Craniopharyngeoma complications and treatment
Reading File
Finding Sources
Searching PubMed
craniopharyngioma treatment outcomes
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content from multiple authoritative sources. Let me compile the full answer.
Craniopharyngioma: Complications and Treatment
Overview
Craniopharyngioma is a slow-growing, histologically benign epithelial tumor arising from remnants of Rathke's pouch. It accounts for 2%-5% of all CNS tumors and 3%-5% of pediatric brain tumors. Despite its benign histology, its location near the hypothalamus, pituitary stalk, and optic structures gives it outsized clinical consequences. There is a bimodal age distribution: a childhood peak at 5-14 years and an adult peak at 50-60 years.
Two subtypes:
- Adamantinomatous (90%): more common in children; mixed solid/cystic with calcifications; CTNNB1 (beta-catenin) mutations (~94%)
- Papillary (10%): predominant in adults; mostly solid, rarely calcified; BRAF V600E mutations (~95%)
Imaging
Sagittal T1-weighted MRI showing a large craniopharyngioma with the optic chiasm compressed against the tumor surface:
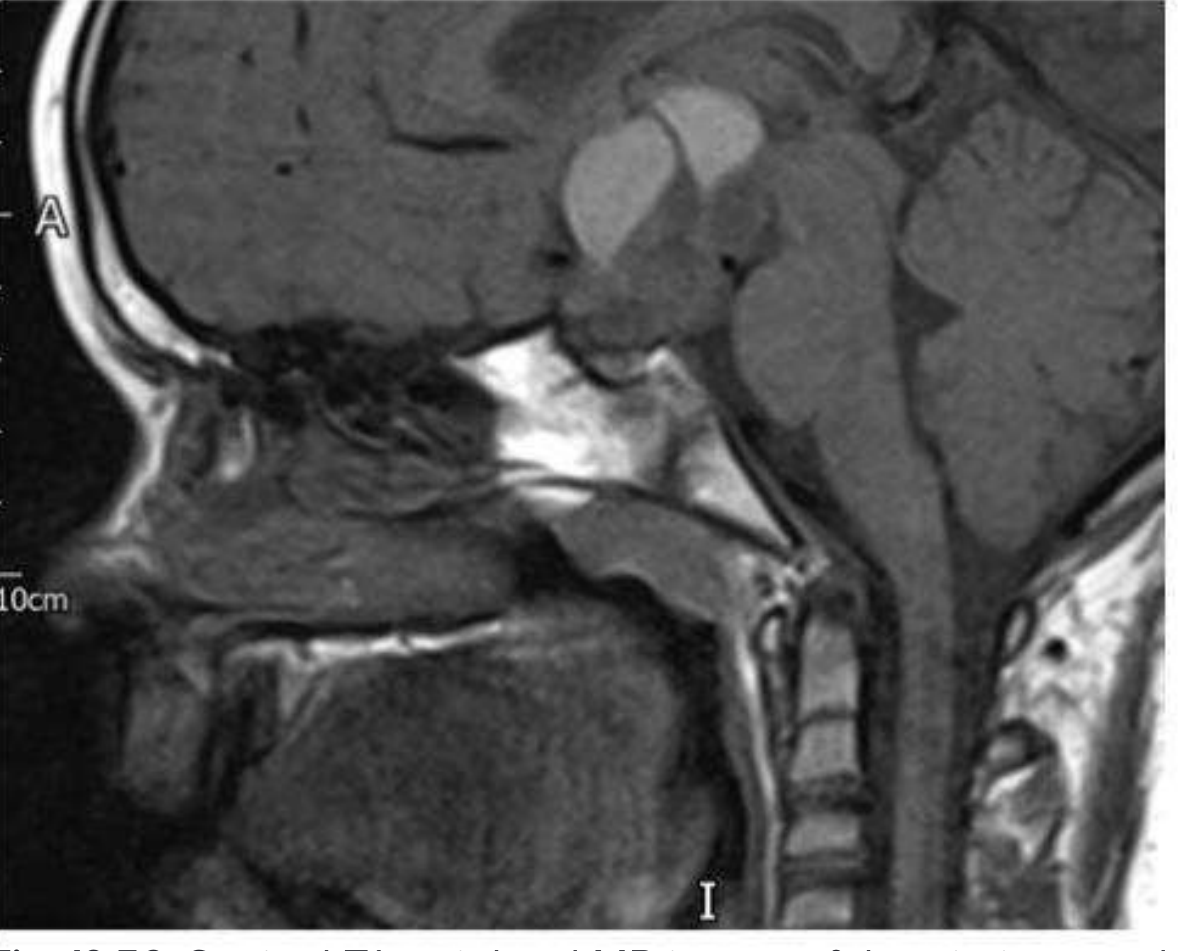
Fig. 19.56 from Kanski's Clinical Ophthalmology
Sagittal post-contrast MRI showing a partially solid retrosellar mass with patchy enhancement and non-enhancing anterior cystic components, with pituitary tissue compressed at the sella floor:
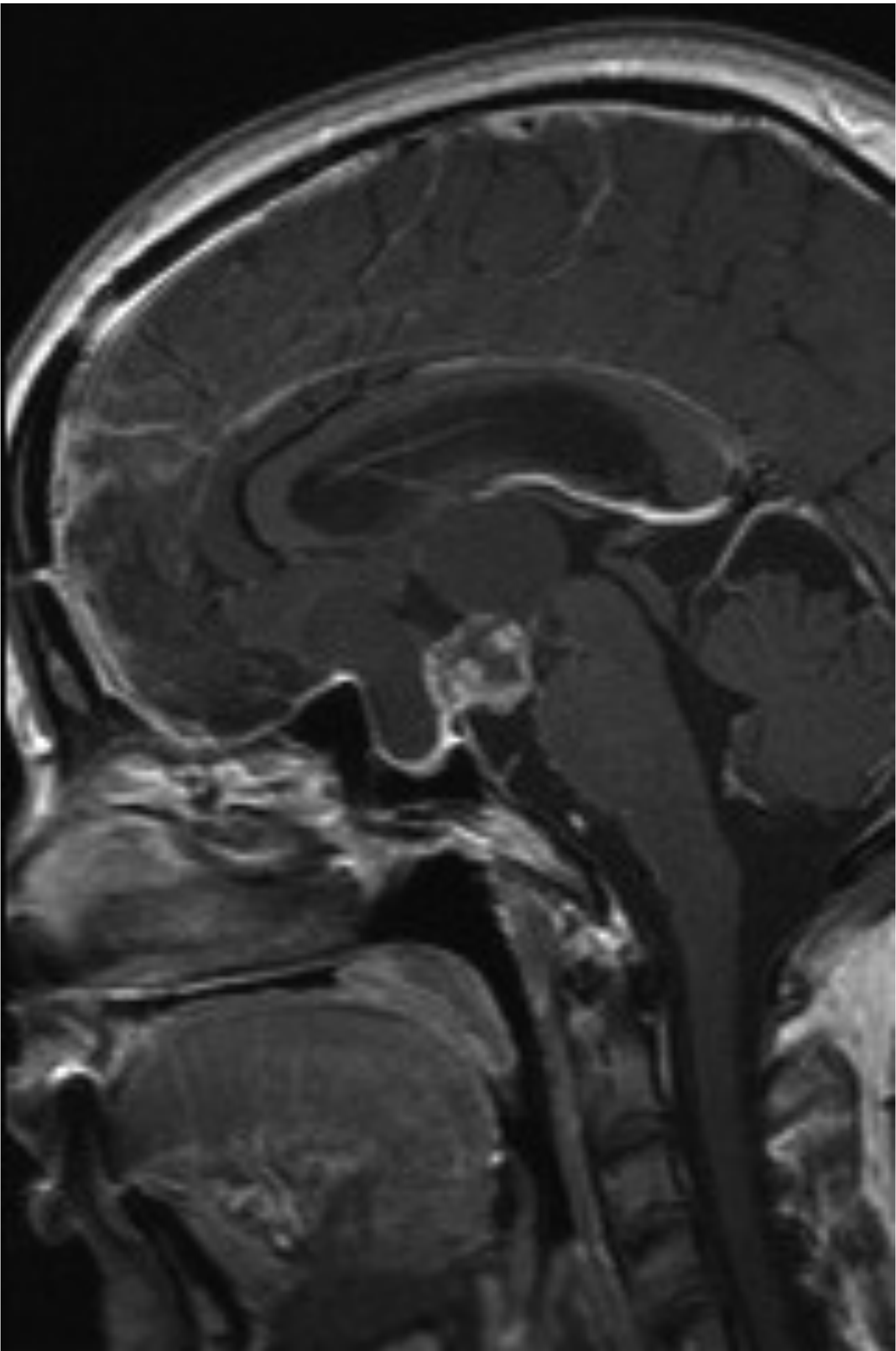
Scott-Brown's Otorhinolaryngology, Fig. 57.8
Classic MRI appearance: multicystic and solid contrast-enhancing suprasellar mass; cystic components bright on T1 pre-contrast. CT is important for identifying intratumoral calcifications (present in ~75% of cases).
