Hydrocele with vercio veins
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from the textbooks. Let me compile a thorough answer.
Hydrocele and Varicocele
Hydrocele
Definition
A hydrocele is an abnormal collection of serous fluid within the tunica vaginalis (or a patent processus vaginalis) surrounding the testis. - Bailey & Love's Surgery, 28th ed.
Incidence
- Affects ~1% of adult men
-
80% of newborns have a patent processus vaginalis, but most close spontaneously within 18 months
Types (Structural Classification)
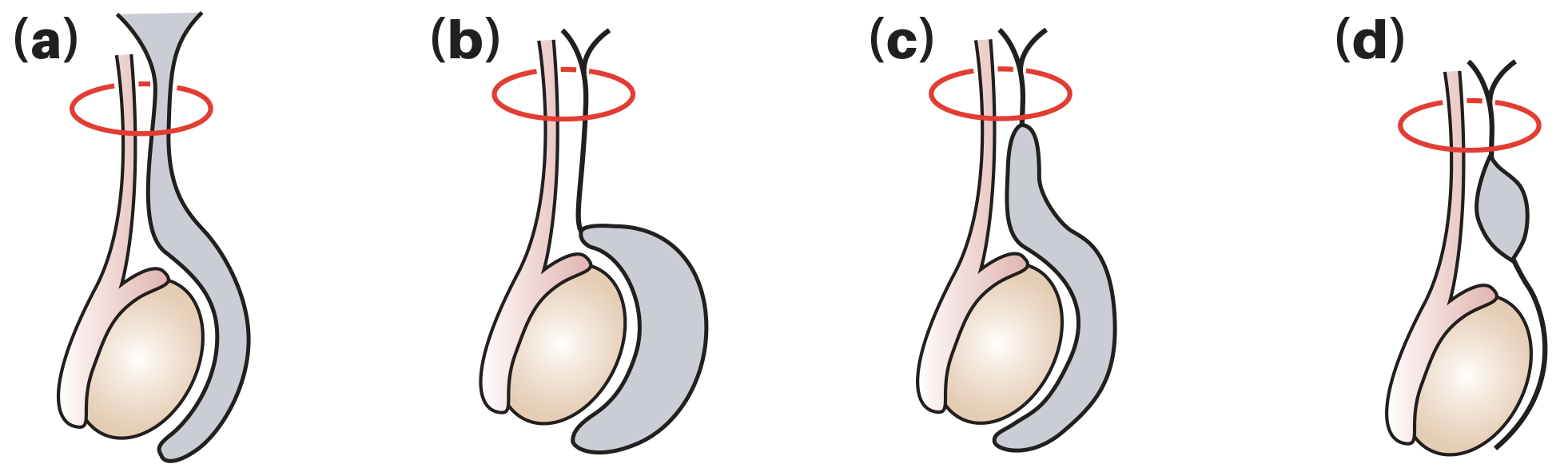
(a) Vaginal/primary hydrocele - most common; (b) Infantile hydrocele; (c) Congenital/communicating hydrocele; (d) Hydrocele of the cord
| Type | Description |
|---|---|
| Communicating (congenital) | Patent processus vaginalis allows peritoneal fluid to flow into the scrotum; associated with indirect inguinal hernia |
| Non-communicating (vaginal) | Processus closed; fluid accumulates due to excessive production or defective lymphatic absorption by the tunica vaginalis |
| Infantile hydrocele | Proximal processus patent, distal closed; fluid trapped mid-cord |
| Hydrocele of the cord | Both ends of processus closed, mid-portion patent - forms a smooth oval swelling above the testis |
Secondary hydroceles occur in men >40 years - caused by local injury, torsion, infection, neoplasm, or radiotherapy. If a tumour is suspected, do NOT puncture the hydrocele (risk of malignant needle-track implantation). - Bailey & Love
Clinical Features
- Usually painless, may grow to a large size before presentation
- Can get "above" the swelling (unlike inguinal hernia)
- Testis/epididymis may be impalpable within the fluid
- Transilluminates (fluid-filled = translucent)
- Scrotal ultrasound is the key adjunct to assess the underlying testis
Treatment
- Small hydroceles: no treatment needed
- Congenital: herniotomy (ligation of patent processus vaginalis)
- Sizeable/symptomatic acquired hydroceles - three surgical options:
- Plication (Lord's operation) - suitable for thin-walled sacs; minimal dissection, low haematoma risk
- Eversion (Jaboulay's operation) - sac is everted behind the testis
- Excision - for thick-walled sacs
Varicocele ("Vercio Veins")
Definition
A varicocele is an abnormal dilatation and enlargement of the pampiniform plexus (scrotal venous plexus draining the testis). - Bailey & Love
Incidence
- Affects 10-20% of adult males
- Found in ~40% of infertile males
- ~90% are left-sided (left testicular vein drains into the higher-pressure left renal vein; right drains directly into the IVC)
- If a solitary right-sided varicocele is found, always image the kidney to exclude a retroperitoneal mass or renal tumour
Pathophysiology - 3 Theories
- Absent/incompetent valves at the junction of the testicular vein with the renal vein (left) or IVC (right) - allows retrograde venous reflux
- "Nutcracker" effect - left testicular vein compressed between the superior mesenteric artery and the aorta
- Angulation at the junction of the left testicular vein and left renal vein
