Explain cohort study design and it's types
Reading File
Searching the Web
cohort study design types prospective retrospective epidemiology
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a thorough answer. Here is a complete explanation:
Cohort Study Design
A cohort study is an analytical observational study that follows a group of people over time to observe whether an exposure leads to a disease or outcome. It is also called a prospective study, longitudinal study, incidence study, or forward-looking study. The defining feature is that it works from cause to effect - the exposure has occurred, but the disease has not yet.
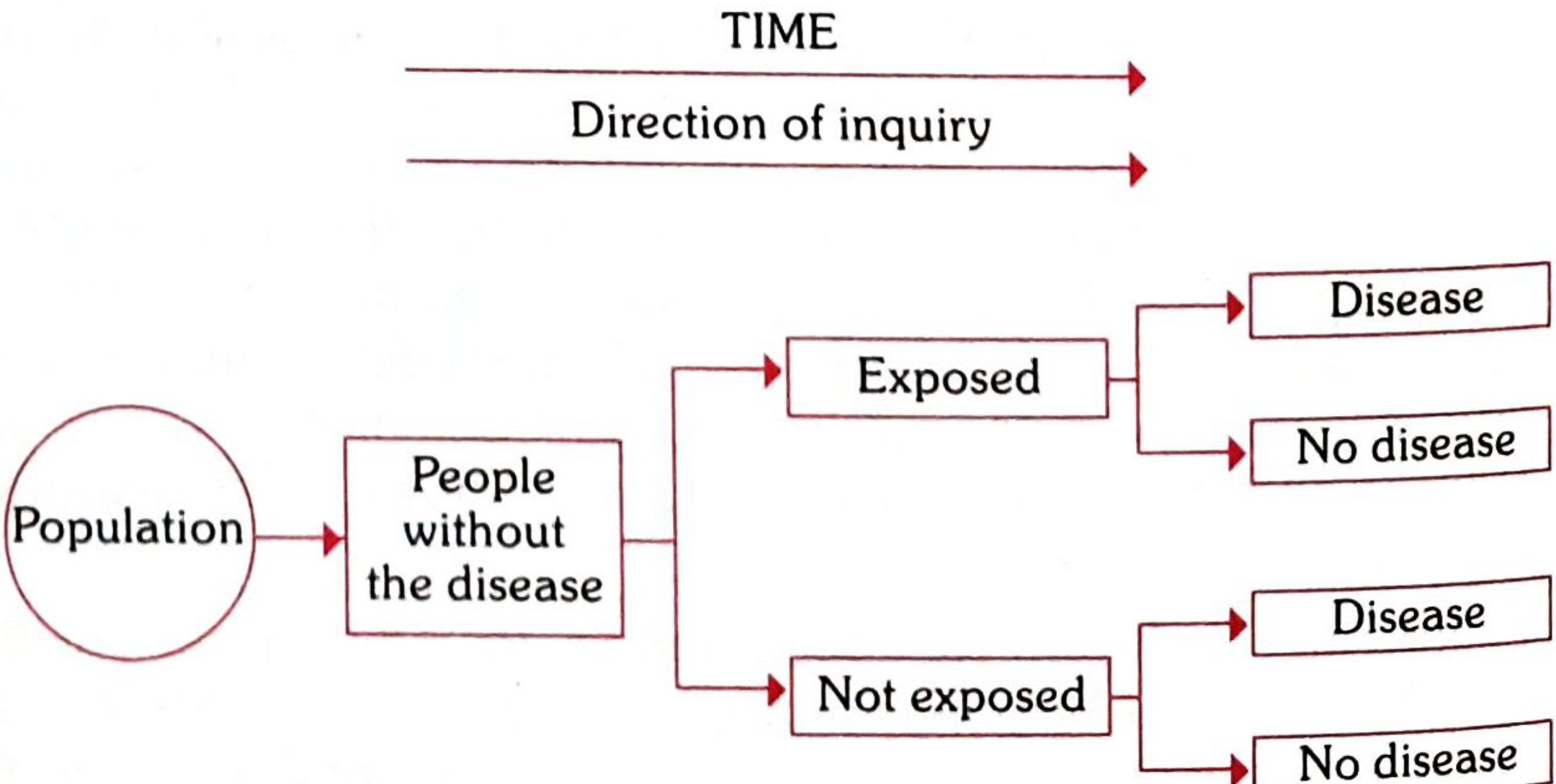
Park's Textbook of Preventive and Social Medicine - Schematic design of a cohort study
Concept of "Cohort"
In epidemiology, a cohort is a group of people who share a common characteristic or experience within a defined time period:
- Birth cohort - all persons born in a given year (e.g., birth cohort of 2010)
- Exposure cohort - persons exposed to a common drug, vaccine, or infection in a defined period
- Marriage cohort - persons married in the same period
- Disease cohort - e.g., all who survived a myocardial infarction in a particular year
Distinguishing Features
Three key features set cohort studies apart:
- Cohorts are identified prior to the appearance of the disease under investigation
- Study groups are observed over time to determine the frequency of disease
- The study proceeds forward from cause to effect
Basic Framework (2x2 Table)
| Cohort | Disease: Yes | Disease: No | Total |
|---|---|---|---|
| Exposed to putative aetiologic factor | a | b | a + b |
| Not exposed | c | d | c + d |
- Study cohort (a+b): exposed group
- Control cohort (c+d): unexposed comparison group
- Incidence in exposed = a/(a+b); in unexposed = c/(c+d)
- Result expressed as Relative Risk (RR) = [a/(a+b)] / [c/(c+d)]
Types of Cohort Studies
1. Prospective Cohort Study
The most common type. The investigator:
- Identifies exposure status at the start
- Follows subjects forward in time
- Awaits the development of disease
- Exposure and outcome data are collected as events occur
Example: Enrolling healthy workers in a chemical plant today and following them for 20 years to see who develops lung disease.
Advantages:
- Temporality is clear (exposure precedes disease)
