Describe clinical features, screening policy and treatment of familial adenomatous polyposis. [3
Reading File
Finding Sources
Searching PubMed
"familial adenomatous polyposis" AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed for a comprehensive answer. Here is the full structured response:
Familial Adenomatous Polyposis (FAP)
Genetics and Pathogenesis
FAP is an autosomal dominant disorder caused by a germline mutation in the APC (adenomatous polyposis coli) tumor suppressor gene on chromosome 5q21-22. APC is a key negative regulator of the Wnt signaling pathway. The mutated allele is inherited from the affected parent; adenomas develop when the second (normal) allele is lost or mutated (two-hit hypothesis).
- Prevalence: 1 in 5,000-7,500
- ~75% of cases are familial; ~25-30% arise from de novo mutations
- Most mutations lie between codons 168 and 1640; hotspots at codons 1061 and 1309
Clinical Features
Colorectal (Classic FAP)
- Hundreds to thousands of colorectal adenomas (by definition >100; often thousands) developing in adolescence
- Present in up to 15% by age 10 and 75% by age 20
- Polyps are predominantly in the rectum and left colon
- Morphologically identical to sporadic adenomas (tubular, villous); flat/depressed adenomas and microscopic adenomas (1-2 dysplastic crypts) also occur
- Symptoms: rectal bleeding, diarrhea, abdominal pain, mucous discharge
- Without treatment: 100% risk of colorectal carcinoma, often before age 30, and nearly always by age 50
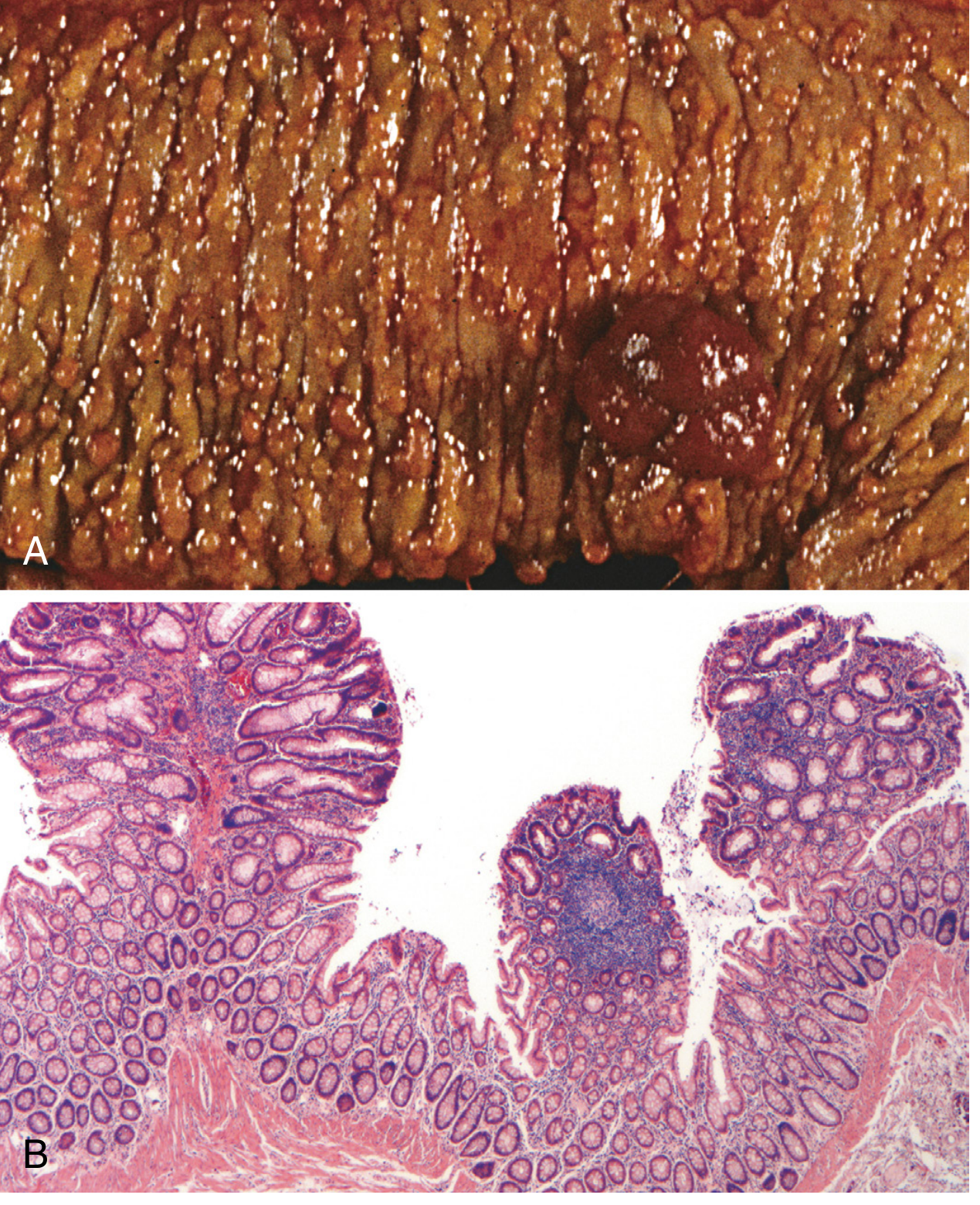
Fig. 17.51 - Familial adenomatous polyposis: (A) gross specimen showing carpet of polyps; (B) histology showing multiple tubular adenomas. - Robbins, Cotran & Kumar Pathologic Basis of Disease
Extracolonic Intestinal Manifestations
| Site | Feature | Details |
|---|---|---|
| Stomach | Fundic gland polyps (FGPs) | 30-90% of patients; low malignant potential; 3rd-4th decade |
| Stomach | Gastric adenomas | 10-30%; malignant potential; mostly antral; higher risk in Japanese/Korean populations |
| Duodenum | Duodenal adenomas | >95% of patients; around ampulla of Vater; develop ~15 years after colonic polyps |
| Duodenum | Duodenal/periampullary cancer | 5-10%; second leading cause of death in FAP; ~age 50 |
Extraintestinal (Extra-GI) Manifestations
- Congenital hypertrophy of retinal pigment epithelium (CHRPE) - present at birth; useful early screening marker (75%)
- Osteomas - mandible, skull, long bones (80%)
- Desmoid tumors - fibromatosis, particularly mesenteric; can be life-threatening
- Epidermoid and sebaceous cysts
- Thyroid tumors (papillary carcinoma)
- Adrenal tumors
- Medulloblastoma (when combined with colonic polyposis = Turcot syndrome)
- Gardner syndrome - FAP + osteomas + soft tissue tumors (epidermal cysts, desmoids) - caused by specific APC mutations
Attenuated FAP (AFAP)
A milder variant caused by mutations in the 5' and 3' regions of APC, with <100 adenomas (often 10-99), predominant proximal colon involvement, and later cancer onset (average 50s vs. 30s in classic FAP).
