Defination of all Krishanagata rogas ( opthal bams )
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching the Web
Krishanagata rogas Ayurveda ophthalmology BAMS definition list
Reading Web Page
https://www.easyayurveda.com/netra-krishnagata-rogas
Searching the Web
Krishnagata rogas 5 types Savrana Shukra Avrana Shukra Sira Shukla definition Ayurveda
Reading Web Page
https://www.easyayurveda.com/netra-krishnagata-rogas
I now have comprehensive information to provide a detailed answer on all Krishnagata Rogas for BAMS ophthalmology (Shalakya Tantra).
Krishnagata Rogas - Definitions (BAMS Ophthalmology / Shalakya Tantra)
What is Krishnagata?
Krishnagata refers to diseases occurring in the Krishna Mandala - the black portion of the eye, which corresponds to the cornea and iris in modern anatomy. Krishna Mandala measures 1/3 of the Netra Budbuda (eyeball). It is predominantly formed from the Vata Mahabhuta (air element).
The cornea and iris together form the Prathama Patala (first layer/tunic) and Dwiteeya Patala (second layer/tunic) of the eye in Ayurvedic anatomy.
Total Number of Krishnagata Rogas
| Authority | Number of Diseases |
|---|---|
| Sushruta (Sushruta Samhita) | 4 diseases |
| Vagbhata (Ashtanga Hridayam) | 5 diseases (adds Siraja Shukra) |
The 4 Krishnagata Rogas (as per Sushruta)
1. Savrana Shukra (Kshata Shukra / Savrana Shukla)
Modern Correlation: Ulcerative Keratitis / Corneal Ulcer / Superficial Punctate Keratitis
Definition:
Savrana Shukra is a disease of the Krishna Mandala (cornea) in which a Vrana (ulcer) appears on the black of the eye. The ulcer appears like a needle puncture - small, pin-point, circular in shape, located deep in the cornea, and is hardly visible to the naked eye.
Etymology: "Sa" = with; "Vrana" = ulcer; "Shukra/Shukla" = white opacity - meaning a white opacity with an ulcer.
Key Features:
- Small, pinpoint circular ulcer on cornea
- Hot (burning) tears (Ushnasrava)
- Severe eye pain
- Inability to see properly
- Nimagna Rupa (sunken appearance of the lesion)
Dosha: Raktaja (caused by vitiated Rakta/blood)
Prognosis: Asadhya (Incurable) - one of the most serious Krishnagata Rogas
Vagbhata's Version - Kshata Shukra: Master Vagbhata named this as Kshata Shukra and described symptoms in layers - symptoms corresponding to first layer of the eye are treatable with difficulty (Kricchrasadhya), while symptoms involving second and third layers are incurable.
2. Avrana Shukra (Avrana Shukla)
Modern Correlation: Corneal Opacity / Leucoma
Definition:
Avrana Shukra is a disease of the cornea in which a thin white covering or opacity forms over the cornea without any ulcer. It appears as a white, smooth, painless opacity on the black of the eye.
Etymology: "A" = without; "Vrana" = ulcer; "Shukra/Shukla" = white - meaning a white opacity WITHOUT an ulcer.
Key Features:
- Thin white opacity/covering on the cornea
- No pain (Nirveda)
- No tearing (Ashrunayana)
- No ulceration - smooth surface
- Diminished vision due to opacity
Dosha: Raktaja (caused by vitiated Rakta/blood)
Prognosis: Sadhya (Curable) - the only one among the 4 Krishnagata Rogas that is curable
Treatment: Aushadha Sadhya (treatable through medicines alone); surgical procedures are contraindicated (Ashastra Krutya Roga). Medicines like Anjana (collyrium), Aschyotana (eye drops), and Seka (washing/irrigation) are used.
Avrana Shukra is considered a sequel or an early/less severe stage compared to Savrana Shukra - if the ulcer heals but leaves a scar, it manifests as Avrana Shukra.
3. Akshipakatyaya (Pakaatyaya)
Modern Correlation: Hypopyon Ulcer / Keratomalacia / Panophthalmitis (advanced stage)
Definition:
Akshipakatyaya is a severe inflammatory disease of the cornea and the entire eye where pus accumulation (Paka) occurs in the anterior chamber and the entire eye undergoes suppurative inflammation. The word "Pakatyaya" means "the disease has crossed (exceeded) the stage of Paka (suppuration)."