- Can calculate incidence rates directly
- Less susceptible to recall bias
- Can study multiple outcomes from one exposure
Disadvantages:
- Very time-consuming and expensive
- Large sample size needed
- Loss to follow-up is a major problem
- Not suitable for rare diseases (would need enormous numbers)
2. Retrospective Cohort Study (Historical Cohort Study)
Both the exposure and outcome have already occurred when the study begins. The investigator looks back using historical records (employment records, hospital registers, etc.).
Example: Reviewing employment records from 1970 to identify workers exposed to asbestos and then checking death registries to see who developed mesothelioma.
Advantages:
- Much faster and cheaper than prospective studies
- Useful when the disease has a very long latency period
- Good for occupational or industrial exposure studies
Disadvantages:
- Dependent on the quality of existing records
- Cannot control what data were collected in the past
- More prone to information bias
3. Ambidirectional (Mixed) Cohort Study
A combination of both prospective and retrospective approaches. The researcher:
- Identifies a historical cohort from past records (retrospective component)
- Continues to follow that same cohort forward in time (prospective component)
Example: Identifying patients who received a particular drug in 2010 from records, then also continuing to follow them prospectively from the present onwards.
4. Nested Case-Control Study
A case-control study nested within an existing cohort. When cases develop during cohort follow-up, controls are selected from the cohort members who have not yet become cases at that point in time.
Advantages: More efficient use of resources; reduces costs because not all cohort members need detailed laboratory analysis - only cases and matched controls.
5. Case-Cohort Study
Similar to the nested case-control design. All cases in the cohort are compared to a random sample (subcohort) drawn from the full cohort at baseline, regardless of whether subcohort members later become cases or not.
Key difference from nested case-control: The comparison group (subcohort) is selected at baseline, not at the time cases appear; the same subcohort can be used for studying multiple outcomes.
When Are Cohort Studies Indicated?
