches
Bottom line: The more proximal the lesion → the more functions lost. The more distal → only motor palsy.