Appendictomy
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Searching PubMed
appendectomy laparoscopic open appendicitis
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Excellent - I now have all the content needed for a thorough overview. Here is the full answer:
Appendectomy - Overview
An appendectomy is the surgical removal of the vermiform appendix. It is the definitive treatment for acute appendicitis, one of the most common causes of the acute surgical abdomen worldwide.
Anatomy of the Appendix
The appendix is approximately 9 cm long and 0.6 cm wide, originating from the terminal cecum where the three taenia coli converge. Its blood supply comes from the appendiceal artery, a branch of the ileocolic artery.
While the base always arises from the cecum, the tip position is variable - this is why presentations differ:
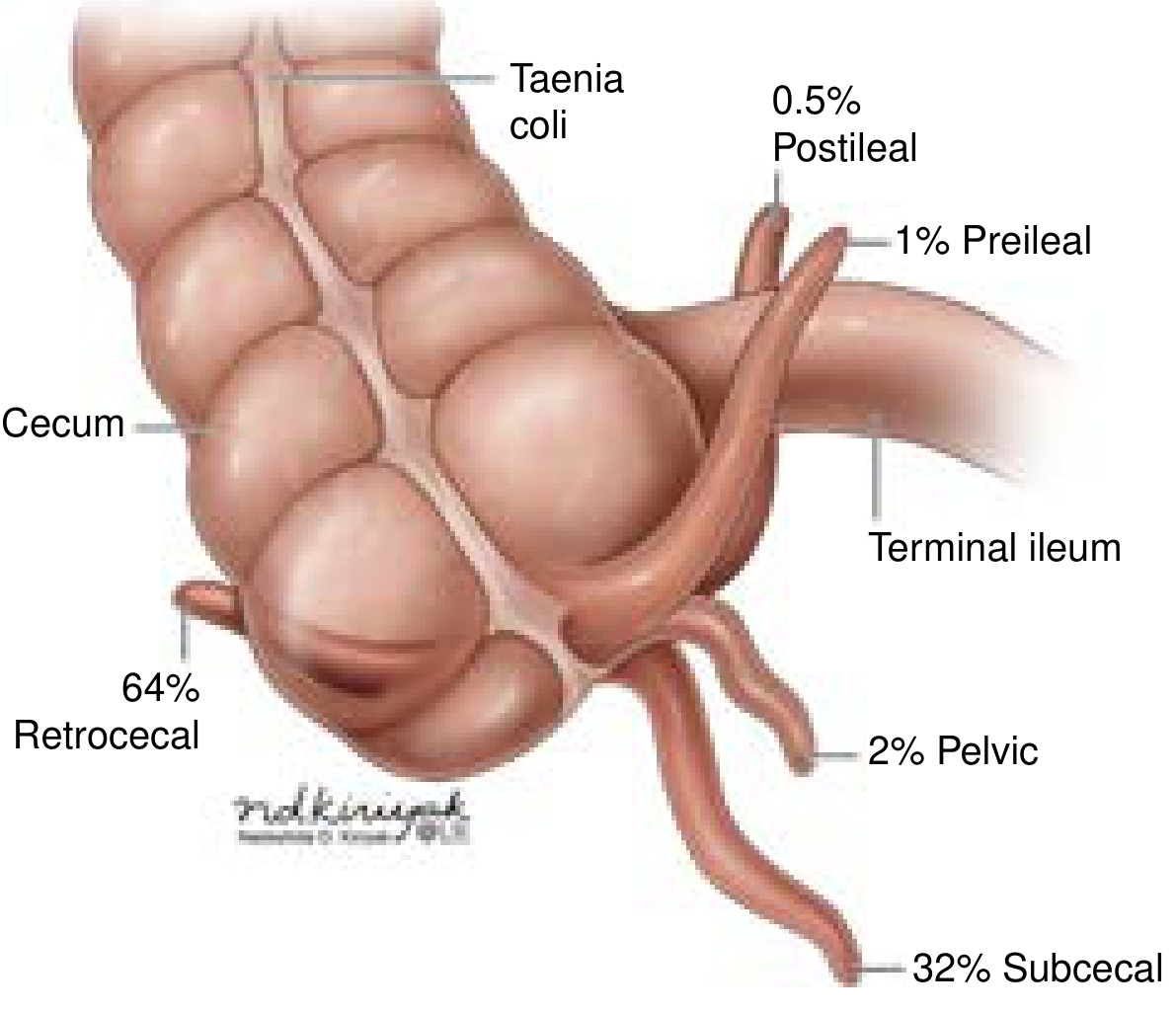
| Position | Frequency | Clinical sign |
|---|---|---|
| Retrocecal | 64% | Positive psoas sign |
| Subcecal | 32% | RLQ pain |
| Pelvic | 2% | Positive obturator sign |
| Preileal | 1% | Variable |
| Postileal | 0.5% | Variable |
Indications
The primary indication is acute appendicitis, with a lifetime risk of 7-10% and ~400,000 US cases per year (16-40% perforated at presentation). Other indications include:
- Interval appendectomy - after initial nonoperative management of a periappendiceal abscess/phlegmon
- Incidental appendectomy - selectively considered in patients undergoing chemotherapy, those with Crohn's disease (if cecal base is uninflamed), or during cytoreductive ovarian surgery (though not routinely advocated due to adhesion risk)
- Intraoperative finding of appendiceal pathology (Crohn's ileitis, Meckel's diverticulitis mimicking appendicitis)
Procedure Types
1. Laparoscopic Appendectomy (preferred)
The standard of care for uncomplicated appendicitis in both adults and children. Key steps:
- Position: Supine, left arm tucked, consider Foley catheter
- Access: Umbilical port via Veress needle (closed) or Hasson technique (open), insufflated to 12-15 mmHg CO₂
- Port placement: Umbilical camera port + working ports in LLQ/RLQ (configuration varies by patient)
- Steps: Four-quadrant exploration → Trendelenburg right-side-up → cecum identified by taenia coli → mesoappendix divided with a linear stapler (white load) or electrosurgical device (LigaSure) → appendix transected with blue load stapler or Endoloop → specimen placed in retrieval bag → wound closure
- For a retrocecal appendix, the white line of Toldt must be divided to mobilize the cecum
Advantages: Lower wound infection rates, shorter hospital stay, faster return to work, better outcomes in children and obese patients.
