Champys principle of osteosynthesis
Reading File
Finding Sources
Searching the Web
Champy principle of osteosynthesis mandible ideal lines fixation
Reading File
Reading File
Reading File
Loading Image
I now have enough information from the textbooks and web search to provide a complete, well-structured answer.
Champy's Principle of Osteosynthesis
Background
Maxime Champy and colleagues introduced their concept of ideal osteosynthesis lines in the 1970s (Champy M, Lodde JP, Muster D, et al., Ann Chir Plast Esthet, 1977). This work established the biomechanical basis for miniplate fixation of mandibular fractures and remains the foundation of modern oral and maxillofacial fracture management.
Core Concept: Load-Sharing Fixation
Champy's technique is a form of load-sharing osteosynthesis - in contrast to the load-bearing approach of the AO/ASIF (Association for Osteosynthesis). The difference is critical:
| Feature | Champy (Load-Sharing) | AO/ASIF (Load-Bearing) |
|---|---|---|
| Plate type | Miniplate | Large, rigid reconstruction plate |
| Screw type | Monocortical | Bicortical |
| Plate function | Neutralizes tensile forces only | Overcomes ALL forces |
| Bone contact | Required for compression | Not required |
| Fracture type | Simple, non-comminuted | Comminuted, bone-deficient |
The Champy technique relies on bone surface contact at the fracture site to handle compressive forces, while the miniplate handles only tensile (distractive) forces. This is why it is NOT suitable for comminuted fractures where bone contact is lost.
Biomechanical Basis
During mandibular function (mastication), two opposing forces act on the mandible:
- Superior border = Tension zone - bone tends to be pulled apart here
- Inferior border = Compression zone - bone is pushed together here
Champy's key insight: placing a plate along the superior border (tension zone) neutralizes the harmful tensile forces while allowing the beneficial compressive forces at the inferior border to promote bone healing.
Torsional forces between the canines (symphysis/parasymphysis region) are the most complex - this region experiences significant twisting forces requiring two plates rather than one.
Ideal Lines of Osteosynthesis
These are anatomically specific lines where miniplates should be placed for optimal stability:
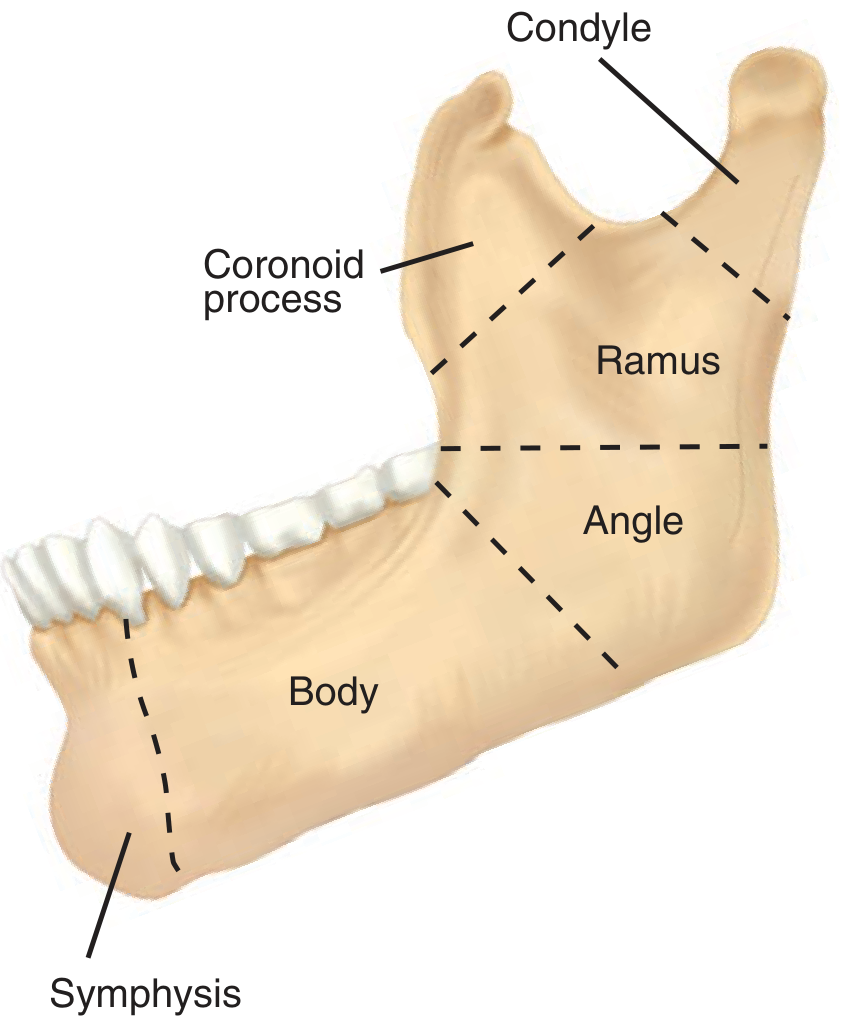
1. Symphysis and Parasymphysis (anterior mandible)
- Two plates required due to high torsional forces in this region
- Superior plate: along the level of the tooth roots (~5 mm below alveolar crest)
- Inferior plate: near the inferior border
- Plates must be at least 5 mm apart to prevent stress concentration and hardware failure
2. Body of the Mandible
- Single plate placed along the external oblique ridge, at the level of the tooth roots
- Must remain below tooth roots and above the inferior alveolar nerve canal
3. Angle of the Mandible
- Single plate placed either:
- Superiorly, on the external oblique ridge (behind the last molar) - preferred by Champy; allows splay at inferior angle to close over time
- Laterally, on the lateral border - technically more demanding
- Only one of the two Champy lines at the angle needs a plate
4. Ramus
- Single plate along the posterior or lateral surface
Technical Features
- Monocortical screws - only the outer cortex is engaged; protects roots and inferior alveolar nerve
- Intraoral approach - reduces external scarring and dissection
- Malleable miniplates - thin (2 mm), easily adapted to bone contour
- No intermaxillary fixation (IMF) required in most cases - a major patient benefit
- Introduced originally as stainless steel plates; now titanium is standard
Indications and Contraindications
Ideal for:
- Simple (non-comminuted) fractures
- Fractures with adequate bone stock (load-sharing is possible)
- Mandibular angle fractures (the region Champy's technique is best suited for)
Not appropriate for:
- Comminuted fractures (bone contact lost - no compression possible)
- Fractures with significant bone loss
- These require load-bearing reconstruction plates with bicortical screws
Comparison with AO Technique
As noted in Schwartz's Principles of Surgery (11th ed.), mandibular bracing follows two schools: rigid fixation (AO/ASIF) and less rigid but functionally stable fixation (Champy technique). Both are valid; the key principle shared by both is to release maxillomandibular fixation and begin range of motion as soon as possible to prevent temporomandibular joint ankylosis. - Schwartz's Principles of Surgery, 11th Ed., p. 2030
Summary Table
| Region | Number of Plates | Plate Position |
|---|---|---|
| Symphysis / Parasymphysis | 2 | Superior (subapical) + Inferior border |
| Body | 1 | External oblique ridge / subapical |
| Angle | 1 | External oblique ridge or lateral border |
| Ramus | 1 | Lateral surface |
The key rule is: the more anterior the fracture, the more torsional the force, and the more fixation points are needed. This is why symphyseal fractures always need two plates while angle fractures need only one.
This is a shared conversation. Sign in to Orris to start your own chat.