Etymology: "Akshi" = eye; "Paka" = suppuration/cooking; "Atyaya" = excessive/beyond limit - meaning excessive suppuration of the eye.
Key Features:
- Severe, intense pain in the eye
- Pus formation in the anterior chamber (Hypopyon)
- Redness and swelling of the entire eye
- Complete loss of vision
- The entire eye is involved (not just cornea)
- Fever and constitutional symptoms may accompany
Dosha: Tridoshaja (caused by simultaneous vitiation of all three Doshas - Vata, Pitta and Kapha)
Prognosis: Asadhya (Incurable) - because it is Tridoshaja and involves the entire eye
Significance in BAMS: This condition is considered the most severe stage of Krishnagata Roga - it represents a progression from untreated Savrana Shukra.
4. Ajakajata (Ajakaajaata)
Modern Correlation: Anterior Staphyloma / Corneal Staphyloma
Definition:
Ajakajata is a disease of the cornea in which the cornea bulges outward like a grape or goat's eye, forming a dark-colored, protruding mass. The diseased cornea protrudes due to weakness and thinning, with the underlying iris/uvea pushing through.
Etymology: "Aja" = goat; "Kaajata" = eye of a goat - because the bulging cornea resembles the eye of a goat (protruding appearance).
Key Features:
- Dark-colored (bluish-black) protrusion of the cornea
- Cornea becomes thin and bulges outward
- Resembles the eye of a goat
- Usually painless in established stage
- Severely impaired or absent vision
- Results from weakened corneal tissue after ulceration
Dosha: Raktaja (caused by vitiated Rakta/blood)
Prognosis: Asadhya (Incurable)
5. Siraja Shukra (Sira Shukla) - Additional disease per Vagbhata
Modern Correlation: Corneal Vascularization / Pannus
Definition:
Siraja Shukra is a disease described by Vagbhata in which blood vessels (Siras) grow into the cornea, causing white opacity with visible blood vessel tracks. This is an additional (5th) Krishnagata Roga mentioned in Ashtanga Hridayam.
Etymology: "Sira" = blood vessel; "Shukra/Shukla" = white - meaning a white opacity associated with blood vessels.
Key Features:
- White opacity on the cornea
- Visible vascular tracks (blood vessels) running into the cornea
- Reduced transparency of the cornea
- Impaired vision
Prognosis: Generally mentioned as a knowledge-based condition (Jnana-vishaya) in BAMS curriculum
Summary Table
| # | Roga | Modern Equivalent | Dosha | Prognosis |
|---|---|---|---|---|
| 1 | Savrana Shukra | Corneal Ulcer / Ulcerative Keratitis | Raktaja | Asadhya (Incurable) |
| 2 | Avrana Shukra | Corneal Opacity / Leucoma | Raktaja | Sadhya (Curable) |
| 3 | Akshipakatyaya | Hypopyon / Panophthalmitis | Tridoshaja | Asadhya (Incurable) |
| 4 | Ajakajata | Anterior Staphyloma | Raktaja | Asadhya (Incurable) |
| 5 | Siraja Shukra | Corneal Vascularization/Pannus | - | Knowledge-level (Vagbhata only) |
Key Points for BAMS Exam
- Total Krishnagata Rogas: 4 (Sushruta) or 5 (Vagbhata)
- Only curable (Sadhya) disease: Avrana Shukra - treated by medicines only (Ashastra Krutya)
- Only Tridoshaja disease: Akshipakatyaya
- The other 3 (Savrana Shukra, Akshipakatyaya, Ajakajata) are Asadhya (incurable)
- Raktaja diseases: Savrana Shukra, Avrana Shukra, Ajakajata (all three caused by vitiated blood)
- Progression sequence: Savrana Shukra → Avrana Shukra → Akshipakatyaya → Ajakajata (stages of worsening corneal disease)
- Krishna Mandala = Cornea + Iris; formed from Vata Mahabhuta
- BAMS Detailed study required: Savrana/Kshata Shukla and Avrana Shukla
- BAMS Brief knowledge required: Sira Shukla, Akshipakatyaya, and Ajakajata
Sources: EasyAyurveda - Netra Krishnagata Rogas, EasyAyurveda - Classification of Eye Diseases, RGUHS BAMS Syllabus, comparative study by Nandam et al., 2019
Classify Corneal Ulcers.Describe etiology, clinical features, management and complications of Bacterial, Viral and Fungal Corneal Ulcers. ( Don't make it too difficult for me haha )
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have all I need. Let me compile the comprehensive, student-friendly answer.
