Explain cervical erosion in detail from. DC Dutch book of gynecology
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have all the information needed to write a comprehensive, detailed answer. Here is the full explanation:
Important Note on Source
The library does not contain DC Dutta's Textbook of Gynecology. The closest available gynecology references are Berek & Novak's Gynecology and Harrison's Principles of Internal Medicine 22E - both authoritative sources that cover the same topic in detail. The content below is drawn from those sources and is consistent with what DC Dutta covers on this topic.
Cervical Erosion (Cervical Ectopy / Ectropion)
Terminology - The Modern Understanding
The term "cervical erosion" is a misnomer that has largely been abandoned in modern gynecology. As Harrison's (2025) states:
"Cervical ectopy, often mislabeled 'cervical erosion,' is easily confused with infectious endocervicitis."
The condition is more accurately called cervical ectopy or cervical ectropion. It is not a true erosion (i.e., there is no loss of epithelium) - the epithelium is completely intact. The red, raw-looking appearance on the exocervix that clinicians historically called an "erosion" is simply the normal columnar epithelium of the endocervical canal that has extended (everted) onto the visible ectocervix.
Normal Cervical Anatomy - The Foundation
To understand cervical erosion, the cervical anatomy must be clear.
The cervix is lined by two distinct epithelial types:
- Ectocervix: covered by stratified squamous epithelium (pale pink, opaque, glycogen-containing)
- Endocervical canal: lined by mucus-secreting columnar epithelium (red, glistening, single-cell layer)
The point where these two epithelia meet is the squamocolumnar junction (SCJ). This is not a fixed anatomical landmark - it is a dynamic, hormonally responsive boundary.
