Clinical features of hydrocephalus in pediatrics
Reading File
Finding Sources
Searching PubMed
hydrocephalus children clinical features
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
I now have comprehensive, well-sourced content. Let me compile the full answer.
Clinical Features of Hydrocephalus in Pediatrics
Hydrocephalus in children is a pressure-dependent enlargement of the cerebral ventricles resulting from obstruction or impaired absorption of CSF. The clinical presentation differs markedly depending on age at onset (whether cranial sutures are open or closed) and rate of onset (acute vs. chronic).
Age-Based Presentation
1. Infants and Children Under 2 Years (Open Sutures)
Because the cranial sutures are not yet fused, the skull can expand and accommodate rising intracranial pressure. This means head enlargement dominates the clinical picture, and classic signs of raised ICP (e.g., papilledema) are often absent or late.
Head and Skull Signs:
- Macrocephaly - head circumference rapidly crosses centile lines on growth charts, soon surpassing the 97th percentile
- Frontal bossing - prominent forward protuberance of the frontal skull; the face looks relatively small and pinched in contrast
- Bulging anterior (and posterior) fontanelle - tense even when the infant is relaxed and upright (a key sign; it is NOT reliable after 1 year once the fontanelle closes)
- Sutural diastasis - palpable separation of skull sutures
- Calvarial thinning - "beaten silver" or "copper-beaten skull" pattern on X-ray
- Scalp vein engorgement - prominent distended scalp veins from raised intracranial venous pressure
- "Cracked-pot" sign (Macewen sign) - a resonant, hollow sound on skull percussion, due to the thinned, separated skull
Eye Signs:
- Sunset (setting-sun) sign - upper eyelids retract, eyes deviate downward; the sclerae are visible above the irises. Caused by pressure on the midbrain tectum from dilated third ventricle, producing paresis of upward conjugate gaze. This sign resolves after adequate shunting.
- Lateral rectus palsy (CN VI palsy) - can cause convergent squint; often a false localizing sign
Systemic/Behavioral Signs:
- Irritability - one of the most common early symptoms in neonates and infants
- Poor feeding and fretfulness
- Vomiting - especially early morning (due to ICP rise in the recumbent position)
- Lethargy and torpor - as pressure progresses, infants become less responsive, languid, and uninterested in surroundings
Motor Signs:
- Lower limb spasticity - from stretching of the corticospinal tracts as they arc around the enlarged ventricles; deep tendon reflexes are brisk
- Tremulous arm movements - in advanced cases
- As the condition becomes extreme, the infant may adopt flexed arms and flexed/extended leg postures
Visual Consequences (late/untreated):
- Optic atrophy and reduced vision (notably there is usually no papilledema in infants because the open skull dissipates the pressure)
If hydrocephalus is arrested, the child is typically delayed in motor function but often surprisingly verbal (language can be preserved disproportionately).
2. Children Over 2-3 Years (Fused or Fusing Sutures)
Once the sutures close (generally by age 3), the skull is rigid. Head enlargement is no longer possible, so the full clinical picture of raised intracranial pressure emerges instead.
Raised ICP Signs:
- Headache - often worse in the morning; described as progressive; in posterior fossa tumors causing obstructive hydrocephalus, the classic pattern is early-morning headache followed by vomiting
- Nausea and vomiting - projectile, especially in the morning; due to recumbent hypercapnia increasing cerebral blood flow
- Papilledema - present on fundoscopy; a consistent finding at this age (unlike in infants)
- Altered consciousness - drowsiness, somnolence, and ultimately coma in acute cases