Corneal Ulcers - Classification, Etiology, Features, Management & Complications
What is a Corneal Ulcer?
A corneal ulcer is a loss of continuity of the corneal epithelium with underlying stromal involvement, usually associated with infection or inflammation. It is one of the most important causes of preventable blindness worldwide.
CLASSIFICATION
CORNEAL ULCERS
│
├── A. By Etiology (Most Important!)
│ ├── 1. INFECTIVE
│ │ ├── Bacterial (most common overall)
│ │ ├── Viral (Herpes Simplex - most common in developed countries)
│ │ ├── Fungal (most common in tropical/agricultural regions)
│ │ └── Protozoal (Acanthamoeba - contact lens wearers)
│ │
│ └── 2. NON-INFECTIVE
│ ├── Neurotrophic (loss of corneal sensation)
│ ├── Exposure keratopathy (lagophthalmos, ectropion)
│ ├── Autoimmune (Mooren's ulcer, rheumatoid arthritis)
│ ├── Nutritional (Vitamin A deficiency → xerophthalmia)
│ └── Toxic / chemical
│
├── B. By Location
│ ├── Central
│ └── Peripheral / Marginal
│
├── C. By Depth
│ ├── Superficial (epithelial)
│ ├── Stromal (anterior / middle / deep)
│ └── Descemetocele (Descemet's membrane exposed)
│
└── D. By Prognosis
├── Healing (responding to treatment)
└── Non-healing / Progressive
1. BACTERIAL CORNEAL ULCER
Most common cause of infectious corneal ulcer worldwide.
Etiology (Common Organisms)
| Organism | Key Feature |
|---|---|
| Pseudomonas aeruginosa | #1 in contact lens wearers; >60% of lens-related ulcers; very aggressive |
| Staphylococcus aureus | Common skin/nasal commensal; focal well-defined yellow-white infiltrate |
| Streptococcus pneumoniae | Upper respiratory commensal; often aggressive |
| S. pyogenes | Throat/vaginal commensal; aggressive infections |
| Neisseria gonorrhoeae | Can penetrate HEALTHY epithelium (important exception!) |
| N. meningitidis, H. influenzae, C. diphtheriae | Also can penetrate intact epithelium |
Most bacteria need compromised corneal defences to cause infection. The exceptions above can breach a healthy cornea.
Risk Factors (Predisposing Conditions)
- Contact lens wear - single most important risk factor (especially soft lenses worn overnight, poor hygiene)
- Corneal trauma (including post-LASIK surgery)
- Ocular surface disease (dry eye, blepharitis)
- Systemic immunosuppression, diabetes
- Topical steroid use
- Bullous keratopathy, keratoconus
Clinical Features
Symptoms:
- Sudden onset severe eye pain
- Redness (circumcorneal injection)
- Photophobia
- Watering / discharge (mucopurulent)
- Blurred vision
Signs:
- Epithelial defect + underlying stromal infiltrate (white/yellow-white)
- Stromal oedema and folds in Descemet's membrane
- Anterior uveitis
- Hypopyon (pus in anterior chamber) - seen in moderate-severe cases
- Posterior synechiae
- Chemosis and eyelid swelling in severe cases
- Pseudomonas - can cause very large, rapidly spreading ulcer → descemetocele → perforation
Investigations
- Corneal scraping - gold standard (mandatory for ulcers >2 mm, central, deep stromal, chronic)
- Gram stain - identifies bacteria and fungi
- Culture on blood agar, chocolate agar, Sabouraud agar (incubated at 37°C)
- Brain-Heart Infusion (BHI) broth for enrichment
- Stains used: Gram, Giemsa, Ziehl-Neelsen (for Mycobacterium), Calcofluor white
- Sensitivity testing to guide antibiotic choice
Management
General:
- Stop contact lens wear immediately (mandatory)
- Hospital admission for aggressive disease or poor compliance
- Clear eye shield if significant thinning/perforation risk
Medical Treatment:
- Empirical broad-spectrum topical antibiotics - start before culture results
- Fluoroquinolones (Ciprofloxacin 0.3%, Ofloxacin 0.3%, Moxifloxacin 0.5%) - drug of choice for monotherapy; covers most pathogens
- Fortified antibiotics for severe cases: Fortified Tobramycin (1.3%) + Cefazolin (5%) - dual therapy
- Dosing: Hourly day and night for 24-48 hours, then tapered
- Cycloplegics (Atropine 1%) - for pain relief and to prevent posterior synechiae
- Topical steroids - only after infection is controlled and with caution
Surgical:
- Corneal transplant (Penetrating Keratoplasty) - for perforations or non-healing ulcers
- Tissue glue + bandage contact lens - for small perforations
- Conjunctival flap - for peripheral/chronic non-healing ulcers
Complications
- Corneal perforation - especially Pseudomonas
- Hypopyon (sterile pus in AC)
- Endophthalmitis (rare without perforation)
- Corneal scarring - permanent opacity, irregular astigmatism
- Corneal vascularization
- Descemetocele formation
- Iris prolapse after perforation
- Phthisis bulbi (shrunken, non-functional eye) - end stage
2. VIRAL CORNEAL ULCER (Herpes Simplex Keratitis)
Most common infectious cause of corneal blindness in developed countries. HSV-1 is the usual culprit.