The area between the original SCJ and the physiologically active SCJ is the transformation zone (TZ) - the most important region of the cervix clinically, as it is where squamous neoplasia (CIN and cervical cancer) originates.
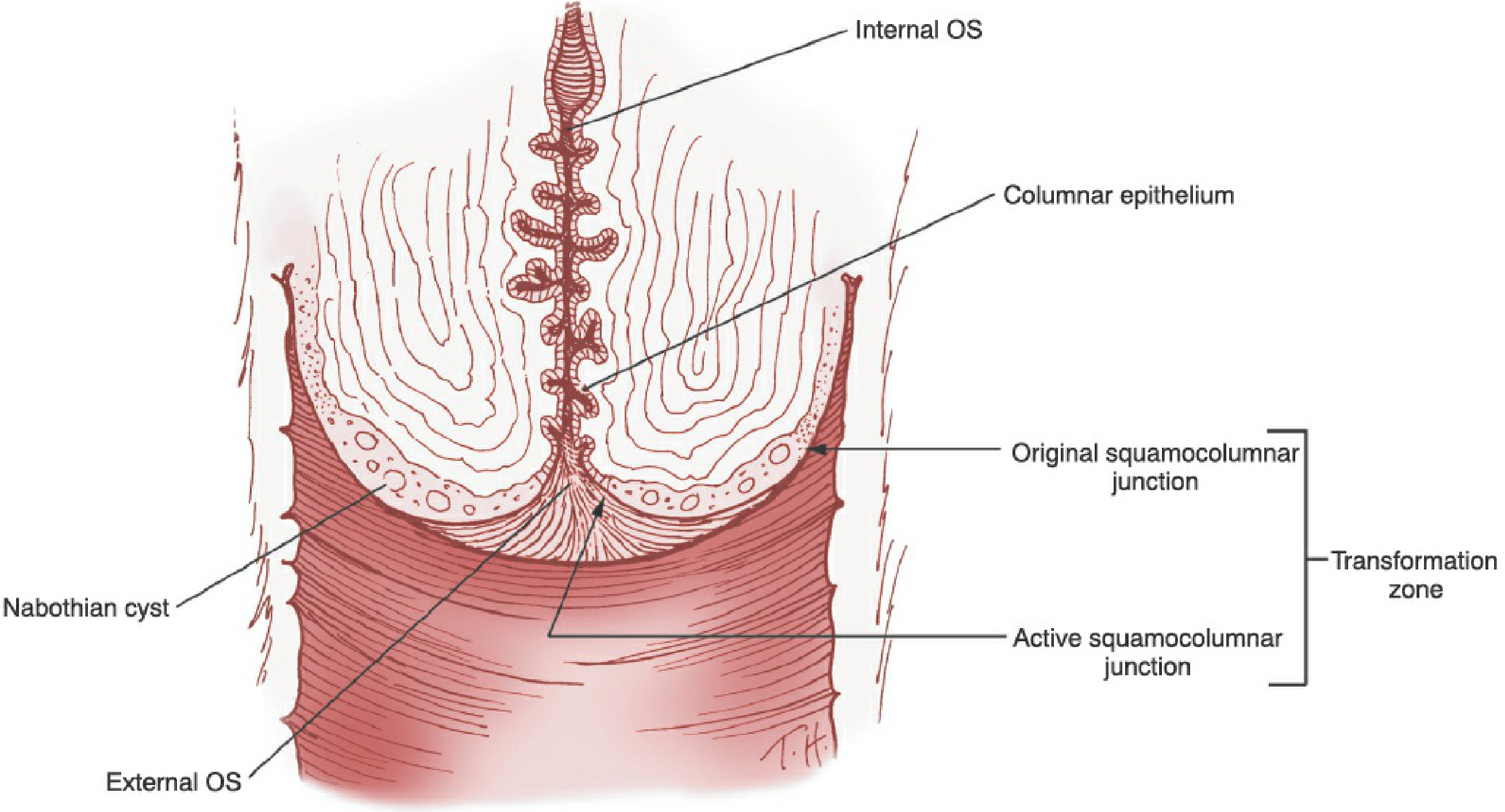
Berek & Novak's Gynecology, Fig. 16-3: The cervix and endocervix with the transformation zone clearly demarcated
Definition of Cervical Ectopy (Erosion)
Cervical ectopy is the extension of columnar (glandular) epithelium from the endocervical canal onto the visible exocervix. Because columnar epithelium is red and single-layered (vs. the thick, pale squamous epithelium), it appears as a red velvety area around the external os - giving the erroneous impression of a raw, eroded surface. The epithelium is, however, histologically intact.
Physiological Basis and Causes
The SCJ migrates in response to estrogen levels and other stimuli. Under high estrogen influence, the SCJ moves outward (eversion), exposing columnar epithelium on the ectocervix. This is a physiological process, not a pathological one.
As Berek & Novak states:
"In early childhood, during pregnancy, or with oral contraceptive use, columnar epithelium may extend from the endocervical canal onto the exocervix, a condition known as eversion or ectopy."
Factors that promote cervical ectopy:
| Factor | Mechanism |
|---|---|
| Puberty / menarche | Rising estrogen drives eversion of columnar epithelium |
| Pregnancy | High estrogen and progesterone cause maximal eversion |
| Oral contraceptive pills | Estrogen component favors persistence or reappearance of ectopy |
| Multiparity | Cervical eversion during repeated labor |
| Neonatal period | Transplacental maternal estrogen causes eversion at birth |
