Ventilator modes and uses with statergy in various diseases full details for knowledge with proper approach
Reading File
Finding Sources
Finding Sources
Searching PubMed
"mechanical ventilation" AND "modes" AND "ARDS"
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a fully detailed, textbook-referenced guide to ventilator modes and disease-specific strategies:
Mechanical Ventilation: Modes, Settings, and Disease Strategies
1. Foundational Concepts
What Does "Mode" Mean?
A ventilator mode describes the relationship among breath types (mandatory, assisted, supported, and spontaneous) and the inspiratory phase control variables (volume-targeted vs. pressure-targeted). Every mode is defined by three variables:
- Trigger - what starts inspiration (patient effort [flow/pressure] or time)
- Limit - what controls the shape of inspiration (pressure or flow)
- Cycle - what ends inspiration (volume, time, or flow threshold)
Breath Types
| Breath Type | Trigger | Limit | Cycle |
|---|---|---|---|
| Controlled (mandatory) | Time | Flow or pressure | Volume or time |
| Assisted | Patient effort | Flow or pressure | Volume or time |
| Pressure supported | Patient effort | Pressure | Flow threshold |
| Spontaneous (CPAP) | Patient effort | None | Patient effort |
2. Core Ventilator Modes in Detail
A. Controlled Mechanical Ventilation (CMV)
Mechanism: The ventilator delivers all breaths at a preset rate. The patient cannot trigger additional breaths. Used in apneic patients (brain damage, deep sedation, or paralysis).
- Volume-controlled CMV (VCV): Fixed preset tidal volume (Vt); flow is constant (square wave); airway pressure varies with compliance.
- Pressure-controlled CMV (PCV): Fixed inspiratory pressure and time; Vt varies with lung compliance/resistance.
Use: Reserved for patients with no respiratory drive. Rarely used independently outside of the OR.
B. Assist-Control Ventilation (ACV) - The Most Common ICU Mode
Mechanism: The ventilator delivers a breath when triggered by the patient's effort OR, if no effort occurs within the preset cycle time, time-triggers a backup breath. Every breath is fully supported - there are no unsupported spontaneous breaths.
- Volume Assist-Control (VACV): Volume-targeted, flow-cycled. Vt is guaranteed with each breath. Airway pressure varies. The greater the patient's inspiratory effort, the lower the airway pressure seen on the monitor. Patient performs approximately one-third of the work of a passive breath even when settings are correct.
- Pressure Assist-Control (PACV): Pressure-targeted, time-cycled. Pressure is guaranteed; Vt varies. Initial flow is rapid (decelerating waveform), which may improve patient synchrony and gas distribution.
Key Points:
- Machine inspiratory time (T
i) may be shorter or longer than the patient's neural Ti, producing dyssynchrony (premature cycling or delayed cycling). - If set backup rate is much lower than the patient's spontaneous rate, an inverse I:E ratio can develop.
- Risk of double triggering: if Vt is set very low, mechanical T
ibecomes shorter than neural Ti; the patient triggers a second breath immediately after cycling, effectively doubling the Vt delivered.
Murray & Nadel's Textbook of Respiratory Medicine, p. 3175; Fishman's Pulmonary Diseases, p. 2607
C. Pressure Support Ventilation (PSV) - The Most Widely Used Mode Overall
Mechanism: All breaths are patient-triggered. Once triggered, the ventilator delivers flow to meet a set inspiratory pressure. The ventilator cycles off when inspiratory flow falls to a threshold (typically 10-35% of peak flow, adjustable). This flow-cycling allows the patient to control inspiratory duration and synchronizes with neural Ti.
Settings:
- PS level: Typically 5-20 cm H2O above PEEP; titrate to achieve Vt ~6-8 mL/kg
- Cycling criterion: Adjust to match end of patient effort (avoid premature cycling = under-assistance; avoid delayed cycling = over-assistance)
Advantages:
- Best patient-ventilator synchrony (patient controls rate, Vt, and inspiratory time)
- Reduced sedation requirements
- Preferred mode for weaning
Risk: In patients with obstructive disease (COPD), flow may never return to the cycling threshold during inspiration because high airway resistance keeps flow elevated; this causes delayed cycling and expiratory muscle recruitment during mechanical inspiration.