Screening Policy
For At-Risk Family Members / Known APC Mutation Carriers
| Organ | Modality | Age to Start | Interval |
|---|---|---|---|
| Colorectum | Flexible sigmoidoscopy or colonoscopy | 10-12 years of age | Annually |
| Upper GI (duodenum/stomach) | Upper endoscopy (EGD) | ~20 years of age | Determined by Spigelman score |
| Thyroid | Annual ultrasound | Late teens | Annually |
| Desmoid | Abdominal CT/MRI | If symptomatic or post-surgery | As needed |
Key points:
- Because polyps preferentially involve the left colon and rectum, annual flexible proctosigmoidoscopy is acceptable as an alternative to full colonoscopy; if adenomas are found, proceed to full colonoscopy
- Genetic testing (APC mutation analysis) should be offered to at-risk family members; a mutation is identifiable in ~75% of families
- CHRPE (detected on ophthalmologic exam at birth) can be an early adjunct to screening before endoscopy is warranted
- Spigelman severity staging (I-IV) for duodenal adenomas determines surveillance intervals: Stage I = no cancer risk at 10 years; Stages II-III = 2% risk; Stage IV = 36% risk → closer surveillance or prophylactic surgery
Treatment
Colorectal Surgery (Mandatory - Prophylactic)
Prophylactic colectomy is the standard of care and is generally recommended within 10 years of disease onset (typically late teens to early 20s). Three surgical options:
| Procedure | Details | Advantage / Disadvantage |
|---|---|---|
| Panproctocolectomy + permanent ileostomy | Entire colon and rectum removed | Eliminates all rectal risk; permanent stoma |
| Colectomy + ileorectal anastomosis (IRA) | Colon removed; rectum preserved | Avoids stoma; requires annual rectal surveillance; suitable only if rectal polyp load is low |
| Restorative proctocolectomy + ileal pouch-anal anastomosis (IPAA) | Colon and rectum removed; J-pouch formed | No stoma; restores continence; remaining pouch requires surveillance for pouch neoplasia |
The choice depends on the rectal polyp burden, APC mutation location, and patient preference.
Upper GI Management
- Small tubular adenomas / low-grade dysplasia at ampulla: biopsy and observe
- High-risk adenomas (villous, >1 cm, high-grade dysplasia, or Spigelman stage IV): endoscopic resection or surgical duodenectomy/pancreaticoduodenectomy
Desmoid Tumors
- Non-resectable or mesenteric desmoids: sulindac, anti-estrogens (tamoxifen), or tyrosine kinase inhibitors (imatinib, sorafenib) in refractory cases
Chemoprevention
- Sulindac (NSAID) and celecoxib (COX-2 inhibitor) reduce polyp number and size but do not eliminate the need for surgery and are not substitutes for prophylactic colectomy
- Celecoxib is FDA-approved as an adjunct (not primary) treatment for FAP
Surveillance After Surgery
- After IRA: annual flexible sigmoidoscopy of the rectal remnant
- After IPAA: regular pouch endoscopy (recent 2024 systematic review PMID 37878460 highlights importance of pouch surveillance for neoplasia in FAP)
- Upper GI endoscopy continues lifelong per Spigelman staging
Summary Table: FAP vs. Attenuated FAP
| Feature | Classic FAP | Attenuated FAP |
|---|---|---|
| Polyp number | >100 (hundreds-thousands) | <100 (10-99) |
| Location | Left colon + rectum | Proximal colon |
| Age of cancer | 30-40 if untreated | 50s |
| APC mutation site | Codons 168-1640 | 5' and 3' ends of gene |
Sources: - Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 756-757 | - Current Surgical Therapy 14e, p. 287 | - Sleisenger and Fordtran's GI and Liver Disease, p. 2578 | - Bailey and Love's Short Practice of Surgery 28th ed., p. 1424
Recent Evidence Note: Updated European guidelines (EHTG-ESCP 2024, PMID 38722804) and a 2024 systematic review on FAP pouch neoplasia surveillance (PMID 37878460) are broadly consistent with the above management framework, with emphasis on individualized surgical approach and lifelong upper GI and pouch surveillance.
This is a shared conversation. Sign in to Orris to start your own chat.