After menopause, estrogen levels fall and the transformation zone recedes entirely into the endocervical canal, making it invisible on speculum exam.
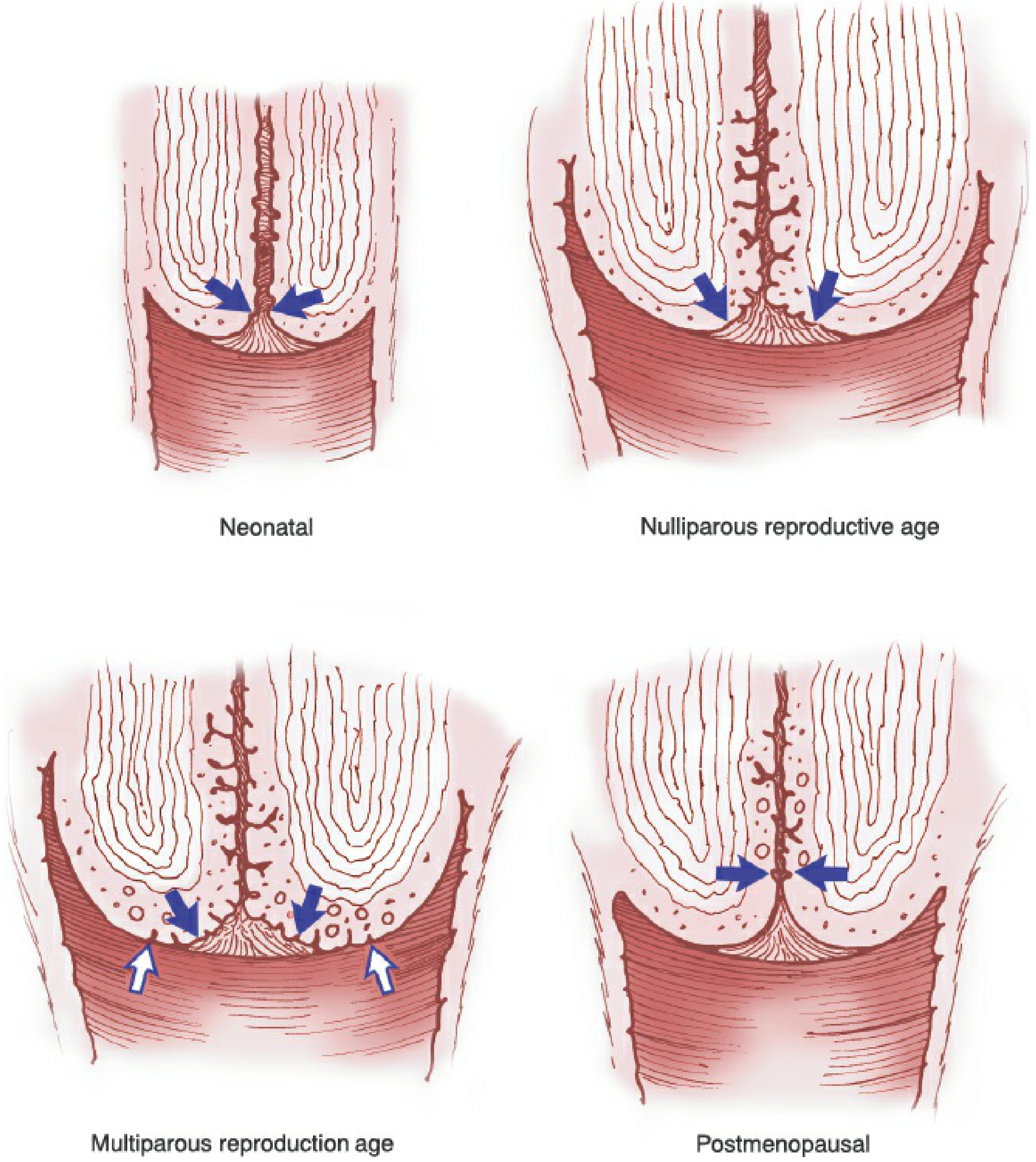
Berek & Novak's Gynecology, Fig. 16-4: Changes in the location of the transformation zone and SCJ throughout a woman's life. Blue arrows = internal boundary of SCJ; White arrows = external boundary of SCJ.
Histology
Columnar epithelium (seen in ectopy):
- A single layer of tall columnar cells
- Mucus granules at the apex, round nucleus at the base
- Composed of numerous ridges, clefts, and infoldings
- Technically these are not true glands, but the term "gland openings" is commonly used
Squamous epithelium (normal ectocervix) has four layers:
- Basal layer - single row of immature cells with large nuclei
- Parabasal layer - 2-4 rows, provide replacement cells
- Intermediate layer - 4-6 rows with polyhedral cells, intercellular bridges, glycogen differentiation begins
- Superficial layer - 5-8 rows of flattened cells, pyknotic nuclei, glycogen-filled; these exfoliate and form the basis of the Pap test
Squamous Metaplasia - The Natural Resolution
The body naturally replaces ectopic columnar epithelium with squamous epithelium through squamous metaplasia. This process happens via the subcolumnar reserve cells:
"Under stimulation of lower vaginal acidity, the reserve cells proliferate, lifting the columnar epithelium. The immature metaplastic cells have large nuclei and a small amount of cytoplasm without glycogen. As the cells mature normally, they produce glycogen, eventually forming the four layers of epithelium."
- Berek & Novak's Gynecology
Metaplasia starts at the tips of columnar villi (most exposed to acid pH) and progresses inward. As deeper clefts are replaced, trapped mucus-secreting cells form nabothian cysts - the retention cysts visible on the cervix that mark the original SCJ.
