Aednomyosis
Reading File
Finding Sources
Searching PubMed
adenomyosis
Searching the Web
adenomyosis clinical overview diagnosis treatment 2025
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive information from multiple authoritative textbooks. Here is a complete overview:
Adenomyosis
Definition
Adenomyosis is the presence of endometrial glands and stroma within the myometrium (uterine smooth muscle), accompanied by reactive smooth muscle hypertrophy and hyperplasia. The ectopic endometrial tissue may be diffuse (spread throughout the myometrium) or focal (forming a localized mass called an adenomyoma). It is considered the "internal" counterpart of endometriosis.
- Robbins & Kumar Basic Pathology, p. 608
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 929
Epidemiology
- Prevalence ranges widely (1%-70%) due to variable diagnostic criteria - historically it was only diagnosed histologically after hysterectomy
- Most commonly diagnosed in the 4th and 5th decades of life
- Found in 10%-88% of hysterectomy specimens
- 33% of cases are asymptomatic
- A 2025 systematic review (PMID: 41257733) is currently the most up-to-date estimate of global prevalence
Pathogenesis
The exact mechanism is not fully established. Leading theories include:
- Invagination/direct extension theory - endometrial tissue invades downward into the myometrium, possibly facilitated by disruption of the endometrial-myometrial junction
- Metaplastic theory - müllerian remnants or stem cells within the myometrium undergo endometrial differentiation
- Iatrogenic/trauma theory - uterine instrumentation (caesarean section, curettage, surgical termination) disrupts the endometrial-myometrial interface, allowing invasion
The ectopic tissue induces reactive myometrial hypertrophy, leading to uterine enlargement.
Risk Factors
| Category | Factors |
|---|---|
| Hormonal | Early menarche (≤10 years), short cycles (≤24 days), elevated BMI, oral contraceptive use, tamoxifen, prolonged oestrogen exposure |
| Reproductive | Increasing parity, multiple pregnancies, spontaneous miscarriage |
| Iatrogenic | Caesarean section, endometrial curettage, surgical termination, endometrial ablation, leiomyomas breaching the endometrial-myometrial interface |
| Comorbidities | Endometriosis, endometrial hyperplasia |
- Bailey and Love's Short Practice of Surgery, 28th ed., p. 1604
Clinical Features
Symptoms (classic triad):
- Dysmenorrhoea - often severe, worsening just before menstruation
- Menorrhagia (abnormal uterine bleeding) - occurs in 40%-60% of patients; caused by increased endometrial surface area, increased gland volume, and greater vascularisation
- Chronic pelvic pain / dyspareunia
- Subfertility
Signs:
- Enlarged, globular, tender uterus - typically symmetrically enlarged ("boggy uterus")
- Uterine tenderness on palpation
- Note: 33% of patients are asymptomatic
Adenomyosis is part of the PALM-COEIN classification (A = adenomyosis) used by ACOG for evaluating abnormal uterine bleeding.
Diagnosis
Transvaginal Ultrasound (TVUS)
First-line imaging; accuracy 68%-86% for diffuse adenomyosis (lower for focal disease or coexisting fibroids).
MUSA (Morphological Uterus Sonographic Assessment) criteria - at least 3 of the following features are required:
- Enlarged globular uterus with asymmetric myometrial thickening
- Myometrial cysts (2-6 mm subendometrial cysts, seen in ~50%) representing haemorrhagic foci
- Echogenic subendometrial linear striations
- Hyperechogenic islands / diffuse echogenic nodules
- Fan-shaped shadowing
- Irregular junctional zone
- Poor definition of the endometrial-myometrial interface
- "Rain shower" appearance - multiple fine areas of attenuation
- Speckled colour Doppler vascularity pattern
MRI (gold standard imaging)
MRI is superior for distinguishing adenomyosis from fibroids and for pre-surgical planning.