Etiology
- Herpes Simplex Virus type 1 (HSV-1) - causes disease above the waist (face, lips, eyes)
- HSV-2 - genital herpes; rarely involves the eye (neonatal conjunctivitis, sexual transmission)
- Virus resides latent in trigeminal ganglion after primary infection
- Reactivated by: fever, UV light, stress, immunosuppression, menstruation, trauma
- Spread: droplet transmission or direct contact; common in poor hygiene/crowding
Epidemiology: Up to 60% of corneal ulcers in developing countries may be due to HSV; ~10% of HSK patients eventually have vision <6/60.
Types of Herpes Simplex Keratitis
| Type | Layer Involved | Key Feature |
|---|---|---|
| Epithelial (Dendritic) | Epithelium | Branching dendritic ulcer - pathognomonic |
| Disciform (Stromal) | Stroma + endothelium | Disc-shaped stromal oedema - immune-mediated |
| Necrotizing Stromal | Deep stroma | Active viral replication; stromal melting |
| Neurotrophic | Epithelium | Non-healing defect due to corneal anaesthesia |
Clinical Features
Epithelial HSK (Most Common)
Symptoms:
- Foreign body sensation, watering, mild pain
- Reduced corneal sensation (anaesthesia - characteristic!)
- Blurred vision
- History of cold sores / lip blisters common
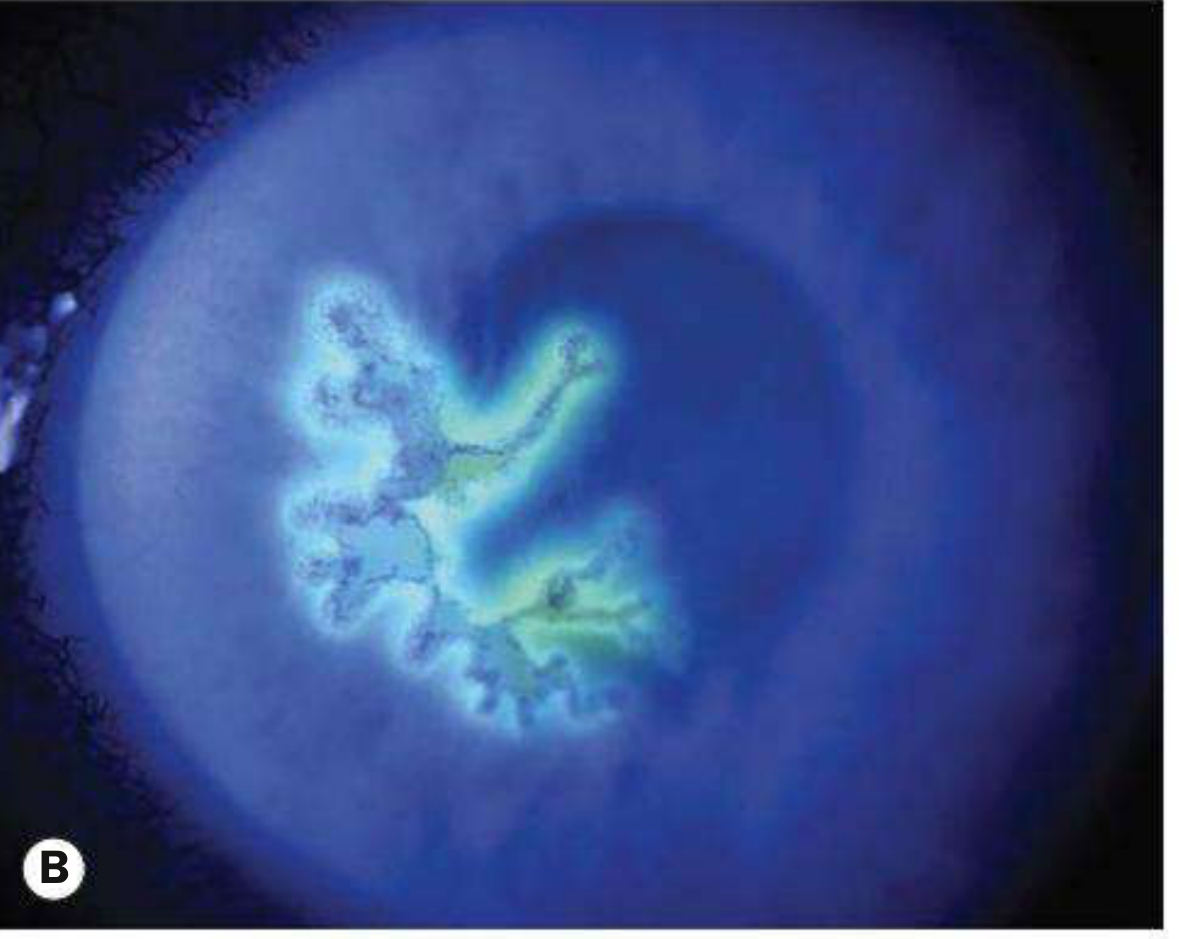
Signs - The Pathognomonic Finding:
- Dendritic ulcer - branching, tree-like (dendrite = branch in Greek) ulcer with terminal bulbs at the ends
- Stains brilliantly with fluorescein (the ulcer bed stains green)