Grading (WHO / Clinical Classification)
| Grade | Description |
|---|---|
| Subclinical | Not palpable or visible; detected only by Doppler ultrasound |
| Grade 1 | Palpable only during Valsalva manoeuvre |
| Grade 2 | Palpable at rest, not visible |
| Grade 3 | Visible and palpable at rest ("bag of worms") |
Clinical Features
- Often asymptomatic; may cause dragging discomfort, worse on standing at end of day
- Affected side of scrotum hangs lower
- "Bag of worms" feel on palpation in the erect position
- Veins decompress on lying down (if they do not decompress supine - suspect underlying venous obstruction/renal tumour)
- Longstanding cases: testicular atrophy on the affected side
Varicocele and Infertility - Key Mechanisms
- Elevated intratesticular temperature (primary mechanism) - impairs countercurrent heat exchange in the pampiniform plexus
- Increased oxidative stress and sperm DNA fragmentation
- Testicular hypoperfusion and stasis - hypoxia and toxin accumulation
- Elevated apoptosis-associated microRNA in seminal fluid
- Results: reduced sperm count, motility, morphology, testicular atrophy, and lower testosterone - Campbell Walsh Wein Urology
Treatment
- Percutaneous (radiological) embolisation of the gonadal veins - usual first-line when discomfort is significant
- Varicocelectomy (surgical repair) - recommended in men with low sperm count + clinical varicocele + unexplained infertility
- Microsurgical (subinguinal) approach using the operating microscope is the gold standard - lowest recurrence, lowest hydrocele rate
- Open inguinal (Ivanissevich) or laparoscopic approaches also used
- Treatment of subclinical varicocele or men with normal semen parameters does not improve spontaneous pregnancy rates
The Key Connection: Post-Varicocelectomy Hydrocele
This is a critical relationship between the two conditions:
- Hydrocele formation is the most common complication of varicocelectomy
- Incidence: 3-33% (average ~7%) after non-microscopic approaches
- Cause: lymphatic obstruction during cord dissection - confirmed by protein concentration analysis of hydrocele fluid
- At least half of post-varicocelectomy hydroceles grow large enough to require surgical excision
- A large post-op hydrocele creates an insulating layer around the testis, which may impair counter-current heat exchange and partly negate the fertility benefit of the varicocelectomy
- Prevention: Using magnification (loupes or operating microscope) to identify and preserve lymphatics almost eliminates the risk - this is the main advantage of the microscopic subinguinal approach - Campbell Walsh Wein Urology
| Approach | Hydrocele Rate | Notes |
|---|---|---|
| Non-microscopic (open) | 3-33% | Lymphatics not consistently identified |
| Microscopic (subinguinal) | <1% | Lymphatics preserved under magnification |
| Laparoscopic | Intermediate | Lymphatic injury possible |
| Radiological embolisation | Very low | No cord dissection |
Bailey & Love's Short Practice of Surgery 28th ed. | Campbell Walsh Wein Urology
This is a shared conversation. Sign in to Orris to start your own chat.