2. Open Appendectomy
Still essential to know - used when laparoscopy is unavailable, contraindicated, or conversion is needed.
- Incision: Oblique (muscle-splitting) incision at McBurney's point (one-third of the distance from the right ASIS to the umbilicus), within a skin crease
- Layers: External oblique split along fiber direction → internal oblique bluntly spread → transversus abdominis split → peritoneum incised
- Technique: Cecum elevated → appendix identified at taenia convergence → mesoappendix divided (stapler or Kelly clamps with 3-0 silk ties) → base crushed, ligated with 0 chromic, divided → stump cauterized or invaginated with purse-string/Z-stitch
- Closure: Layers closed with absorbable suture; skin may be left open or loosely approximated in perforation cases
3. Interval Appendectomy
Performed 6-8 weeks after successful nonoperative management of a periappendiceal abscess or phlegmon. The rationale is to allow inflammation to resolve before operating in a technically hostile field. Its necessity is debated - recurrence rates after successful nonoperative management are ~20% over 5 years, and many patients never need surgery.
4. Single-Incision Laparoscopic Appendectomy (SILA)
A newer approach using a single umbilical port. A 2026 meta-analysis (PMID 40981423) found comparable operation time and postoperative pain versus standard three-port laparoscopy, with cosmetic advantage.
Management by Disease Stage
| Stage | Management |
|---|---|
| Uncomplicated appendicitis | Laparoscopic appendectomy (preferred); antibiotics-only is an acceptable alternative in select patients |
| Perforated appendicitis with diffuse peritonitis | Resuscitate → urgent appendectomy (laparoscopic if feasible) |
| Periappendiceal abscess/phlegmon | IV antibiotics + percutaneous drainage (if drainable) → interval appendectomy |
For perforated cases, IV antibiotics such as piperacillin-tazobactam or ceftriaxone + metronidazole are started immediately. Postoperative antibiotics continue for at least 3-5 days. A 2025 Cochrane review (PMID 40214287) examined the role of abdominal drainage after appendectomy for complicated appendicitis.
Nonoperative Management (Current Controversy)
Recent evidence supports antibiotics alone as a viable option for uncomplicated, non-perforated appendicitis in selected adult patients. The most common regimen is IV ertapenem or ceftriaxone + metronidazole, then oral amoxicillin-clavulanate. However, ~20-30% of patients treated nonoperatively will eventually require appendectomy, and appendicitis caused by an appendicolith carries higher failure rates.
Special Populations
- Children: Infants have the highest perforation rates (51-100%). The Pediatric Appendicitis Score (PAS ≥7 = high probability) guides workup. Laparoscopic appendectomy is preferred; APSA guidelines recommend 3-5 days of postoperative antibiotics after perforation.
- Pregnant patients: Appendicitis is the most common non-obstetric surgical emergency in pregnancy. Laparoscopy is safe in all trimesters with appropriate port adjustments.
Intraoperative Findings That Mimic Appendicitis
| Finding | Action |
|---|---|
| Ovarian torsion | Detorsion + oophoropexy |
| Crohn's terminal ileitis | Appendectomy if cecal base is uninflamed |
| Meckel's diverticulitis | Segmental small bowel resection + primary anastomosis |
| Appendiceal mass | Laparoscopic appendectomy/ileocecectomy in a retrieval bag (no spillage) |
Sources: Current Surgical Therapy 14e (Mahdi & Pegoli); Schwartz's Principles of Surgery 11e - Current Surgical Therapy, p. 324-332
This is a shared conversation. Sign in to Orris to start your own chat.