Complications
Complications arise both from the tumor itself and from treatment.
Tumor-Related Complications
| System | Complication |
|---|---|
| Visual | Visual field defects (bitemporal hemianopia or complex patterns); compresses chiasm from above/behind, initially damaging upper nasal fibres -> inferotemporal field loss; optic nerve atrophy |
| Endocrine | Panhypopituitarism (GH deficiency in >70% of children at diagnosis; TSH, ACTH, LH/FSH deficits); diabetes insipidus; hyperprolactinemia (stalk compression) |
| Hypothalamic | Severe obesity (damage to satiety centers); thermoregulatory failure; hypodipsia |
| Neurological | Obstructive hydrocephalus (third ventricle encroachment); raised ICP; headache; short-term memory deficits; psychomotor slowing |
| Growth/Development | Dwarfism; delayed sexual maturation; GH deficiency in >70% of pediatric cases |
| Cognitive/Behavioral | Behavioral dysfunction, cognitive impairment, reduced quality of life - particularly in children |
Children at diagnosis commonly present with growth hormone deficiency, obstructive hydrocephalus, short-term memory deficits, and psychomotor slowing. Onset is insidious - a 1-2 year history of slowly progressive symptoms is typical. - Bradley and Daroff's Neurology in Clinical Practice
Post-Treatment Complications
Surgical extirpation commonly worsens pituitary function; often results in:
- Complete panhypopituitarism and diabetes insipidus
- Severe hypothalamic obesity (damage to thirst, temperature, and appetite regulatory centers)
- Permanent neuroendocrine deficits requiring lifelong hormone replacement
Radiation-related long-term complications include:
- Cognitive and endocrine deficits
- Optic neuropathy
- Secondary malignancies
- Vascular injury - moyamoya disease
Most long-term survivors experience significant morbidity from panhypopituitarism, cognitive impairment, and obesity, with a potentially shortened life expectancy from these sequelae. - Goldman-Cecil Medicine
Treatment
1. Surgery (Primary Treatment)
Microsurgical resection is the mainstay. Approaches include:
- Transsphenoidal (preferred when hypothalamus is not involved; also for subdiaphragmatic tumors)
- Transcranial (subfrontal or pterional) for larger/suprasellar extension
- Endoscopic endonasal surgery (EES) - increasingly used; can be employed regardless of size/location except purely intraventricular tumors
Key consideration: Hypothalamic-sparing surgery reduces severe obesity without significantly increasing recurrence rates. Radical resection carries high morbidity; the goal is now often maximal safe resection rather than gross total resection at all costs.
Recurrence rates:
- After total resection: ~30%
- After subtotal resection: ~57%
- After subtotal resection + radiation: ~30%
2. Radiation Therapy
- External beam radiotherapy (EBRT): Extends progression-free survival (PFS) after incomplete resection; used as primary treatment for unresectable or recurrent tumors
- Stereotactic radiosurgery (e.g., Gamma Knife): Used for small residual or recurrent disease
- Intracavitary irradiation: ³²P or ⁹⁰Y instilled into cystic components after stereotactic aspiration; suitable for purely cystic or mixed tumors
3. Intracystic Therapy (for Cystic Craniopharyngioma)
For solitary cystic tumors, stereotactic aspiration followed by instillation of:
- Bleomycin (sclerosing agent) - risk of severe neurotoxicity if the cyst wall leaks into CSF
- Interferon-alpha - subcutaneous (short-acting or pegylated) or intracystic injection; shows promising results in delaying need for radiotherapy
- ³²P or ⁹⁰Y (radioactive colloids)
4. Targeted (Molecular) Therapy
A major recent advance:
- Papillary subtype (BRAF V600E): BRAF inhibitors (vemurafenib/dabrafenib) + MEK inhibitors have shown success in case reports and small series. A Phase II trial of combined MEK/BRAF inhibition is ongoing.