Murray & Nadel's, p. 3175; Fishman's, p. 2607 (Fig. 147-5)
D. Synchronized Intermittent Mandatory Ventilation (SIMV)
Mechanism: Delivers a guaranteed number of positive-pressure breaths per minute (volume or pressure targeted), synchronized with the patient's effort. Between mandatory breaths, the patient can breathe spontaneously (unassisted or with PS).
Key Problem: The respiratory center does not adjust its output breath-to-breath; inspiratory effort and tension-time index are nearly equivalent for both spontaneous and assisted (mandatory) breaths during SIMV. Even at rates of 14 breaths/min, the tension-time index for both breath types exceeds the threshold for respiratory muscle fatigue. This means SIMV may cause or perpetuate muscle fatigue rather than progressive muscle conditioning.
Current Status: SIMV has largely fallen out of favor - evidence shows it delays liberation from mechanical ventilation compared to ACV or PSV weaning. Now mainly used as a historical reference or in specific protocols.
Fishman's Pulmonary Diseases, p. 2694; Murray & Nadel's, p. 3175
E. Pressure-Regulated Volume Control (PRVC) / Adaptive Pressure Ventilation
Mechanism: A hybrid mode combining pressure-targeted breaths (decelerating flow, better synchrony) with volume guarantee as a feedback signal. The ventilator automatically adjusts the inspiratory pressure target breath-to-breath to achieve the set Vt.
Behavior:
- If respiratory mechanics improve (↑ compliance) → pressure target automatically decreases
- If mechanics worsen → pressure target increases
- If patient increases spontaneous effort → pressure target decreases (can lead to under-support during recovery)
Volume Support (VS): Same principle applied to PSV - patient-triggered, flow-cycled, but with automatic pressure adjustment to hit Vt target.
Caution: If the patient is actively breathing with high effort, the ventilator may lower pressure delivery, resulting in inadequate unloading of the respiratory muscles.
F. Adaptive Support Ventilation (ASV)
Mechanism: An assist-control, pressure-targeted, time-cycled mode that uses continuous measurements of respiratory mechanics (compliance, resistance, auto-PEEP) to automatically set the Vt-frequency pattern based on the minimum work of breathing (Otis equation). The clinician sets only desired minute ventilation (as % of predicted normal) and patient height.
Use: Increasingly used in post-cardiac surgery patients; may shorten weaning time in selected patients.
G. CPAP (Continuous Positive Airway Pressure)
Mechanism: Application of a constant positive pressure at the airway opening during entirely spontaneous breathing. The ventilator provides no inspiratory assistance. The patient performs all the work of breathing.
Physiologic Effects:
- Increases FRC by recruiting atelectatic regions
- Reduces intrapulmonary shunt and improves oxygenation
- Improves lung compliance
- Counters intrinsic PEEP (auto-PEEP) in obstructive disease - reduces inspiratory triggering effort
- Reduces LV afterload by lowering LV transmural pressure (useful in cardiogenic pulmonary edema)
Clinical Use:
- OSA (primary indication)
- Cardiogenic pulmonary edema (dramatic benefit)
- Mild hypoxemic respiratory failure (bridge before intubation)
- Weaning: PS 5 cm H2O + PEEP 5 cm H2O ("minimal support" spontaneous breathing trial)
Murray & Nadel's, p. 3195
H. BiPAP / BPAP (Bilevel Positive Airway Pressure)
Mechanism: Pressure cycles between two levels:
- IPAP (inspiratory positive airway pressure) - higher pressure during inspiration = inspiratory assistance
- EPAP (expiratory positive airway pressure) - lower pressure during expiration = PEEP
In its most common form, BPAP = PSV + PEEP delivered noninvasively.
Key Considerations for NIV Delivery:
- Leaks are the primary cause of dyssynchrony: inspiratory leaks → flow never reaches cycling threshold → prolonged inspiration; expiratory leaks → auto-triggering
- Modern "NIV mode" ventilators and dedicated NIV machines have leak-compensation algorithms
- Pressures are set lower than invasive MV to avoid mask leak
- Neurally Adjusted Ventilatory Assist (NAVA) during NIV is unaffected by leaks (trigger = diaphragm EMG)
Strong Recommendation: BPAP for COPD exacerbations with respiratory acidosis (reduces intubation rate, mortality, ICU stay - Level A evidence).