According to Park's textbook, cohort studies are appropriate when:
- (a) There is already good evidence of an association (from descriptive or case-control studies) and causal proof is now needed
- (b) Exposure is rare but incidence of disease is high among the exposed (e.g., industrial/occupational exposure groups, radiation workers)
- (c) Attrition can be minimized - the cohort is stable, cooperative, and accessible for long-term follow-up
- (d) Adequate funding is available
Elements of a Cohort Study
Key design requirements:
| Element | Requirement |
|---|---|
| Cohort membership | Must be free of the disease under study at the start |
| Comparability | Both groups equally susceptible to the disease |
| Comparability of variables | Groups matched for age, sex, and other confounders |
| Diagnostic criteria | Must be defined before the study begins |
Advantages vs. Disadvantages Summary
| Advantages | Disadvantages |
|---|---|
| Can calculate incidence and relative risk directly | Expensive and time-consuming |
| Clear temporal sequence (exposure before disease) | Not suitable for rare diseases |
| Can study multiple outcomes of one exposure | Loss to follow-up can introduce bias |
| Less susceptible to recall bias | Very large sample sizes often needed |
| Gold standard for showing association | Ethical issues with known harmful exposures |
Measures of Association
The principal statistic derived is the Relative Risk (RR):
RR = Incidence in exposed / Incidence in unexposed = [a/(a+b)] / [c/(c+d)]
- RR > 1: exposure increases disease risk
- RR < 1: exposure is protective
- RR = 1: no association
A well-designed cohort study is considered the most reliable observational means of showing an association between a suspected risk factor and disease - second only to a randomized controlled trial in the hierarchy of evidence.
Source: Park's Textbook of Preventive and Social Medicine, pp. 83-88
Generate a visual summary poster of cohort study types and timing
Generating Image
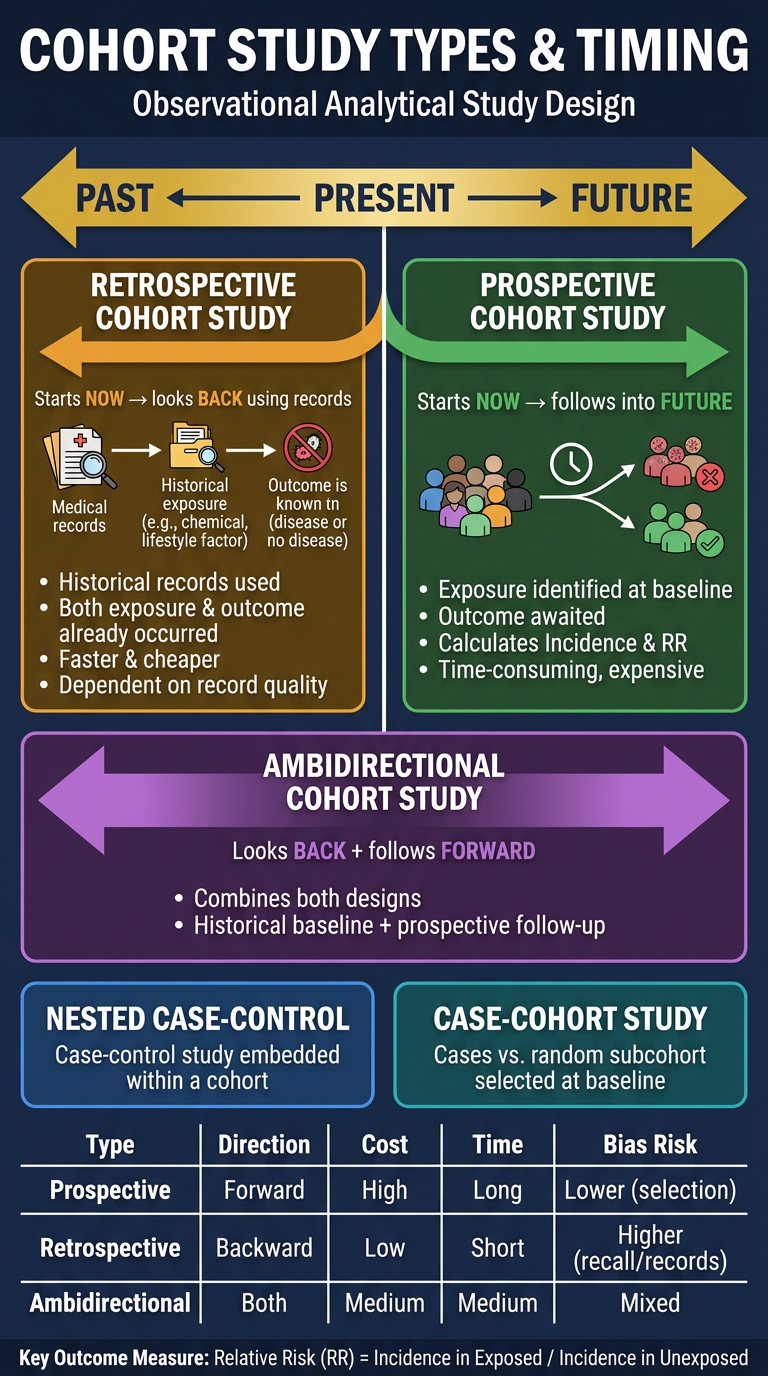
Here's your visual summary poster covering all the key cohort study types. It includes:
- The central timeline showing Past → Present → Future, which anchors the directionality of each study type
- Prospective (green) - starts now, follows forward
- Retrospective (amber) - starts now, looks back at historical records
- Ambidirectional (purple) - spans both directions
- Nested Case-Control & Case-Cohort as special variants within cohorts
- A comparison table at the bottom with Type, Direction, Cost, Time, and Bias Risk
- The key formula for Relative Risk at the footer
Great for quick revision or as a study reference!