- Adamantinomatous subtype (CTNNB1/beta-catenin): Drugs targeting the Wnt/beta-catenin pathway are still under development.
5. Hormone Replacement
Most patients treated with surgery and/or radiation require lifelong hormone replacement covering:
- GH, thyroid hormone, cortisol (ACTH axis), sex steroids, vasopressin (DI)
- Monitoring and treatment of hypothalamic obesity
Prognosis
The most important factors for progression-free survival are extent of resection and postoperative radiation. Quality of survival is a paramount consideration - the challenge is balancing tumor control against the profound morbidity of hypothalamic damage. A 2024 systematic review (PMID 37466685) of global pediatric craniopharyngioma management confirmed that outcomes depend heavily on treatment modality and institutional approach. A 2025 meta-analysis on radiation therapy for childhood-onset craniopharyngioma (PMID 39751704) provides updated evidence on radiotherapy efficacy and toxicity.
Sources: Bradley and Daroff's Neurology in Clinical Practice | Kanski's Clinical Ophthalmology | Goldman-Cecil Medicine | Scott-Brown's Otorhinolaryngology Head & Neck Surgery
Hyponatremia post craniotomy in craniopharynguoma after hypernatremia
Finding Sources
Finding Sources
Searching PubMed
craniopharyngioma triphasic diabetes insipidus hyponatremia postoperative
Reading File
Reading File
Reading Article
PMID: 38761265
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
Reading File
I now have comprehensive information from all key sources. Let me synthesize the full answer.
Post-Craniotomy Hyponatremia After Hypernatremia in Craniopharyngioma
This is the classic triphasic response - one of the most important and dangerous post-operative sodium patterns following pituitary stalk injury during craniopharyngioma surgery.
The Triphasic Response: Pathophysiology