Murray & Nadel's, p. 3195
I. Airway Pressure Release Ventilation (APRV)
Mechanism: A biphasic pressure mode where the patient spends most of the respiratory cycle at a high CPAP level (Phigh) that promotes alveolar recruitment, with brief, periodic releases to a low pressure (Plow) for CO2 elimination. Spontaneous breathing is allowed at any time throughout the cycle.
Settings:
- P
high: 20-30 cm H2O (the sustained pressure for recruitment) - P
low: 0-5 cm H2O (release pressure) - T
high: 4-6 seconds (long - >80% of cycle) - T
low: 0.4-0.8 seconds (short - prevents full exhalation and alveolar derecruitment)
Proposed Benefits:
- Alveolar recruitment maintained throughout cycle
- Allows unrestricted spontaneous breathing (potentially less sedation)
- One small RCT (n=138, China) showed more ventilator-free days, shorter ICU stay vs. lung-protective ventilation
Limitations: No large multicenter RCT confirms superiority over ARDSNet strategy. Routine use in ARDS cannot be recommended until such data exist.
Fishman's Pulmonary Diseases, p. 2505
J. Inverse Ratio Ventilation (IRV)
Mechanism: I:E ratio is set >1:1 (typically 2:1 or 3:1 via PCV). Prolonging inspiratory time increases mean airway pressure without raising peak pressure, potentially improving oxygenation in ARDS.
Problem: Limited expiratory time → dynamic hyperinflation and auto-PEEP. This auto-PEEP + applied PEEP may be non-lung-protective and compromise cardiac output.
Current Status: Considered a salvage strategy only, not routine use. Should not be used to circumvent the ARDS Network low-Vt approach.
K. High-Frequency Oscillatory Ventilation (HFOV)
Mechanism: Rapid oscillations (3-15 Hz) generating very small Vt (<3 mL/kg) around a sustained mean airway pressure (MAP). Both inspiration and active expiration are generated. Theoretically the "ultimate" lung-protective mode.
Evidence in ARDS:
- OSCAR Trial: No mortality benefit vs. usual care
- OSCILLATE Trial: Stopped early - HFOV arm had higher in-hospital mortality (likely due to required high sedation, deep paralysis, and hemodynamic compromise)
Current Status: HFOV is not recommended for routine ARDS management in adults. May still have a role in severe refractory pediatric respiratory failure.
L. NAVA (Neurally Adjusted Ventilatory Assist)
Mechanism: Trigger, limit, and cycle are all controlled by the electrical activity of the diaphragm (EAdi), detected via esophageal electrode catheter. The ventilator delivers proportional assistance that tracks the patient's neural drive in real time.
Advantages:
- Near-elimination of patient-ventilator dyssynchrony (wasted efforts, delayed cycling)
- Not affected by circuit leaks (ideal for NIV)
- No auto-triggering from secretions/circuit
Limitations: Requires specialized electrode catheter; not yet proven to reduce mortality; limited availability.
3. Key Ventilator Settings - The Physiologic Approach
Tidal Volume (Vt)
- Standard patients (no ARDS, normal compliance): 7-8 mL/kg predicted body weight (PBW)
- ARDS: 6 mL/kg PBW, reduce to 4-5 mL/kg if plateau pressure >30 cm H2O
- Critical rule: Target plateau pressure <28-30 cm H2O. Vt of 6 mL/kg has been proven superior only when plateau pressure was >32 cm H2O in ARDSNet trials. In patients with plateau pressure in the low 20s (most ventilated patients), forcing 6 mL/kg is not evidence-based and causes double triggering.