- Stains at margins with rose Bengal (the infected but living cells at edges stain red)
- May enlarge into a geographic ulcer (large, amoeboid shaped)
- Reduced/absent corneal sensation
Disciform (Stromal) HSK
- Central disc-shaped area of stromal oedema - hazy, thickened cornea
- Overlying epithelial oedema (bullae)
- Keratic precipitates (KP) directly under the oedematous area
- Raised IOP common (trabeculitis)
- Mild anterior uveitis
Investigations
- Clinical diagnosis usually (dendritic ulcer is pathognomonic)
- Corneal scraping in viral transport medium → PCR (most sensitive - up to 90%) or culture
- Giemsa stain → multinucleated giant cells
- HSV serology - only rises on primary infection
- Immunocytochemistry available
Management
Epithelial HSK:
- Topical antivirals:
- Aciclovir 3% eye ointment - 5 times daily for 14 days (first choice)
- Ganciclovir 0.15% gel - 5 times daily
- Trifluridine (vidarabine) - alternatives
- Oral antivirals - for immunocompromised, children, severe disease:
- Aciclovir 200-400 mg 5 times daily for 5-10 days
- Famciclovir or Valaciclovir (better tolerated, less frequent dosing)
- Debridement - wiping the corneal surface with a sterile swab, 2 mm beyond ulcer edge; removes virus-laden cells
- Cycloplegics (Homatropine 1%) for comfort
- Topical antibiotic prophylaxis (some practitioners)
⚠️ IMPORTANT RULE: NEVER use topical steroids in epithelial HSK - this dramatically worsens the ulceration and can cause corneal perforation!