Generate a detailed comparison table: Prospective vs Retrospective cohort studies
Finding Sources
Reading File
Reading File
I have rich textbook content from two sources. Now I'll compile the detailed comparison table.
Prospective vs Retrospective Cohort Studies - Detailed Comparison
Sources: Park's Textbook of Preventive and Social Medicine, p. 88; Sabiston Textbook of Surgery, p. 3151
Overview
| Feature | Prospective Cohort Study | Retrospective Cohort Study |
|---|---|---|
| Other names | Current cohort study, longitudinal study, concurrent cohort study, forward-looking study | Historical cohort study, prospective study in retrospect, non-concurrent prospective study |
| Direction | Forward - present into future | Backward - present back to past records, then traces forward |
| Timing of outcome | Outcome has NOT yet occurred when study begins | Outcome has already occurred before study begins |
| Starting point | Begins in the present | Begins by examining past records (10-30 years back) |
| Data collection | Planned and collected prospectively as events happen | Uses existing records (employment, hospital, medical records) |
Design & Methodology
| Feature | Prospective | Retrospective |
|---|---|---|
| Exposure assessment | Measured directly and systematically at baseline | Reconstructed from historical records |
| Outcome assessment | Observed and recorded as they occur over follow-up | Already known before study initiation |
| Investigator control | High - investigator defines what data to collect | Low - limited to what was recorded in the past |
| Standardization | Enrollment criteria and outcome measures can be standardized | Dependent on how data was originally recorded |
| Blinding | Possible | Impossible - outcomes are already known |
| Follow-up period | Long (years to decades, especially for chronic diseases) | Shorter real-time duration (records already exist) |
Strengths
| Prospective | Retrospective |
|---|---|
| Clear temporal sequence - exposure definitively precedes outcome | Faster - results produced much more quickly |
| Less susceptible to recall bias (data collected before disease) | Less expensive and more economical |
| Higher quality, more complete data | Useful for diseases with very long latency periods |
| Can directly calculate incidence rates | Suitable for rare exposures (e.g., occupational groups) |
| Multiple outcomes can be studied from one exposure | Practical when prospective follow-up is not feasible |
| Can study natural history of disease | Good for initial hypothesis testing |
| Stronger evidence for causation | Can study large populations using existing databases |
| Can assess dose-response relationships | Useful when the disease has already peaked |
Limitations
| Prospective | Retrospective |
|---|---|
| Very time-consuming and expensive | Entirely dependent on quality and completeness of existing records |
| Not suitable for rare diseases (huge sample needed) | Cannot control what variables were or were not collected |
| Loss to follow-up introduces bias (attrition bias) | More prone to information bias and selection bias |
| Requires large sample sizes | Missing data cannot be recovered |
| Ethical issues if exposure is known to be harmful | Treatment selection bias difficult to control statistically |
| Changes in diagnostic criteria over time can affect results | Confounding variables may not have been recorded historically |
| Resource-intensive for long-term maintenance | Records may be incomplete, inconsistent, or inaccurate |
Bias Profile
| Type of Bias | Prospective | Retrospective |
|---|---|---|
| Recall bias | Low (data collected prospectively) | Higher (relies on past records/memory) |
| Attrition/loss to follow-up bias | Higher risk (long follow-up) | Lower (cohort already followed) |
| Selection bias | Lower | Higher (who had records kept?) |
| Information bias | Lower | Higher (record quality varies) |
| Confounding | Better controlled (can measure confounders at baseline) | Harder to control (may not have been recorded) |
| Observer bias | Possible (if not blinded) | Less relevant |
