hi
Hi! How can I help you today?
tell me about diabetes in detail
Reading File
search_medical_text
diabetes mellitus types etiology pathophysiology
search_medical_text
diabetes mellitus diagnosis clinical features complications management
search_medical_image
diabetes mellitus pathophysiology insulin glucose diagram
GradeResponse
GradeResponse
GradeResponse
Diabetes Mellitus — A Comprehensive Overview
What Is Diabetes?
Diabetes mellitus (DM) is a group of metabolic disorders of carbohydrate metabolism in which glucose is both underutilized and over-produced, resulting in chronic hyperglycemia (elevated blood glucose). It stems from defects in insulin secretion, insulin action, or both. (Laboratory Analysis in the Diagnosis and Management of Diabetes Mellitus, p. 1)
Classification
| Type | Core Mechanism | Key Features |
|---|---|---|
| Type 1 DM | Autoimmune destruction of pancreatic β-cells | Absolute insulin deficiency; usually juvenile onset |
| Type 2 DM | Insulin resistance + relative insulin deficiency | Most common (~90–95%); strongly linked to obesity |
| Gestational DM (GDM) | Resembles T2DM; occurs in pregnancy | Affects ~17% of pregnancies; remits post-delivery |
| MODY | Monogenic defects in β-cell function | Autosomal dominant; often misdiagnosed as T1 or T2 |
| Secondary DM | Due to other diseases (pancreatitis, Cushing's, drugs) | Varies by cause |
Pathophysiology
Type 1 DM
- Autoimmune T-cell mediated destruction of islet β-cells
- Leads to absolute insulin deficiency
- Without insulin, glucose cannot enter cells → hyperglycemia
- Fat breakdown accelerates → diabetic ketoacidosis (DKA) risk
Type 2 DM
- Begins with peripheral insulin resistance (muscle, liver, fat cells)
- β-cells compensate by secreting more insulin initially
- Over time, β-cells exhaust and insulin secretion declines
- Result: progressive hyperglycemia
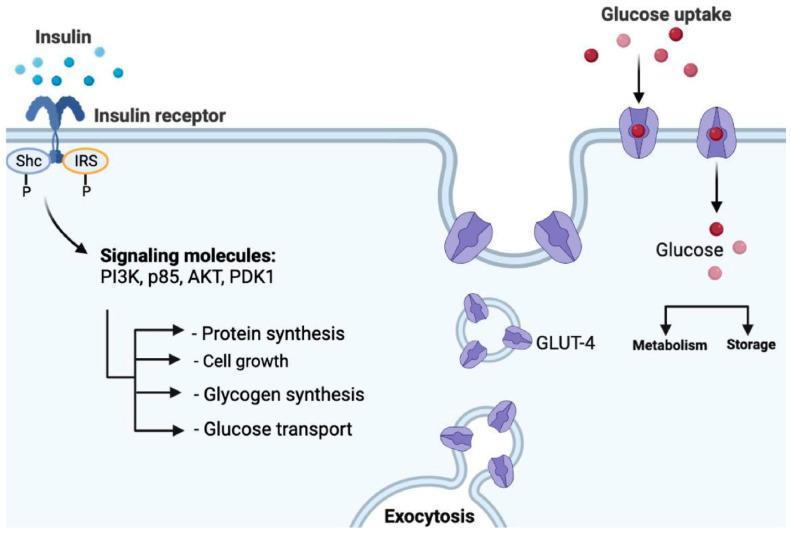
The diagram below illustrates the insulin signaling pathway at the cellular level — showing how insulin normally drives glucose uptake via GLUT-4 transporters, and where this cascade breaks down in T2DM:
Clinical Features
Symptoms of Hyperglycemia ("The 3 Polys")
- Polyuria — frequent urination (osmotic diuresis)
- Polydipsia — excessive thirst
- Polyphagia — increased hunger despite eating
- Weight loss (especially T1DM)
- Fatigue, blurred vision, slow wound healing
T1 vs T2 Presentation
| Feature | Type 1 | Type 2 |
|---|---|---|
| Onset | Sudden, often childhood | Gradual, usually adult |
| Body habitus | Normal/thin | Often overweight/obese |
| Ketosis | Common | Rare (unless stressed) |
| Family history | Less prominent | Strong |
| Autoantibodies | Present (GAD, IA-2) | Absent |
Diagnosis
(AACE Comprehensive Care Plan 2022, p. 2)
Any one of the following criteria is diagnostic:
| Test | Diagnostic Threshold |
|---|---|
| Fasting Plasma Glucose (FPG) | ≥ 126 mg/dL (7.0 mmol/L) |
| 2-hour Plasma Glucose (OGTT) | ≥ 200 mg/dL (11.1 mmol/L) |
| HbA1c | ≥ 6.5% (48 mmol/mol) |
| Random Plasma Glucose + symptoms | ≥ 200 mg/dL |
Prediabetes:
- FPG: 100–125 mg/dL
- HbA1c: 5.7–6.4%
- 2-hr OGTT: 140–199 mg/dL
Monitoring
- HbA1c: reflects average blood glucose over ~3 months; target generally < 7% for most adults
- Self-monitoring of blood glucose (SMBG): capillary finger-stick
- Continuous Glucose Monitoring (CGM): real-time glucose trends; recommended for T1DM and many T2DM patients on insulin