Respiratory Rate (RR)
- ACV: Set close to the patient's spontaneous rate to avoid large discrepancy (which creates inverse I:E)
- ARDS: 6-35 breaths/min, adjusted to achieve pH ≥7.30
- Large rate-Vt discrepancy creates inverse I:E by fixing mechanical T
iwhile total cycle time shortens
PEEP
- Prevents alveolar collapse at end expiration
- ARDS: Use FiO2/PEEP ladder (see table in ARDSNet protocol below)
- COPD: Start at 5 cm H2O; may increase to 50-80% of total auto-PEEP to reduce inspiratory trigger effort
I:E Ratio
- Normal: 1:2 to 1:3
- ARDS: 1:1 to 1:3 (per ARDSNet)
- COPD/Asthma: As long as possible expiratory time (1:3 to 1:5) to allow full exhalation and reduce auto-PEEP
FiO2
- Target SpO2 88-95% (ARDS) or >92% (most others); avoid 100% O2 for prolonged periods (absorption atelectasis, oxygen toxicity)
- Start 0.8 if infiltrates present; 0.4 if COPD/asthma/PE (no infiltrates)
Trigger Sensitivity
- Set at -1 to -2 cm H2O (pressure trigger) or 1-3 L/min (flow trigger) - sensitive enough to avoid wasted efforts but not so sensitive as to allow auto-triggering
- Auto-PEEP impairs triggering in COPD: if intrinsic PEEP = 8 cm H2O and trigger is -2 cm H2O, the patient must generate 10 cm H2O effort to trigger a breath → external PEEP up to ~80% of intrinsic PEEP reduces this burden
4. Disease-Specific Ventilation Strategies
A. ARDS (Acute Respiratory Distress Syndrome)
Pathophysiology: Diffuse alveolar damage, reduced FRC, heterogeneous lung with dependent consolidation/atelectasis, recruitable middle zone, and relatively normal non-dependent zone ("baby lung"). VILI occurs by barotrauma (overdistention of normal alveoli) and biotrauma (cytokine release from injured cells).
The ARDSNet Lung-Protective Strategy (Gold Standard):
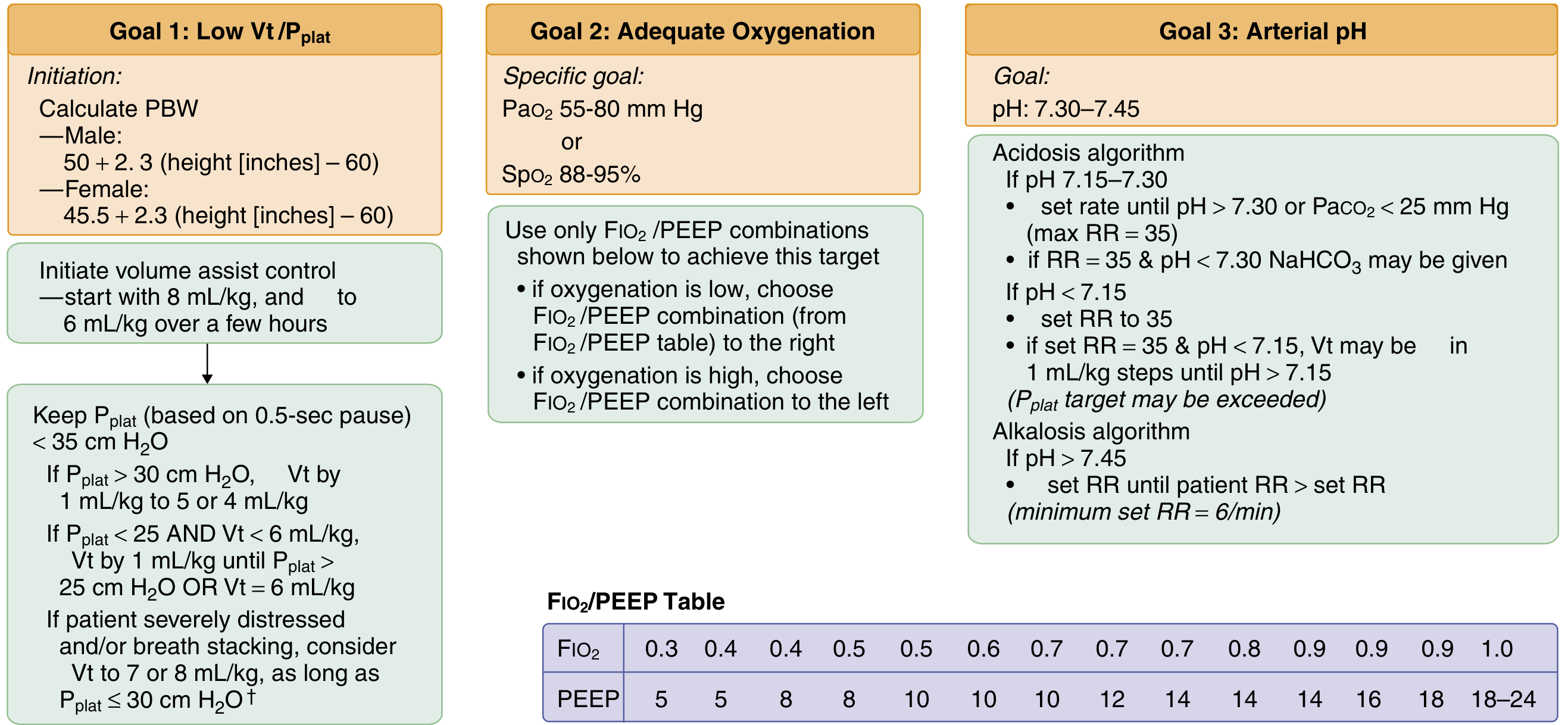
| Parameter | Target |
|---|---|
| Mode | Volume Assist-Control |
| Vt | ≤6 mL/kg PBW (reduce to 4-5 if Pplat >30) |
| Plateau Pressure | ≤30 cm H2O |
| RR | 6-35, titrate to pH ≥7.30 |
| I:E ratio | 1:1 to 1:3 |