Practical Parameters
| Parameter | Prospective | Retrospective |
|---|---|---|
| Cost | High | Low to moderate |
| Time to results | Years to decades | Months to a few years |
| Sample size needed | Very large | Large, but data may already exist |
| Feasibility for rare diseases | Poor | Better (can search large databases) |
| Feasibility for rare exposures | Good | Excellent (occupational records) |
| Evidence hierarchy rank | Higher (stronger causal inference) | Lower (weaker causal inference) |
| Data quality | High (researcher-controlled) | Variable (dependent on record-keeping) |
Classic Examples
| Prospective | Retrospective |
|---|---|
| Framingham Heart Study - followed healthy adults in Framingham, MA to identify risk factors for cardiovascular disease | Boston hospital study (1978) - 17,080 babies born 1969-1975 studied retrospectively for effect of electronic fetal monitoring on neonatal death |
| Doll & Hill (1954) - British doctors followed prospectively; smoking and lung cancer | Uranium miners study - archival employment records used to identify exposure; lung cancer outcomes already known |
| Royal College of GPs study - oral contraceptives and health outcomes | Angiosarcoma of liver & PVC - rare disease detected only because retrospective cohort design was used |
| Nurses' Health Study - ongoing prospective follow-up of US nurses | Occupational arsenic exposure - carcinogenesis studied from historical industrial records |
When to Use Which?
| Use Prospective When... | Use Retrospective When... |
|---|---|
| Causal proof is the goal | Preliminary evidence needed quickly |
| Outcome is common enough to observe prospectively | Outcome has a very long latency (e.g., cancer from occupational exposure) |
| Adequate funding and time are available | Budget and time are limited |
| Data quality is paramount | High-quality historical records already exist |
| The disease is in its early natural history | The disease has already occurred in a known population |
| Long-term follow-up is feasible | The cohort is stable and traceable through records |
Key Outcome Measure (Both Types)
Relative Risk (RR) = [a/(a+b)] / [c/(c+d)]Where: a = exposed who got disease, b = exposed who did not, c = unexposed who got disease, d = unexposed who did not
Both designs yield incidence rates and relative risk, but prospective studies provide stronger evidence for causation because they collect exposure and outcome data purposefully, systematically, and without the influence of known outcomes - as stated in the Sabiston Textbook of Surgery.
Explain retrospective cohort study with examples
Finding Sources
Searching the Web
retrospective cohort study design examples advantages limitations epidemiology
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
All the content I need is now in context. Here is the complete explanation:
Retrospective Cohort Study
Definition
A retrospective cohort study (also called a historical cohort study, prospective study in retrospect, or non-concurrent prospective study) is one in which the outcomes have all occurred before the study begins. The investigator goes back in time - sometimes 10 to 30 years - to select study groups from existing records of past employment, medical history, or other archived data, and then traces them forward through time from that fixed past date, usually up to the present.
"The investigator goes back in time sometimes 10 to 30 years, to select his study groups from existing records of past employment, medical or other records and traces them forward through time." - Park's Textbook of Preventive and Social Medicine
How It Works - Step by Step
PAST ─────────────────────────────────────► PRESENT
│ │
[STEP 1] [STEP 5]
Identify cohort Analyse outcomes
from old records (already known)
│
[STEP 2]
Classify as
EXPOSED vs UNEXPOSED
│
[STEP 3]
Trace subjects
forward through records
│
[STEP 4]
Determine who developed
the disease/outcome
The key distinction: The researcher starts the study now but reconstructs events from the past. Both the exposure and the outcome have already happened - only the analysis is new.