The sequence hypernatremia → hyponatremia occurs because of pituitary stalk transection (complete or partial) during resection. The AVP (vasopressin) neuronal cell bodies reside in the hypothalamic paraventricular and supraoptic nuclei; their axons travel down the stalk to terminate in the posterior pituitary. Stalk injury severs this connection with predictable consequences in three phases:
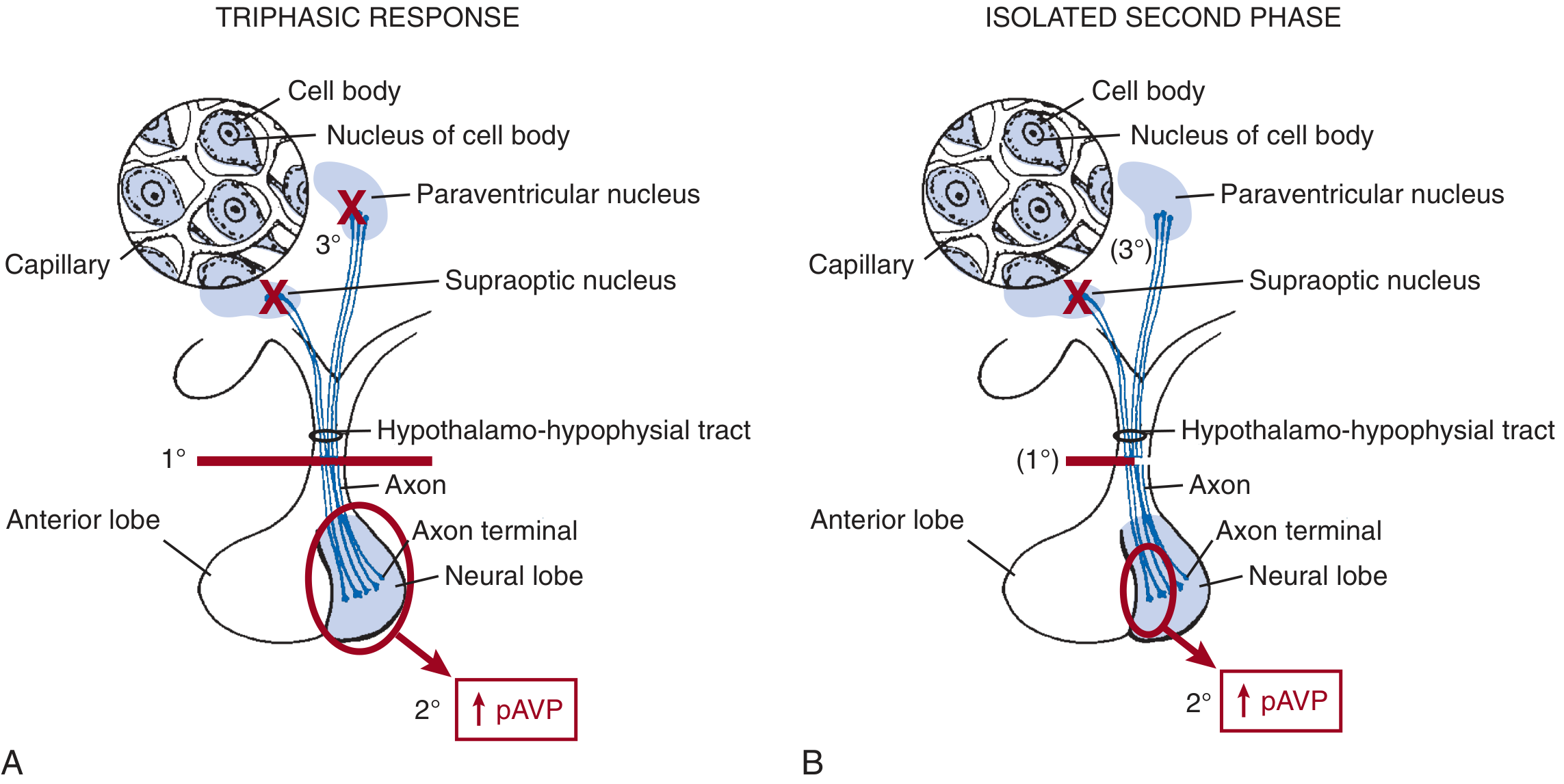
Fig. 15.11, Brenner & Rector's The Kidney: Mechanisms of the triphasic DI response (A) and the isolated second-phase SIADH (B)
Phase 1 - Diabetes Insipidus (Hypernatremia) - Hours to Days
- Mechanism: Axon shock following stalk transection. The severed axons cannot transmit signals from the hypothalamus to the posterior pituitary, so AVP secretion ceases.
- Result: Massive polyuria (hypotonic urine), hypernatremia, hypernatremia, rising serum osmolality.
- Duration: Several hours to a few days.
Phase 2 - SIADH (Hyponatremia) - Days 2 to 14
- Mechanism: The disconnected posterior pituitary gland (and the remaining severed axon terminals) undergoes Wallerian-type degeneration. As the axon terminals die, they dump all stored AVP uncontrollably into the bloodstream. This AVP release is completely autonomous - it is not regulated by osmolality or volume status.
- Result: Concentrated urine, free water retention, dilutional hyponatremia.
- Critical trap: Overly aggressive fluid administration during Phase 1 (to treat DI/hypernatremia) does NOT suppress this uncontrolled AVP release and can worsen the degree of dilutional hyponatremia in Phase 2.
- Duration: 2 to 14 days (until posterior pituitary AVP stores are depleted).
Phase 3 - Return of Permanent DI - After Day 10-14
- Mechanism: Once all stored AVP in the degenerating posterior pituitary is exhausted, DI returns - this time permanently, because >80-90% of the hypothalamic AVP neuronal cell bodies have undergone retrograde degeneration.
- Result: Polyuria resumes, permanent diabetes insipidus requiring lifelong desmopressin.