| Oxygenation goal | PaO2 55-80 mmHg or SpO2 88-95% |
| pH goal | 7.30-7.45 |
FiO2/PEEP Ladder (ARDSNet):
| FiO2 | 0.3 | 0.4 | 0.5 | 0.6 | 0.7 | 0.8 | 0.9 | 1.0 |
|---|---|---|---|---|---|---|---|---|
| PEEP | 5 | 5-8 | 8-10 | 10 | 10-12 | 14 | 14-18 | 18-24 |
Driving Pressure (ΔP = Pplat - PEEP): Target <15 cm H2O. Driving pressure may be a better predictor of VILI than Vt alone, as it reflects the stress applied to the recruited lung.
Permissive Hypercapnia: Accept PaCO2 up to 60+ mmHg if needed to maintain low Vt. Treat respiratory acidosis (pH 7.15-7.30) by increasing RR up to 35 breaths/min first; NaHCO3 can be considered if pH <7.30 with RR at max.
PEEP Optimization:
- Higher PEEP (12-13 cm H2O) appears beneficial in moderate-severe ARDS (P/F <200) but not mild ARDS
- Recruitment-to-inflation ratio (R/I ratio): Measures change in expired volume when PEEP drops from 15→5 cm H2O; helps identify recruitable patients
- Esophageal pressure-guided PEEP has not been proven superior in large trials but may benefit obese patients
Adjunctive Strategies:
- Prone positioning: ≥16 hours/day for moderate-severe ARDS (P/F <150); proven to reduce 28-day mortality (PROSEVA trial). Only adjunct proven to reduce mortality.
- Neuromuscular blockade (NMB): Cisatracurium 48-hour infusion for severe ARDS (P/F <150) in early phase - improves synchrony, reduces VILI; routine use no longer recommended by current guidelines (ACURASYS and ROSE trials).
- Inhaled NO/prostacyclin: Transiently improves oxygenation but no mortality benefit; useful as bridge to ECMO or prone positioning.
- Recruitment maneuvers: No mortality benefit; ART trial (2017) showed the aggressive recruitment + high PEEP titration strategy had higher 28-day mortality (55.3% vs 49.3%) with increased barotrauma. Not routinely recommended.
- HFOV: Not recommended in adults (OSCAR/OSCILLATE trials).
- VV-ECMO: For severe refractory ARDS (P/F <80 despite optimization); allows "ultra-protective" ventilation with very low Vt (2-4 mL/kg) and high PEEP.