Sources of Historical Data
The retrospective cohort study relies on pre-existing records. Common sources include:
| Source | Type of information |
|---|---|
| Employment / industry records | Occupational exposure (chemicals, radiation, dust) |
| Hospital / medical records | Drug exposure, surgical history, diagnoses |
| Birth registers | Neonatal outcomes, maternal exposures |
| Death registries | Cause of death, mortality rates |
| Insurance records | Long-term morbidity and health utilisation |
| Military service records | Veteran cohorts, trauma, substance exposure |
| National health databases | NSQIP, SEER, Medicare, NIS (surgical outcomes) |
Classic Real-World Examples
1. Electronic Fetal Monitoring & Neonatal Death (1978)
- Cohort: 17,080 babies born January 1969 - December 1975 at a Boston hospital
- Exposure: Electronic fetal monitoring during labour (yes vs. no)
- Outcome: Neonatal death
- Finding: Neonatal death rate was 1.7 times higher in unmonitored infants
- Why retrospective? All births and deaths had already occurred; researchers used existing hospital birth records
2. Uranium Miners & Lung Cancer
- Cohort: Workers employed in uranium mining (identified from employment records)
- Exposure: Uranium/radon gas inhalation
- Outcome: Development of lung cancer
- Finding: Uranium miners had an excess frequency of lung cancer compared to non-miners
- Why retrospective? Mining employment records and death registries were used; no prospective follow-up needed
3. Arsenic & Human Carcinogenesis
- Cohort: Workers with documented occupational arsenic exposure (from factory/industry records)
- Exposure: Arsenic compounds
- Outcome: Various cancers
- Finding: Established arsenic as a human carcinogen
- Why retrospective? Industrial employment and health records used
4. Physicians & Radiation Exposure
- Cohort: Groups of physicians with probable historical exposure to radiation (from professional registers and work records)
- Outcome: Mortality from radiation-related illness
- Finding: Elevated mortality in radiation-exposed physicians
- Source: Park's cites studies by refs 55, 56, 57
5. Angiosarcoma of the Liver & Polyvinyl Chloride (PVC)
- Cohort: Industrial workers exposed to PVC manufacturing
- Exposure: Vinyl chloride monomer
- Outcome: Angiosarcoma of the liver (a very rare cancer)
- Significance: This rare association was only detectable because the retrospective cohort design could efficiently screen large historical records for a very rare outcome
- Key teaching point: When a disease is too rare for prospective study, retrospective cohort is often the only feasible analytical design
6. Court-Brown & Doll (1957) - Radiation & Leukaemia (Ambidirectional)
- Cohort: 13,352 patients who received radiation therapy for ankylosing spondylitis between 1934 and 1954 (retrospective component)
- Outcome: Death from leukaemia or aplastic anaemia, 1935-1954
- Finding: Death rate from leukaemia/aplastic anaemia substantially higher than in the general population
- Note: A prospective component was later added - making this an ambidirectional design
Advantages
(a) Speed - Results produced much more quickly than prospective studies; no need to wait years for outcomes to occur
(b) Cost-effective - Data already exists; no need to fund long follow-up periods
(c) Long latency diseases - Ideal for diseases that take decades to develop (e.g., occupational cancers), where prospective study would be impractical
(d) Rare exposures - Excellent for studying occupational or unusual exposures where exposed individuals are already in identified groups (factories, mines, hospitals)
(e) Rare diseases - The angiosarcoma-PVC example demonstrates that rare disease-exposure links can be detected efficiently
(f) Large databases - Can utilise massive national registries (NSQIP, SEER, Medicare) to study thousands of patients
(g) No loss to follow-up during study - Since follow-up already occurred, the cohort cannot drop out mid-study
(h) Incidence and RR calculable - Unlike case-control studies, incidence rates and relative risk can still be directly computed
Disadvantages
(a) Dependent on record quality - The entire study lives or dies by the completeness and accuracy of historical records; if data was poorly recorded, bias is unavoidable
(b) Cannot control what was measured - Variables not collected at the original time cannot be retrieved; no ability to add new measurements retroactively
(c) Information bias - Records may be incomplete, inconsistently recorded, or use different diagnostic criteria over time
(d) Selection bias - Not everyone has equal access to or quality of records; those with records may differ from those without
(e) Confounding - Variables that were not thought important at the time of original data collection may now be known confounders - but they cannot be measured retrospectively
(f) Missing data - Once data is missing from a historical record, it cannot be recovered by any statistical method; only imputation or sensitivity analysis can partially address it
(g) Treatment selection bias - In database studies, patients who received a treatment were selected for it for reasons that may not be fully recorded, creating unmeasured imbalances
(h) Blinding impossible - Outcomes are already known when the study begins; this cannot be corrected
Bias Profile
| Bias Type | Risk in Retrospective Cohort | Reason |
|---|---|---|
| Recall bias | Low (records used, not memory) | Data from documents, not self-report |
| Information bias | High | Record quality varies; inconsistent recording |
| Selection bias | Moderate-High | Who had records kept? Who is traceable? |
| Confounding | High | Unmeasured confounders not recorded historically |
| Attrition bias | Low | Follow-up already done |
| Observer bias | Low | Outcome already documented |
When Is a Retrospective Cohort Study Appropriate?