Disciform HSK:
- Topical steroids (prednisolone) + topical antivirals together (steroids alone would allow viral replication)
- Long-term oral aciclovir 400 mg twice daily - prophylaxis to prevent recurrences (HEDS trial)
Recurrence prevention:
- Long-term oral aciclovir significantly reduces recurrence rate
Complications
- Corneal scarring - gets worse with each recurrence
- Corneal vascularization and lipid deposition
- Corneal anaesthesia (neurotrophic keratopathy)
- Irregular astigmatism
- Glaucoma (secondary, from trabeculitis or steroid use)
- Cataract (from chronic inflammation or steroids)
- Corneal perforation - in necrotizing form
- Amblyopia in children
- Final visual acuity <6/60 in ~10% of patients
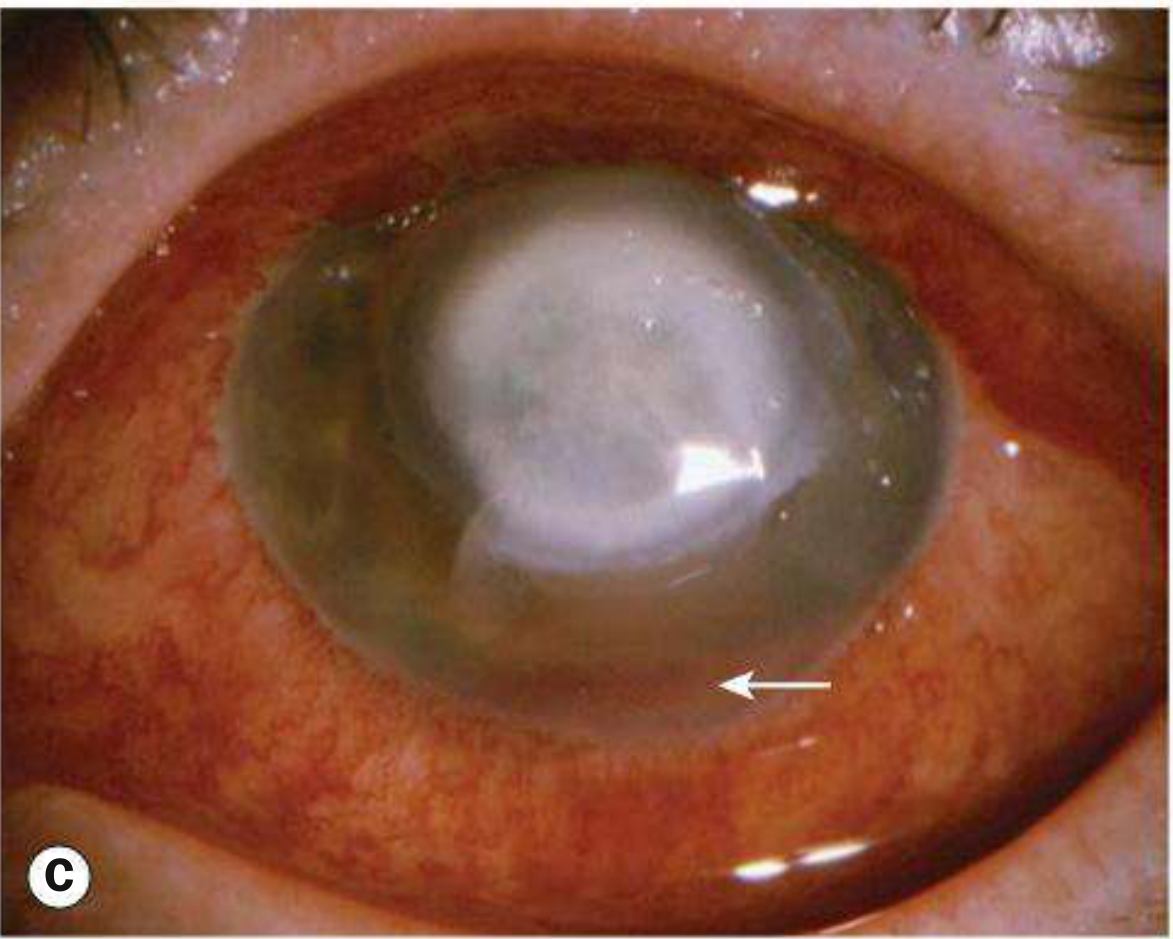
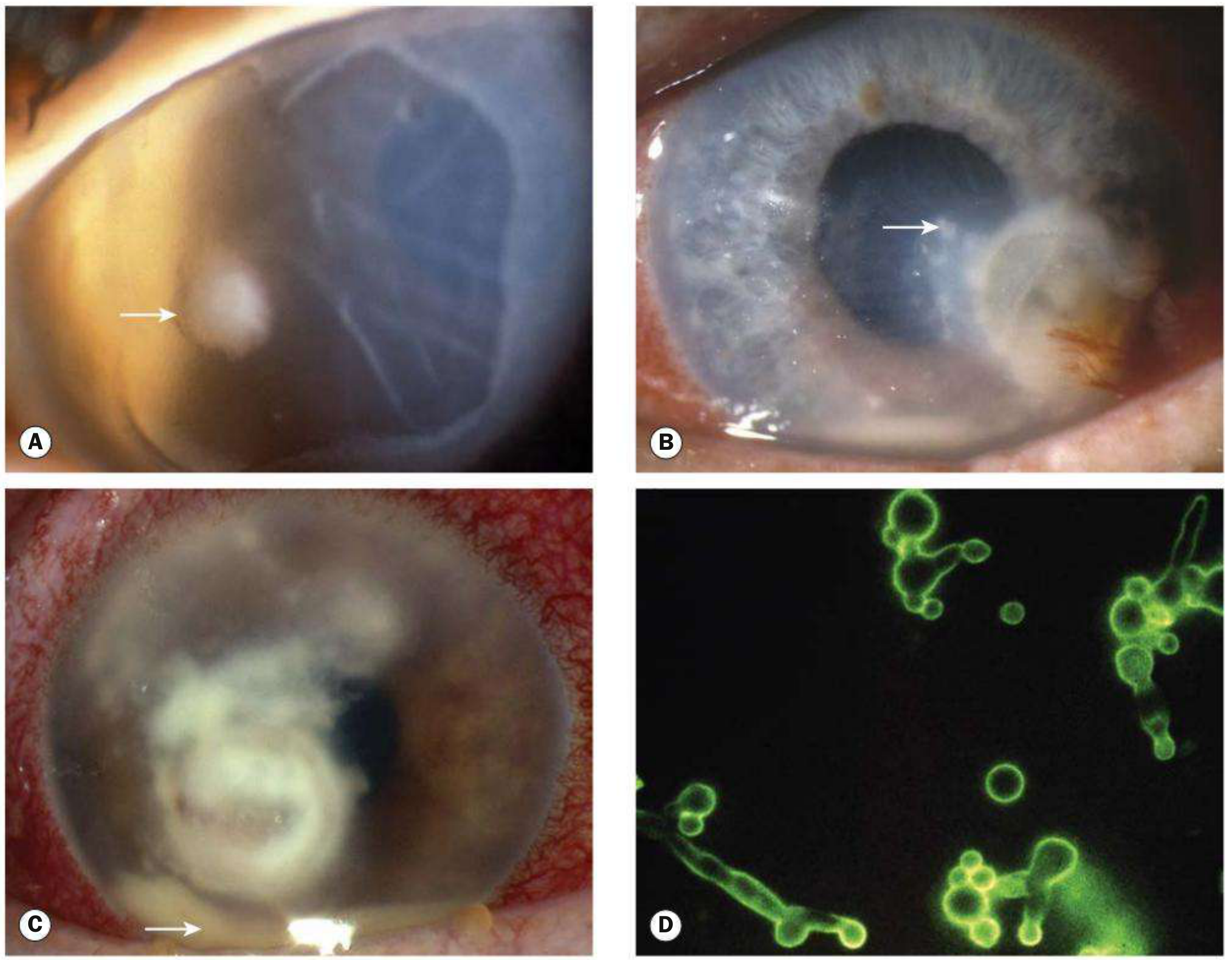
3. FUNGAL CORNEAL ULCER (Fungal Keratitis / Keratomycosis)
The most common cause of corneal blindness in tropical and low-income countries. Often misdiagnosed as bacterial initially!
Etiology
| Type | Organisms | Climate |
|---|---|---|
| Filamentous (moulds) | Fusarium spp., Aspergillus spp. | Tropical (most common there) |
| Yeasts | Candida spp. | Temperate climates |
- Filamentous fungi: multicellular, form hyphae (tube-like projections); aggressive course
- Candida: ovoid, unicellular, reproduce by budding
Risk Factors (Predisposing Conditions)
- Trauma with plant material / agricultural tools - classic history for filamentous fungi (farmer scratched by paddy/thorn)
- Topical corticosteroid use - very important (suppresses immunity, allows fungi to proliferate)
- Chronic ocular surface disease
- Contact lens wear
- Previous corneal transplant
- Systemic immunosuppression, diabetes
Clinical Features
Key point: Diagnosis is often delayed because it looks like bacterial keratitis initially! Have a high index of suspicion, especially with history of plant trauma + steroid use + rural/tropical setting.
Symptoms:
- Gradual onset of pain (slower than bacterial)
- Grittiness, photophobia
- Blurred vision
- Watery or mucopurulent discharge
Signs:
Candida keratitis:
- Yellow-white, densely suppurative infiltrate (looks like bacterial)
Filamentous keratitis (more distinctive):
- Grey or yellow-white stromal infiltrate with indistinct, fluffy (feathery) margins - very characteristic!