Goldman-Cecil Medicine, p. 1067; Fishman's Pulmonary Diseases, p. 2484-2508
B. COPD Exacerbation
Pathophysiology: High airway resistance → expiratory flow limitation → dynamic hyperinflation → auto-PEEP (intrinsic PEEP) → increased work of breathing → respiratory muscle fatigue.
Step 1 - Avoid Intubation (NIV First):
- BPAP (PSV + PEEP) strongly recommended for COPD exacerbations with respiratory acidosis (pH 7.25-7.35, PaCO2 >45 mmHg)
- Reduces intubation rate, mortality, and ICU LOS
- IPAP: Start 10-12 cm H2O, titrate up to 20 cm H2O; EPAP: 4-8 cm H2O
- If NIV fails → intubate
Invasive Ventilation Strategy (if intubated):
| Parameter | Target |
|---|---|
| Mode | VACV or PACV (PSV once stable) |
| Vt | 6-8 mL/kg PBW (higher than ARDS) |
| RR | Low (10-14 breaths/min) to maximize expiratory time |
| PEEP | 5 cm H2O initially; may increase to 50-80% of auto-PEEP |
| I:E | 1:3 to 1:5 (maximize expiratory time) |
| FiO2 | Titrate to SpO2 88-92% |
Key Concepts:
- Minimize minute ventilation - even at cost of permissive hypercapnia (accept pH >7.20)
- Tolerate respiratory acidosis if pH >7.20 - give time for bronchodilators/steroids to work; do NOT increase RR or Vt reflexively
- Auto-PEEP management: Apply external PEEP at 50-80% of measured intrinsic PEEP. This reduces the inspiratory effort needed to trigger (patients with COPD must overcome auto-PEEP before triggering). This strategy does NOT increase air trapping because expiratory flow limitation means absolute pressure does not drive flow.
- High peak pressures with normal plateau = airway resistance problem (not parenchymal). Tolerate high peak pressures; treat with bronchodilators.
- High peak AND plateau pressures = compliance problem. Evaluate for pneumothorax, mucous plugging, auto-PEEP (hemodynamic compromise → disconnect from ventilator briefly to allow decompression).
Goldman-Cecil Medicine, p. 2037-2049; Rosen's Emergency Medicine, p. 2668-2673
C. Status Asthmaticus
Pathophysiology: Severe bronchospasm, mucous plugging, dynamic hyperinflation → auto-PEEP → hemodynamic compromise (decreased venous return, obstructive shock), barotrauma (pneumothorax).
Priority: Avoid Intubation at All Costs - these patients do very poorly on ventilators.
- Heliox (70:30 He:O2 mixture): Reduces turbulent flow; may bridge to intubation
- NIV: Evidence is weaker than COPD; use cautiously if patient is cooperative
If Intubated - "Controlled Hypoventilation":
| Parameter | Target |
|---|---|
| Mode | VACV |
| Vt | 6-8 mL/kg PBW (start lower) |
| RR | Very low: 8-12 breaths/min |
| I:E | 1:4 to 1:5 (maximum expiratory time) |
| PEEP | 0-5 cm H2O (do NOT add external PEEP - unlike COPD) |
| FiO2 | As needed for SpO2 >92% |
| Peak pressures | Accept very high (>50 cm H2O) if plateau is normal |
Why no external PEEP in asthma? Unlike COPD where expiratory flow limitation makes external PEEP below the critical closing pressure "safe," in asthma the mechanism is dynamic compression from bronchospasm and adding external PEEP increases total lung volume and risk of barotrauma.
Accept permissive hypercapnia aggressively - pH target >7.15-7.20. Deep sedation + ketamine (bronchodilator, anesthetic) + consider paralysis to reduce O2 consumption and prevent breath stacking.
Emergency - Obstructive Shock from Hyperinflation: Disconnect from ventilator → apply manual chest compression → resuscitate → recheck settings.
D. Cardiogenic Pulmonary Edema (CPE)
Strategy: NIV is first-line (Level A evidence)
- CPAP 5-10 cm H2O: Reduces preload, reduces LV afterload, recruits flooded alveoli, reduces work of breathing. Suitable for most patients without hypercapnia.
- BPAP: For patients with concurrent hypercapnia or more severe respiratory failure. IPAP 10-15 / EPAP 5-8 cm H2O.