On T2-weighted images:
- Diffuse or focal thickening of the junctional zone (JZ) with low signal intensity (due to smooth muscle hyperplasia)
- JZ ≥ 12 mm - predicts adenomyosis with high accuracy
- JZ ≤ 8 mm - excludes adenomyosis with high accuracy
- JZ 8-12 mm - indeterminate; ancillary criteria used:
- High T2 signal foci within low-signal myometrium (ectopic endometrial islands)
- High T1 signal foci = punctate haemorrhage within ectopic tissue (95% PPV for adenomyosis)
- Linear T2 striations extending from endometrium into myometrium ("finger-like projections")
- Cystic adenomyosis - high T1 and intermediate-low T2 foci (extensive haemorrhagic ectopic endometrium)
MRI mimics: myometrial contractions, endometrial carcinoma, fibroids
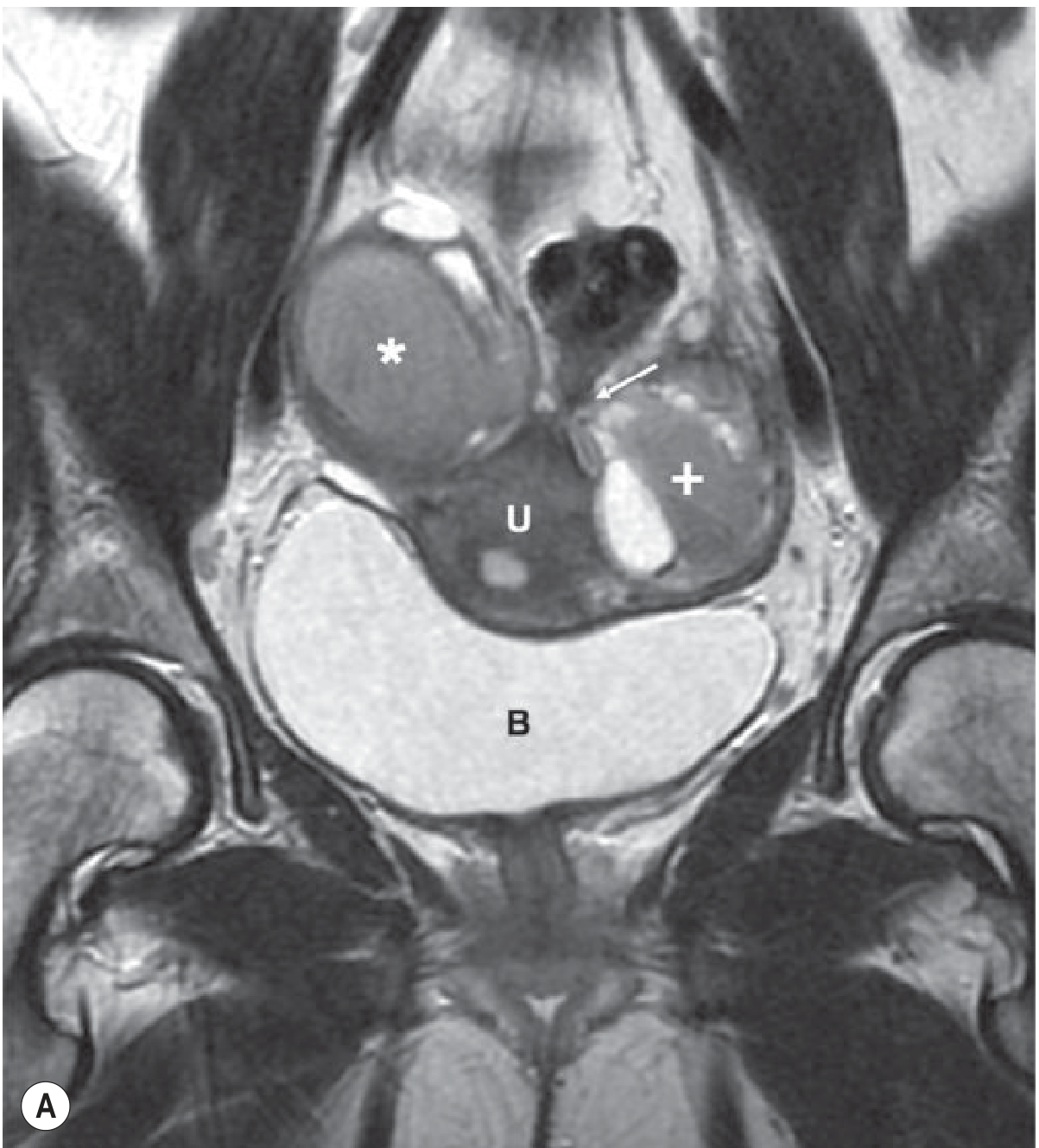
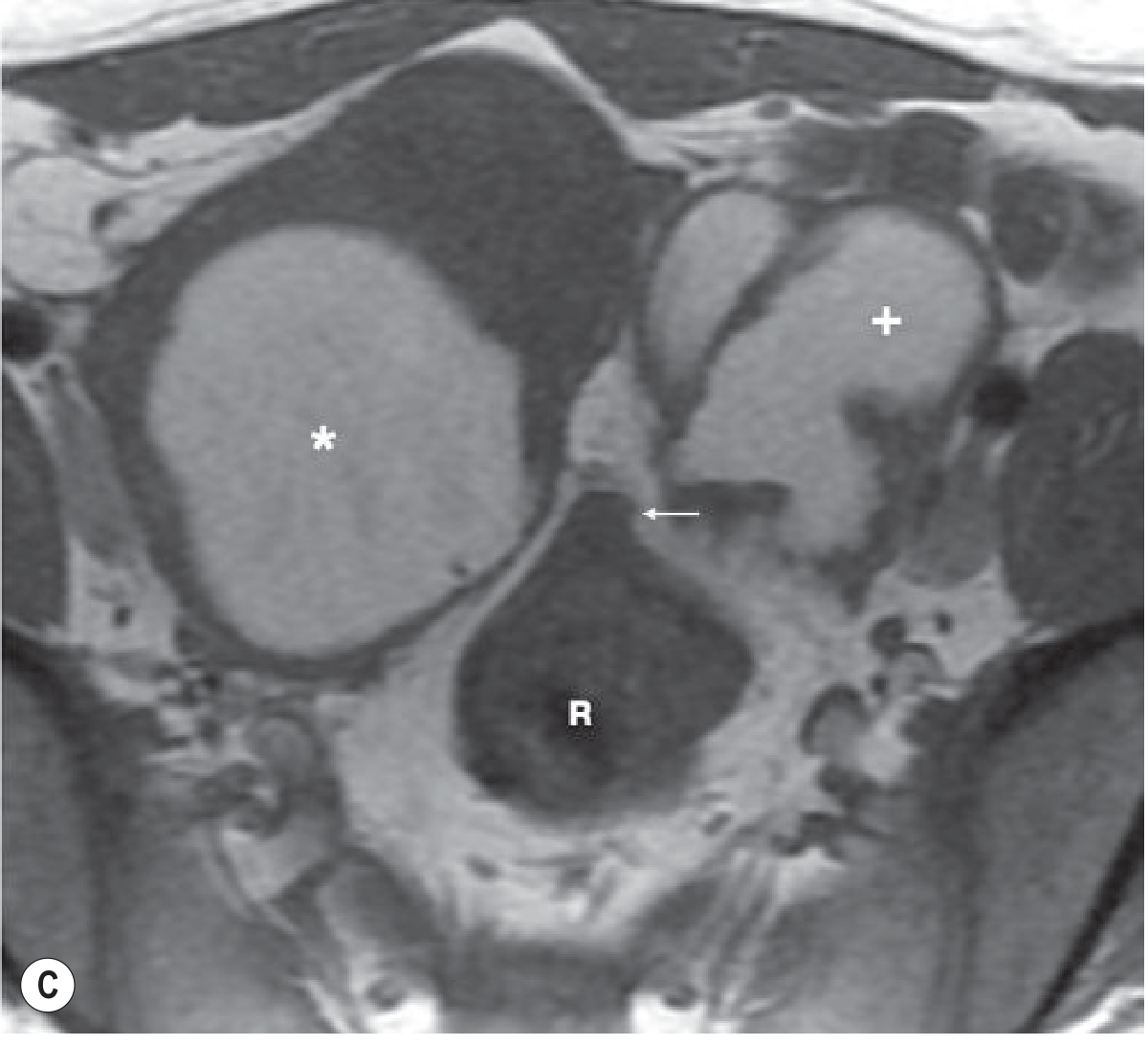
Below are MRI images showing adenomyosis (coronal and axial T2-weighted pelvis):
Histology (gold standard for diagnosis)
-
Endometrial glands and stroma >2.5 mm below the basalis layer within the myometrium
-
Historically only confirmed at hysterectomy
-
Reactive smooth muscle hyperplasia surrounds the ectopic tissue
-
Grainger & Allison's Diagnostic Radiology, p. 898
Management
Treatment depends on symptom severity, age, and desire for future fertility.