Management
Lifestyle (Foundation for All Types)
- Medical nutrition therapy (low glycemic index diet, calorie control)
- Physical activity: ≥150 min/week moderate aerobic exercise
- Weight loss in overweight T2DM patients (even 5–10% is beneficial)
Pharmacotherapy — Type 2 DM
| Drug Class | Examples | Mechanism | Notes |
|---|---|---|---|
| Biguanides | Metformin | ↓ hepatic glucose production | First-line agent |
| GLP-1 agonists | Semaglutide, liraglutide | ↑ insulin, ↓ glucagon, ↓ appetite | CV and weight benefits |
| SGLT-2 inhibitors | Empagliflozin, dapagliflozin | ↑ urinary glucose excretion | CV & renal protective |
| DPP-4 inhibitors | Sitagliptin | ↑ incretin activity | Weight neutral |
| Sulfonylureas | Glipizide, glibenclamide | ↑ insulin secretion | Hypoglycemia risk |
| Thiazolidinediones | Pioglitazone | ↑ insulin sensitivity | Weight gain, fluid retention |
| Insulin | Various formulations | Replaces/supplements insulin | Required in T1DM; used in T2DM |
Insulin Therapy — Type 1 DM
- Basal-bolus regimen is standard (long-acting + rapid-acting insulin)
- Insulin pump (CSII) + CGM ("closed loop" / artificial pancreas) increasingly used
Complications
Microvascular
| Complication | Organs Affected | Key Features |
|---|---|---|
| Diabetic Retinopathy | Eyes | Leading cause of blindness in working adults |
| Diabetic Nephropathy | Kidneys | Leading cause of end-stage renal disease |
| Diabetic Neuropathy | Peripheral nerves | Burning/numbness in feet ("glove & stocking") |
Macrovascular
- Coronary artery disease (CAD) — 2–4× higher risk
- Stroke — 2× higher risk
- Peripheral artery disease (PAD) — diabetic foot ulcers, gangrene
Acute Complications
| Condition | Type | Key Features |
|---|---|---|
| DKA | Mainly T1DM | Ketones, acidosis, vomiting, Kussmaul breathing |
| HHS | Mainly T2DM | Severe hyperglycemia (>600 mg/dL), hyperosmolarity, no ketosis |
| Hypoglycemia | Both | Glucose < 70 mg/dL; sweating, confusion, seizures |
Comorbidities & Special Populations
- Hypertension: Target BP < 130/80 mmHg; ACE inhibitors/ARBs preferred (nephroprotective)
- Dyslipidemia: Statins recommended for most adults with DM
- Obesity: Bariatric surgery can induce T2DM remission in eligible patients
- Pregnancy: GDM managed with diet, monitoring; insulin if needed (metformin/glyburide debated)
- Children: Increasing T2DM in adolescents due to obesity epidemic; T1DM managed with insulin ± CGM
Prevention
- T2DM is largely preventable: lifestyle intervention (diet + exercise) reduces progression from prediabetes by ~58%
- Metformin reduces T2DM risk in high-risk prediabetes patients
- T1DM prevention remains investigational (immune modulation trials ongoing)
Prognosis
With good glycemic control and management of risk factors, people with diabetes can live long, healthy lives. Poorly controlled DM significantly shortens life expectancy and quality of life due to its complications. The AACE 2022 Comprehensive Care Plan emphasizes a person-centered, team-based approach with individualized glycemic targets as the cornerstone of modern diabetes care.
Sources: Laboratory Analysis in the Diagnosis and Management of Diabetes Mellitus (p. 1); AACE Developing a Diabetes Mellitus Comprehensive Care Plan 2022 Update (p. 2)
This is a shared conversation. Sign in to Orris to start your own chat.