- Diplopia - CN VI (abducens) palsy producing horizontal diplopia; a common false localizing sign of raised ICP
- Visual blurring
Gait and Motor:
- Wide-based ataxic gait - from stretching of frontal leg white-matter tracts around the ventricles
- Spasticity of lower limbs
- Cerebellar ataxia if the cause is a posterior fossa lesion
Endocrine Dysfunction (chronic hydrocephalus):
- Short stature
- Menstrual irregularities (in adolescent girls)
- Diabetes insipidus
- These arise from pressure on the hypothalamus
Neurocognitive:
- Declines in school performance
- Behavioral and personality changes
- Developmental delay in motor function
Clinical Features by Cause
| Cause | Age | Distinctive Features |
|---|---|---|
| Prematurity (IVH) | Neonate | Rapidly enlarging head; diagnosed on serial cranial ultrasound through open fontanelle; ~25% of infants <1500 g at risk |
| Aqueductal stenosis / intrauterine infection | Newborn - infant | Noncommunicating hydrocephalus; classic macrocephaly + sunset sign |
| Chiari II malformation (with myelomeningocele) | Infant | Associated spina bifida; hydrocephalus after myelomeningocele repair |
| Posterior fossa tumor (medulloblastoma, ependymoma) | Child | Early-morning headache + vomiting + ataxia + CN VI palsy; acute obstruction at aqueduct |
| Bacterial meningitis (post-infectious) | Any age | Communicating hydrocephalus from basal cistern scarring; often after group B strep, E. coli (neonates) or meningococcal/pneumococcal disease |
| Dandy-Walker malformation | Infant | Dolichocephalic head (prominent occiput); posterior fossa cyst |
Key Signs - Quick Reference
| Sign | Description | Mechanism |
|---|---|---|
| Sunset sign | Eyes deviate downward, sclerae visible above iris | Tectal pressure → upgaze paresis |
| Macewen (cracked-pot) sign | Hollow resonant sound on skull percussion | Thinned, separated skull with fluid beneath |
| Bulging fontanelle | Tense AF even when child is upright and calm | Raised ICP transmitted through open sutures |
| Transependymal edema | Periventricular lucency on CT/MRI | CSF forced through ependyma into white matter |
| Scalp vein engorgement | Prominent scalp veins | Elevated intracranial venous pressure |
Imaging Correlate
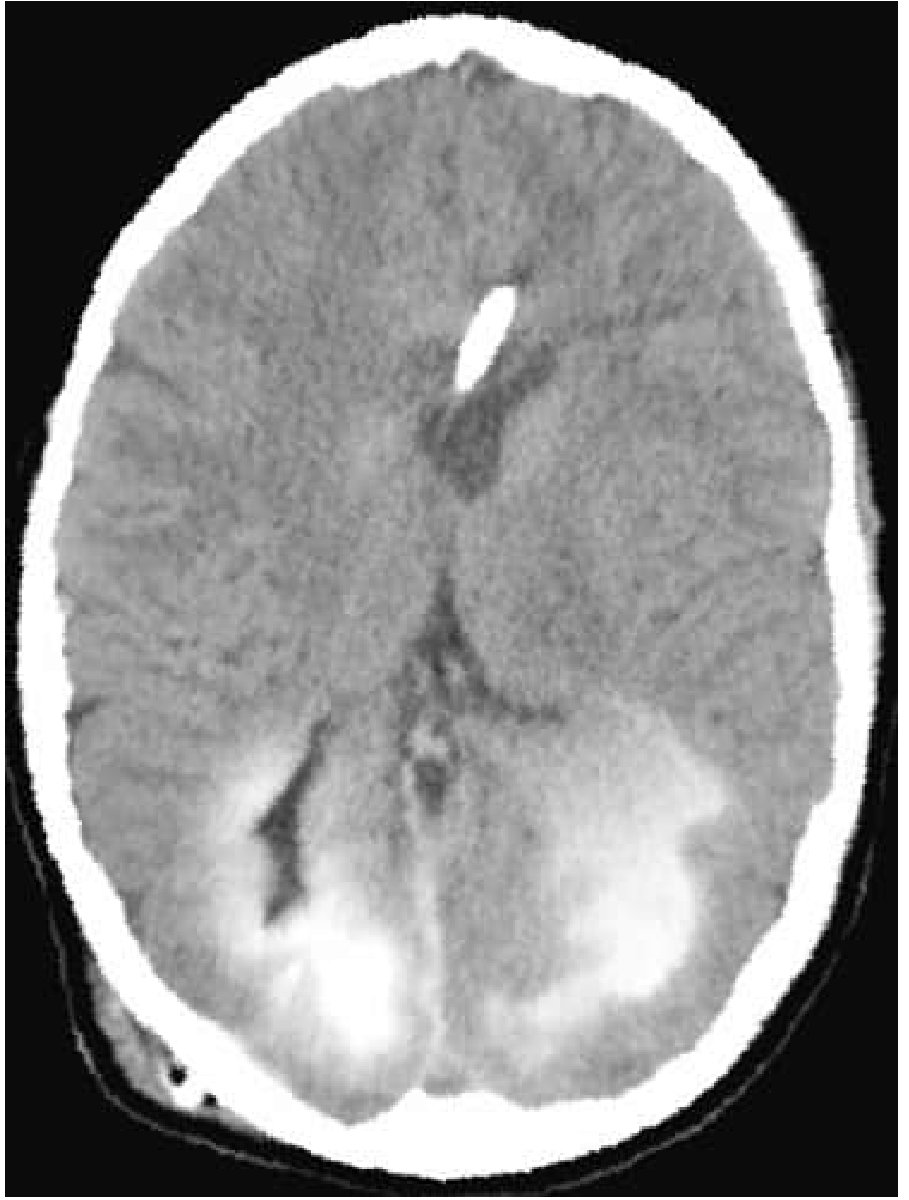
CT showing transependymal flow: contrast infused through a ventricular shunt catheter diffuses into surrounding brain through the ependyma - a hallmark imaging sign of active hydrocephalus - Bradley and Daroff's Neurology in Clinical Practice
On imaging, key findings include:
- Dilatation of temporal horns (early sign)
- Enlargement of anterior/posterior recesses of the third ventricle
- Periventricular interstitial (transependymal) edema
- Obliteration of sulcal spaces and basal cisterns (distinguishing true hydrocephalus from atrophy)
Summary: Age-Based Comparison
| Feature | Infant (<2-3 years) | Older Child (>3 years) |
|---|---|---|
| Head enlargement | Present (sutures open) | Absent (sutures fused) |
| Fontanelle bulging | Yes (key sign) | Not applicable |
| Papilledema | Usually absent | Present |
| Sunset sign | Classic | May be seen |
| Vomiting | Present | Early morning |
| Headache | Crying/irritability | Explicit complaint |
| Scalp vein engorgement | Yes | No |
| Macewen sign | Present | Absent |
Sources:
- Adams and Victor's Principles of Neurology, 12th Ed. - "Syndromes of Hydrocephalus," pp. 1008-1010
- Bradley and Daroff's Neurology in Clinical Practice - "Hydrocephalus in Children," p. 1854
- Grainger & Allison's Diagnostic Radiology - "Hydrocephalus," p. 2028
- Tintinalli's Emergency Medicine, 9th Ed. - "Clinical Features and Diagnosis," p. 834
- A recent systematic review of pediatric hydrocephalus (PMID 39094187) covering 12,355 patients confirms the same dominant presentation patterns, with post-infectious and post-hemorrhagic causes predominating in developing-world settings
This is a shared conversation. Sign in to Orris to start your own chat.