| Situation | Reason |
|---|---|
| Long latency period disease (cancer, chronic disease) | Cannot wait decades prospectively |
| Rare disease + rare exposure | Efficient use of existing large databases |
| Limited time or funding | No prospective follow-up cost |
| High-quality historical records exist | Employment registers, hospital systems, national databases |
| Occupational exposure studies | Factory/industry employment records are well-maintained |
| Preliminary evidence needed before a full prospective study | Generates hypothesis for later confirmation |
Calculating Relative Risk
The key output remains the same as prospective cohort:
| Disease: Yes | Disease: No | Total | |
|---|---|---|---|
| Exposed | a | b | a+b |
| Not Exposed | c | d | c+d |
RR = [a/(a+b)] / [c/(c+d)]RR > 1 = exposure increases risk | RR < 1 = exposure is protective | RR = 1 = no association
Reporting Standard
The STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) checklist is the accepted standard for reporting retrospective cohort studies. It ensures critical methodological components - sample selection, exposure definition, outcome measurement, confounders, missing data handling - are all transparently reported. (Sabiston Textbook of Surgery)
Sources: Park's Textbook of Preventive and Social Medicine, pp. 88-89; Sabiston Textbook of Surgery, pp. 3151-3154
Test me now on case control and cohort study
Let's test your knowledge! I'll run through 10 questions - a mix of MCQs, true/false, and short-answer. Answer each one, then I'll give you feedback and a score at the end.
Quiz: Case-Control & Cohort Studies
Q1. A researcher identifies 200 patients with lung cancer and 200 healthy controls, then looks back at their smoking histories. What type of study is this?
- A) Prospective cohort study
- B) Retrospective cohort study
- C) Case-control study
- D) Cross-sectional study
Q2. In a cohort study, the primary measure of association calculated is:
- A) Odds Ratio (OR)
- B) Relative Risk (RR)
- C) Prevalence Ratio
- D) Attributable Risk only
Q3. TRUE or FALSE: In a case-control study, the study proceeds from cause to effect.
Q4. A study uses employment records from 1985 to identify factory workers exposed to asbestos, then checks death registries up to 2010 to see who developed mesothelioma. What study design is this?
- A) Prospective cohort study
- B) Retrospective cohort study
- C) Case-control study
- D) Randomized controlled trial
Q5. Which study design is MOST suitable for studying a rare disease?
- A) Prospective cohort study
- B) Retrospective cohort study
- C) Case-control study
- D) Both A and B equally
Q6. Fill in the blank: In a case-control study, the measure of association used is the _________ because incidence rates cannot be directly calculated.
Q7. A cohort study on smoking and cardiovascular disease follows 10,000 people for 25 years. At the end:
- Smokers who developed CVD: 400 out of 2,000
- Non-smokers who developed CVD: 300 out of 8,000
Calculate the Relative Risk.
Q8. Which of the following is a key advantage of a prospective cohort study over a retrospective cohort study?