Medical (conservative first-line)
| Drug Class | Examples | Notes |
|---|---|---|
| Analgesics | NSAIDs | First-line for dysmenorrhoea |
| Hormonal contraceptives | Combined oral contraceptive pill | Menstrual suppression |
| Progestogens | Levonorgestrel IUS (Mirena - off-label), dienogest, medroxyprogesterone acetate | LNG-IUS is very effective; dienogest increasingly preferred |
| GnRH agonists | Leuprolide, goserelin | Induces pseudomenopause; limited to 6 months without add-back due to bone loss |
| GnRH antagonists | Relugolix, elagolix | Newer options; oral administration |
| Danazol | - | Androgenic side-effects limit use |
| Aromatase inhibitors | Letrozole | For refractory cases |
| Selective progesterone receptor modulators (SPRMs) | Ulipristal acetate | Under investigation |
Radiological / Minimally Invasive
- Uterine Artery Embolisation (UAE) - effective for symptom relief; complications include post-embolisation syndrome (pain, nausea, fever), haemorrhage, radiation exposure, age-related impairment of ovarian reserve
- High-Intensity Focused Ultrasound (HIFU) / MR-guided Focused Ultrasound (MRgFUS) - non-invasive ablation; adverse effects include abdominal pain, skin burns, sciatic nerve injury from thermal spread, and rarely intestinal perforation
Surgical (uterus-preserving - adenomyomectomy)
For patients who desire fertility preservation:
- Non-excisional techniques - thermal coagulation of diseased myometrium
- Partial reduction surgeries - for diffuse adenomyosis: wedge resections, wedge-shaped uterine wall removal, modified reductive surgery, transverse H-incisions
- Complete adenomyotic excision - for focal adenomyosis: double- or triple-flap method, asymmetric dissection method
Definitive Surgical Treatment
-
Hysterectomy - the only cure; recommended when fertility is no longer desired and medical/conservative treatment has failed
-
Berek & Novak's Gynecology, p. 581; Bailey and Love's, p. 1604
Relationship to Fertility
Adenomyosis is associated with subfertility and adverse obstetric outcomes. A 2024 systematic review (PMID: 39049473) found independent effects of adenomyosis on maternal, placental, fetal, and neonatal outcomes even after accounting for endometriosis and ART-related factors. Lesion type, location, and junctional zone thickness are strong predictors of fertility outcomes.
Key Distinguishing Features vs. Endometriosis
| Feature | Adenomyosis | Endometriosis |
|---|---|---|
| Location of ectopic tissue | Within myometrium | Outside uterus |
| Typical age | 4th-5th decade | 3rd-4th decade |
| Uterus | Enlarged, globular | Usually normal size |
| Malignant transformation | Not reported | Rare (peritoneal/ovarian types) |
| Diagnosis | TVUS / MRI / histology | Laparoscopy / histology |
Recent evidence note: A 2025 meta-analysis (PMID: 41257733) provides updated global prevalence data for both adenomyosis and endometriosis. A 2024 systematic review (PMID: 39067674) examined functional uterine contractility determinants in both conditions - relevant to understanding symptom generation and fertility impact.
This is a shared conversation. Sign in to Orris to start your own chat.