- Satellite lesions (separate smaller infiltrates around the main one) - hallmark sign
- Feathery/branch-like extensions of infiltrate
- Ring-shaped infiltrate
- Rapid progression with necrosis and corneal thinning
- Epithelial defect may be small or absent initially
- Anterior uveitis, hypopyon, endothelial plaque, raised IOP
- Fungi can penetrate intact Descemet membrane → endophthalmitis without obvious perforation (unique to fungi!)
Investigations
- Corneal scraping - must be taken before starting treatment
- KOH (Potassium Hydroxide) preparation - rapid, highly sensitive; shows fungal elements under microscope
- Gram and Giemsa stain - ~50% sensitive for fungi
- Calcofluor white (fluorescent stain) - excellent for fungi and Acanthamoeba
- Periodic Acid-Schiff (PAS), Methenamine silver stains
- Culture on Sabouraud Dextrose Agar (specific for fungi; also grows on blood agar)
- PCR - up to 90% sensitive; investigation of choice in many centres
- Corneal biopsy - if no growth after 1 week of scraping and no improvement after 3-4 days of treatment (fungi proliferate just anterior to Descemet's - deep biopsy may be needed)
- Confocal microscopy - can identify organisms in vivo; not widely available
Management
General:
- Hospital admission usually required
- Stop topical steroids (CRITICAL - they will make it much worse)
- Remove epithelium over the lesion to enhance antifungal penetration
- Regularly remove mucus and necrotic tissue with a spatula
- Improvement is much slower than bacterial - patient and doctor need patience
Topical Antifungals (given hourly initially for 48 hours, then tapered):
| Organism | Drug of Choice | Alternatives |
|---|---|---|
| Candida | Amphotericin B 0.15% | Econazole 1%, Natamycin 5%, Fluconazole 2%, Clotrimazole 1%, Voriconazole |
| Filamentous | Natamycin 5% (best for filamentous, especially Fusarium) | Voriconazole 1%, Econazole 1%, Amphotericin B |
Systemic Antifungals:
- Oral voriconazole or itraconazole for severe/deep cases
- IV amphotericin B - for severe systemic spread
Surgical:
- Penetrating Keratoplasty (PKP) - for non-responding or perforated cases
- Anterior chamber washout for hypopyon
- Evisceration - in end-stage, blinded, painful eye
Complications
- Corneal perforation - very common in fungal keratitis
- Endophthalmitis - can occur even without perforation (unique feature - fungi penetrate Descemet's)
- Severe corneal scarring and opacity
- Secondary glaucoma
- Loss of eye (evisceration/enucleation) - poor prognosis overall
Quick Comparison Table - The Cheat Sheet!
| Feature | Bacterial | Viral (HSK) | Fungal |
|---|---|---|---|
| Onset | Acute / rapid | Acute (epithelial) | Gradual / insidious |
| Pain | Severe | Mild-moderate | Moderate (gradual) |
| Classic Appearance | White/yellow dense infiltrate | Dendritic ulcer (branching) | Fluffy margins + satellite lesions |
| Pathognomonic sign | Hypopyon | Dendrite with terminal bulbs | Satellite lesions + feathery edges |
| Corneal sensation | Normal | REDUCED / absent | Normal (initially) |
| Common setting | Contact lens wearer | Stress, fever, immunocompromised | Farmer, plant trauma, steroid user |
| Key stain/test | Gram stain, culture | Fluorescein (dendrite), PCR | KOH prep, Calcofluor white |
| Treatment | Fluoroquinolone drops | Aciclovir (NEVER steroids alone) | Natamycin / Amphotericin B |
| Steroids | Cautious use after infection controlled | CONTRAINDICATED in epithelial | CONTRAINDICATED (makes it worse) |
| Prognosis | Good if treated early | Recurrent; can scar over time | Often poor; perforation common |
One-Line Memory Tricks
- Bacterial = Contact lens + Quick onset + Dense white infiltrate + Gram stain
- Viral (HSK) = Dendrite + Terminal bulbs + Reduced sensation + NEVER steroids alone
- Fungal = Farmer + Plant trauma + Fluffy/feathery + Satellites + KOH prep + NEVER steroids
Sources: Kanski's Clinical Ophthalmology, 10th ed., Ch. 7 - Cornea and Sclera
This is a shared conversation. Sign in to Orris to start your own chat.