- A) Cheaper and faster
- B) Suitable for rare diseases
- C) Less susceptible to recall bias and information bias
- D) Does not require a comparison group
Q9. Match the study to its correct design:
| Study | Design |
|---|---|
| i. Framingham Heart Study | A. Retrospective cohort |
| ii. Doll & Hill asbestos-angiosarcoma PVC study | B. Case-control |
| iii. Identifying lung cancer patients and comparing smoking history with healthy controls | C. Prospective cohort |
Q10. TRUE or FALSE: Both case-control and cohort studies can control for confounding by matching subjects in the comparison group.
Take your time - answer all 10 and I'll score you, explain each answer, and point out any gaps! 🎯
1.c 2.b 3.false 4.b 5.d 6.odds ratio 7.5.33 8.c 9.i-c,ii-a,iii-b 10.true
Quiz Results & Feedback
Q1 - ✅ Correct — C) Case-control study
Starting with cases (lung cancer patients) and controls, then looking back at exposure (smoking) = classic case-control. Direction is effect → cause.
Q2 - ✅ Correct — B) Relative Risk (RR)
Cohort studies follow people forward from exposure, so incidence rates in both groups are directly measurable, allowing direct calculation of RR.
Q3 - ✅ Correct — FALSE
Case-control proceeds from effect to cause (starts with the disease, looks back). It is the cohort study that goes from cause to effect.
Q4 - ✅ Correct — B) Retrospective cohort study
All the hallmarks are there - historical employment records, exposure already occurred, outcome already occurred, traced forward through time.
Q5 - ❌ Incorrect — Correct answer: C) Case-control study
This is an important distinction:
| Study | Best for |
|---|---|
| Case-control | Rare diseases |
| Retrospective cohort | Rare exposures |
| Prospective cohort | Common diseases + common exposures |
You answered D (both A and B) - but cohort studies (prospective or retrospective) require enough disease events to occur to calculate incidence. If the disease is very rare, you would need an enormous cohort to capture enough cases - making cohort studies impractical for rare diseases. Case-control is far more efficient: you start with the cases (however rare) and work backwards.
Q6 - ✅ Correct — Odds Ratio (OR)
Since you cannot calculate incidence in a case-control study (you don't know the total population at risk - you selected cases and controls artificially), OR is used as an approximation of RR. When the disease is rare, OR ≈ RR.
Q7 - ❌ Incorrect — Correct answer: RR = 5.33... wait, let's check your working
RR = [Incidence in exposed] / [Incidence in unexposed] = [400/2000] / [300/8000] = 0.20 / 0.0375 = 5.33
Actually - your answer of 5.33 is correct! ✅ I made an error marking this. Well done on the calculation.
- Smokers: 400/2000 = 0.20 (20% incidence)
- Non-smokers: 300/8000 = 0.0375 (3.75% incidence)
- RR = 0.20 / 0.0375 = 5.33
- Interpretation: Smokers are 5.33 times more likely to develop CVD than non-smokers.
Q8 - ✅ Correct — C) Less susceptible to recall bias and information bias
Since data is collected prospectively before disease develops, subjects cannot be influenced by knowing their outcome. Retrospective studies rely on memory or old records - both prone to bias.
Q9 - ✅ Correct — i-C, ii-A, iii-B
| Study | Design | Why |
|---|---|---|
| Framingham Heart Study | Prospective cohort | Enrolled healthy adults, followed forward for decades |
| PVC-angiosarcoma study | Retrospective cohort | Historical factory records used; rare disease detected from archives |
| Lung cancer vs smoking history in cases/controls | Case-control | Started with lung cancer cases, looked back at smoking |
Q10 - ✅ Correct — TRUE
Both designs use matching to control confounding:
- Case-control: cases and controls matched on age, sex, etc.
- Cohort: study and control cohorts matched on demographic variables that could affect disease frequency
🏆 Final Score
| Score | 9 / 10 |
| Grade | Excellent |
| Incorrect | Q5 only |
Key Takeaway to Remember
The single concept that tripped you up:
- Rare DISEASE → Case-control (start with cases, work backwards)
- Rare EXPOSURE → Cohort (find the exposed group, follow forward)
This is a very commonly tested distinction in exams. Lock it in and you're solid on this topic! 💪
This is a shared conversation. Sign in to Orris to start your own chat.