Factors influencing metaplasia rate:
- Oral contraceptives: favor persistence of ectopy (slow metaplasia)
- Smoking: reportedly accelerates squamous metaplasia
- Low vaginal pH: stimulates reserve cell proliferation
Clinical Presentation
Most cases are asymptomatic and found incidentally on speculum examination. When symptomatic, patients may report:
- Vaginal discharge - clear or mucoid, from columnar cell secretion
- Post-coital bleeding - the columnar epithelium is friable and bleeds easily on contact
- Intermenstrual spotting (less common)
On speculum examination:
- A red, velvety, well-demarcated area around the external os
- Usually involves the anterior and posterior lips of the cervix
- The os may contain clear or slightly cloudy mucus - not mucopurulent discharge
In cervicitis (which must be distinguished), the discharge is yellow-green (mucopus), and there is true inflammation.
Diagnosis and Distinguishing from Cervicitis
The key clinical challenge is distinguishing ectopy from infectious cervicitis (endocervicitis).
Ectopy:
- Clear or cloudy mucus, not mucopurulent
- Colposcopy shows intact epithelium with a characteristic villous (grape-like) red pattern
- The zone of ectopy is friable - bleeds when touched with a cotton swab or spatula
Cervicitis (endocervicitis):
- Yellow/green mucopurulent discharge
-
30 neutrophils per HPF on Gram stain
- Tests positive for N. gonorrhoeae or C. trachomatis on NAAT
- Ectropion may co-exist and predispose to STI acquisition
Clinical Significance
-
Susceptibility to STIs: Ectopy increases susceptibility to N. gonorrhoeae, C. trachomatis, and HIV because the thin, single-layered columnar epithelium is far less resistant to pathogen penetration than stratified squamous epithelium.
-
Increased risk of CIN: The transformation zone at the advancing SCJ is the zone where CIN originates. Metaplastic cells here are vulnerable to oncogenic stimuli (especially HPV). Changes are most active during menarche and after pregnancy when metaplasia is at its peak.
-
Nabothian cysts: When metaplasia traps mucus-secreting columnar cells under squamous epithelium, nabothian cysts form. These are benign retention cysts and require no treatment.
-
Diethylstilbestrol (DES) exposure: Intrauterine DES exposure (a banned synthetic estrogen) is associated with abnormalities including cervical erosion, ridges, and abnormal vaginal and uterine development.
Management
Cervical ectopy per se does not require treatment. Harrison's states unequivocally:
"Cauterization of ectopy is not warranted."
Indications for treatment are limited to symptomatic cases causing significant discharge or recurrent post-coital bleeding that distresses the patient. Options include:
- Cryotherapy (freezing)
- Electrocautery / diathermy (rarely used now)
- Laser ablation
- Cold coagulation
If ectopy is associated with cervicitis (infection), the infection is treated with appropriate antibiotics (dual therapy for gonorrhea + chlamydia coverage; see Berek & Novak Table 15-3).
Any women with ectopy should have routine cervical cytology (Pap smear) and HPV testing as per standard screening guidelines, since the transformation zone is the site of future neoplastic risk.
Summary Table
| Feature | Detail |
|---|---|
| Synonym | Cervical ectopy, cervical ectropion, eversion |
| Nature | Physiological (not pathological) eversion of columnar epithelium onto exocervix |
| Cause | Estrogen stimulation (puberty, pregnancy, OCPs, neonates) |
| Histology | Single-layer columnar epithelium (intact - no true erosion) |
| Appearance | Red, velvety area around external os |
| Symptoms | Mostly asymptomatic; mucoid discharge, post-coital bleeding |
| Key risk | Susceptibility to STIs (chlamydia, gonorrhea, HIV); CIN in transformation zone |
| Natural resolution | Squamous metaplasia replaces columnar epithelium over time |
| Treatment | Usually none required; treat only if symptomatic |
| Nabothian cysts | Result from trapped mucus glands during metaplasia; benign |
Sources: Berek & Novak's Gynecology (16th ed.), pp. 179, 815, 835-841; Harrison's Principles of Internal Medicine 22E (2025), Cervical Ectopy section
Note: DC Dutta's Textbook of Gynecology was not available in the library. The content above is drawn from Berek & Novak's Gynecology and Harrison's - both at least equivalent in authority to DC Dutta. The clinical content on cervical erosion/ectopy is consistent across all major gynecology texts. If you have access to a specific edition of DC Dutta, I can help you cross-reference any chapter or passage.
This is a shared conversation. Sign in to Orris to start your own chat.