"Overly aggressive administration of fluids during the second phase does not suppress the uncontrolled vasopressin release from the damaged neurohypophysis and can lead to hyponatremia." - Goldman-Cecil Medicine
Isolated Second Phase (Without Phase 1 DI)
If the stalk is injured but not completely severed, Phase 1 DI may not occur (provided ≥10-20% of stalk fibers remain intact, enough AVP reaches the posterior pituitary to prevent DI). However, the injured terminals still degenerate and dump stored AVP - causing an isolated SIADH phase without preceding DI. This has been documented following transsphenoidal surgery for pituitary microadenomas, typically presenting 5-10 days post-operatively. - Brenner & Rector's The Kidney
Clinical Data in Pediatric Craniopharyngioma
A 2024 French cohort study (PMID 38761265) of 26 children after first craniopharyngioma resection found:
- 65.4% (17/26) had the full triphasic pattern: initial DI followed by hyponatremia days later
- 30.8% (8/26) had isolated persistent DI
- Triphasic response was significantly associated with higher Puget MRI classification (grades 1 and 2, indicating greater hypothalamic involvement)
- Dysnatremia was described as the most common and difficult-to-manage immediate post-operative complication
Differential Diagnosis of Post-Craniotomy Hyponatremia
The hyponatremia in Phase 2 must be distinguished from Cerebral Salt Wasting (CSW) - the distinction is therapeutically critical:
| Feature | Phase 2 SIADH (Triphasic) | Cerebral Salt Wasting (CSW) |
|---|---|---|
| Mechanism | Unregulated AVP dump from degenerating pituitary | Renal Na+ wasting from CNS injury (poorly understood) |
| Volume status | Euvolemic or mildly hypervolemic | Hypovolemic |
| Urine sodium | High | High (not discriminative) |
| Treatment | Fluid restriction | Volume repletion + sodium administration |
| Timing | Days 2-14 post-op (follows DI phase) | Variable, days to weeks |
"SIADH is treated by free-water restriction, whereas cerebral salt wasting is treated with volume repletion and sodium administration... Urine electrolyte analysis is not discriminative, as urine sodium is high in both disorders." - Barash's Clinical Anesthesia
Management of Phase 2 Hyponatremia
During the Transition (Phase 1 → Phase 2)
- Watch for abrupt cessation of polyuria - this signals the onset of Phase 2 AVP release
- Reduce or stop free water and hypotonic fluid administration immediately
- Do not reflexively give more fluids because urine output drops
Treating the Hyponatremia
- Fluid restriction is the mainstay (euvolemic/hypervolemic SIADH)
- Avoid over-correction - correction of hyponatremia must not exceed 8-10 mEq/L per 24 hours to prevent osmotic demyelination syndrome (central pontine myelinolysis), especially if hyponatremia is chronic or symptomatic
- For severe symptomatic hyponatremia (seizures, altered consciousness): hypertonic saline (3% NaCl) can be given cautiously at controlled rates
- Rule out concurrent adrenal insufficiency (common post-craniopharyngioma surgery given panhypopituitarism) - glucocorticoid deficiency independently causes hyponatremia and should be corrected with hydrocortisone
Monitoring
- Serum sodium every 4-6 hours in the acute post-operative phase
- Strict urine output monitoring - the shift from high to low output marks the phase transition
- After Day 14, anticipate return of DI and resume desmopressin
Avoiding the Trap
The most dangerous clinical mistake is continuing aggressive IV fluid replacement (started during Phase 1 DI) into Phase 2. Because AVP release in Phase 2 is autonomous and non-suppressible, all administered free water is retained, driving sodium progressively lower. - Goldman-Cecil Medicine; Brenner & Rector's The Kidney
Summary Timeline
Surgery
|
├── Hours 0–48: Phase 1 - DI → HYPERNATREMIA (polyuria, high serum Na+)
| ↓ Axon shock, no AVP release
|
├── Days 2–14: Phase 2 - SIADH → HYPONATREMIA (oliguria, low serum Na+)
| ↓ Uncontrolled AVP dump from degenerating posterior pituitary
| ↓ *** Fluid restriction; avoid overcorrection ***
|
└── After Day 10–14: Phase 3 - Permanent DI returns
↓ AVP stores exhausted; retrograde neuronal degeneration
↓ Lifelong desmopressin required
Sources: Goldman-Cecil Medicine | Brenner & Rector's The Kidney | Barash's Clinical Anesthesia | Frameworks for Internal Medicine
This is a shared conversation. Sign in to Orris to start your own chat.