If Intubated:
| Parameter | Target |
|---|---|
| Mode | VACV or PSV |
| Vt | 6-8 mL/kg PBW |
| PEEP | 8-12 cm H2O (high - recruits edematous alveoli, reduces afterload) |
| FiO2 | Titrate down rapidly once SpO2 improves |
| RR | 12-20 breaths/min |
Physiology: Positive intrathoracic pressure reduces LV transmural pressure (afterload) - this is uniquely beneficial in CPE, as opposed to ARDS where high PEEP may impair RV function.
E. Neuromuscular Disease (NMD) / Spinal Cord Injury / Post-Operative
Examples: Guillain-Barré syndrome, myasthenia gravis, ALS, cervical SCI, post-thoracic surgery.
Pathophysiology: Respiratory muscle weakness → inadequate Vt and cough, retained secretions, atelectasis. Oxygenation is often preserved until late. CO2 rises progressively.
Indicators for Intubation:
- VC <20 mL/kg (or <1 L) - the "20-30-40 Rule" (MIP <-30 cmH2O, MEP <40 cmH2O, VC <20 mL/kg)
- Rapid decline in VC over hours
Ventilation Strategy:
| Parameter | Target |
|---|---|
| Mode | VACV initially; PSV for weaning |
| Vt | 8-10 mL/kg PBW (patients need larger breaths - lungs are normal) |
| PEEP | 5 cm H2O |
| RR | 12-16 breaths/min |
| Pressure support weaning | Progressively decrease PS level |
Key: Respiratory mechanics (compliance, resistance) are normal in pure NMD. Focus on secretion management, regular recruitment, and progressive weaning as underlying disease improves (GBS) or with NIV for chronic conditions (ALS).
F. Traumatic Brain Injury (TBI) / Raised ICP
Conflict: Low Vt (lung-protective) may cause CO2 retention → vasodilation → increased ICP. But high Vt causes VILI.
Strategy:
| Parameter | Target |
|---|---|
| Mode | VACV |
| Vt | 6-8 mL/kg PBW (lung-protective when possible) |
| RR | Titrate to PaCO2 35-40 mmHg (normoventilation) |
| PEEP | 5-8 cm H2O (balance: adequate PEEP vs. elevated ICP via impaired venous return) |
| SpO2 | >94% (cerebral oxygenation critical) |
| Head position | 30 degrees elevation |
Acute ICP Crisis: Brief hyperventilation (PaCO2 30-35 mmHg) is a temporizing measure only - causes cerebral vasoconstriction. Effect lasts 30-60 minutes. Do not use chronically (rebound vasodilation, ischemia).
Avoid: Permissive hypercapnia. Desaturation episodes (SpO2 <90%) dramatically worsen outcomes.
G. Sepsis-Induced ARDS
Follows the ARDSNet protocol (covered above). Additional sepsis-specific points:
- Target SpO2 ≥88-95% (avoid >97% per Surviving Sepsis Campaign 2021)
- Low Vt (≤6 mL/kg PBW) with Pplat ≤30 cm H2O
- Prone positioning ≥16 hours/day for P/F <150
- High PEEP strategy for moderate-severe ARDS
- Conservative fluid strategy (FACTT trial) once resuscitation is complete
H. Pulmonary Embolism (PE)
Key Challenge: RV failure from acute pressure overload. Positive pressure ventilation reduces venous return → worsens RV output → hemodynamic collapse.
Strategy:
| Parameter | Target |
|---|---|
| Mode | VACV or PSV (minimize mandatory breaths) |
| Vt | 6 mL/kg PBW |
| PEEP | Minimal (3-5 cm H2O) - too high reduces RV preload |
| RR | Sufficient to avoid hypercapnia (hypercapnia → pulmonary vasoconstriction) |
| FiO2 | 1.0 initially (no infiltrates, start at 0.4 per Cecil) |
Avoid: High PEEP, high intrathoracic pressures, and permissive hypercapnia (CO2 worsens pulmonary hypertension).
Definitive treatment: Systemic thrombolysis or catheter-directed therapy; ventilation is only supportive.
I. Obesity/Elevated Intra-abdominal Pressure
- Higher PEEP needed (10-15 cm H2O) to recruit gravity-dependent atelectasis
- Vt calculation by PBW (not actual body weight) is critical - obese patients have reduced lung volume but same lung
- Semi-recumbent or reverse Trendelenburg positioning aids FRC
- Plateau pressure may safely exceed 30 cm H2O when chest wall compliance is reduced (stiff chest from obesity) - what matters is transpulmonary pressure (Pplat - pleural pressure)
5. Weaning and Liberation
Readiness Criteria:
- Underlying cause of respiratory failure improving
- Hemodynamically stable (minimal/no vasopressors)
- FiO2 ≤0.4, PEEP ≤8 cm H2O
- Able to follow commands, adequate cough
Rapid Shallow Breathing Index (RSBI):
- RSBI = RR (breaths/min) / Vt (liters)
- Measured during 2 minutes of unassisted spontaneous breathing
- RSBI <105 breaths/min/L → proceed to spontaneous breathing trial (SBT)
- RSBI >105 → patient unlikely to tolerate extubation
Spontaneous Breathing Trial (SBT):
- T-piece or PS 5 + PEEP 5 cm H2O for 30-120 minutes
- Pass criteria: SpO2 >90%, RR <35, HR/BP stable, no distress
- Success → extubate
- Failure → return to full support, treat reversible factors, retry in 24 hours
SBT Failure vs. Extubation Failure:
SBT only predicts ability to breathe; extubation failure relates to upper airway protection (weak cough, secretions, microaspiration). Post-extubation NIV reduces re-intubation in high-risk patients (COPD, heart failure, obesity).
Goldman-Cecil Medicine, p. 2058-2060
6. Ventilator-Induced Lung Injury (VILI) - Summary
| Mechanism | Description | Prevention |
|---|---|---|
| Barotrauma | Alveolar rupture from high pressure | Limit Pplat <30 cm H2O |
| Volutrauma | Overdistension from high volume | Limit Vt ≤6 mL/kg PBW |
| Atelectrauma | Repeated collapse/reopening of alveoli | Adequate PEEP |
| Biotrauma | Cytokine release causing systemic organ failure | All above strategies |
| Patient self-inflicted lung injury (P-SILI) | High spontaneous effort generates large transalveolar swings | Adequate sedation/analgesia; early recognition |
7. Quick Reference Table by Disease
| Disease | Mode | Vt | RR | PEEP | I:E | Special Notes |
|---|---|---|---|---|---|---|
| ARDS | VACV | 6 mL/kg | 6-35 | FiO2/PEEP table | 1:1-1:3 | Prone >16h/day if P/F <150 |
| COPD exacerbation | BPAP (NIV) → VACV | 6-8 mL/kg | 10-14 | 50-80% auto-PEEP | 1:3-1:5 | Permissive hypercapnia OK |
| Status asthmaticus | VACV | 6-8 mL/kg | 8-12 | 0-5 (minimal) | 1:4-1:5 | Disconnect if obstructive shock |
| Cardiogenic PE | CPAP/BPAP → VACV | 6-8 mL/kg | 12-20 | 8-12 | 1:2 | PEEP reduces LV afterload |
| TBI + Raised ICP | VACV | 6-8 mL/kg | PaCO2 35-40 | 5-8 | 1:2 | No permissive hypercapnia |
| NMD/Weakness | VACV → PSV | 8-10 mL/kg | 12-16 | 5 | 1:2 | Normal lungs; focus on weaning |
| Pulmonary embolism | VACV/PSV | 6 mL/kg | Normal | 3-5 (minimal) | 1:2-1:3 | Avoid high PEEP, definitive Rx |
| Obesity/High IAP | VACV | 6 mL/kg PBW | 12-16 | 10-15 | 1:2 | Pplat may exceed 30 cm H2O |
Sources: Murray & Nadel's Textbook of Respiratory Medicine (p. 3175, 3195) | Fishman's Pulmonary Diseases (p. 2484-2509, 2607-2695) | Goldman-Cecil Medicine (p. 1066-1070, 2037-2060) | Rosen's Emergency Medicine (p. 2661-2675)
This is a shared conversation. Sign in to Orris to start your own chat.