Acute Pancreatitis
Reading File
Finding Sources
Searching PubMed
"acute pancreatitis"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Now I have comprehensive material from the textbooks. Let me compile the full response.
Acute Pancreatitis
Acute pancreatitis (AP) is an inflammatory condition leading to enzymatic autodigestion and destruction of pancreatic tissue. It ranges from mild, self-limited disease to sepsis and multiorgan failure. It is the most common pancreatic disease worldwide and one of the top reasons for gastrointestinal hospitalization in the United States, though overall mortality has decreased even as admissions have risen.
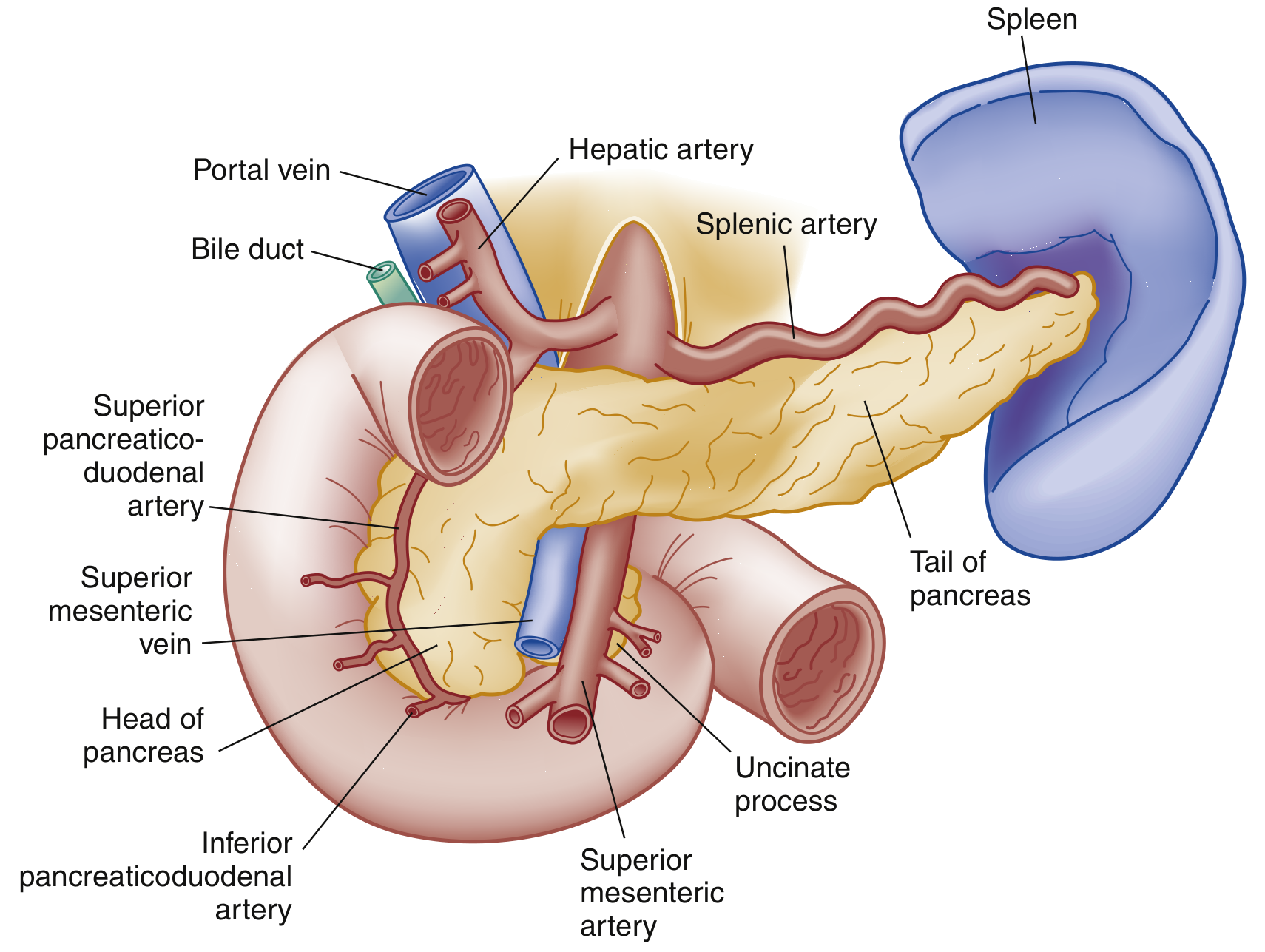
Anatomy
Etiology
The two most common causes are:
- Gallstones (40-70% of cases)
- Chronic alcohol use (25-35% of cases)
Other causes are organized by mechanism:
| Category | Examples |
|---|---|
| Toxic-Metabolic | Alcohol, drugs, hypertriglyceridemia (>1000 mg/dL), hypercalcemia, uremia, scorpion venom |
| Mechanical-Obstructive | Biliary stones, post-ERCP, pancreas divisum, annular pancreas, ampullary tumors, trauma |
| Infectious | Viral (mumps, coxsackievirus, HIV, CMV, EBV, varicella), bacterial (TB, Salmonella, Legionella, Mycoplasma), parasitic (Ascaris) |
| Vascular | Vasculitis, embolism, hypoperfusion/ischemia, hypercoagulability |
| Other | Idiopathic (many due to occult microlithiasis), hereditary, autoimmune, DKA |
Smoking and diabetes are independent risk factors. Many "idiopathic" cases harbor genetic mutations (SPINK1, CFTR combinations).
Pathophysiology
The central mechanism is premature intracellular activation of trypsinogen to trypsin within acinar cells, triggering a cascade of enzyme activation that causes autodigestion of the gland and surrounding tissue. This local injury triggers a systemic inflammatory response (SIRS) via release of cytokines and inflammatory mediators, which can cause:
- Increased microvascular permeability and third-spacing of fluid
- Pulmonary involvement (ARDS, pleural effusions - left-sided more common, atelectasis)
- Cardiovascular collapse (fluid shifts, shock)
- Renal failure (hypoperfusion + inflammatory mediators)
- Coagulopathy / DIC
- Hyperglycemia (reduced insulin secretion), hypocalcemia (low albumin/magnesium)
Classification (2012 Revised Atlanta Classification)
Morphological Types
| Type | Description |
|---|---|
| Interstitial Edematous Pancreatitis | Diffuse pancreatic enlargement with edema, no necrosis; resolves within 1st week in most (~90-95% of cases) |
| Necrotizing Pancreatitis | Involves parenchymal and/or peripancreatic necrosis; ~5-10% of cases; may be sterile or infected |
Severity Grades
| Grade | Organ Failure | Local/Systemic Complications | Mortality |
|---|---|---|---|
| Mild | Absent | Absent | Very rare (<5%) |
| Moderately Severe | Transient (<48 hours) | Present, without persistent organ failure | Low |
| Severe | Persistent (>48 hours) | Present | High (36-50%); extremely high with infected necrosis |
Severity should be reassessed at 24h, 48h, 7 days, and weekly thereafter.
Local Complications (Revised Atlanta Terminology)
Interstitial Edematous Pancreatitis:
- Acute Peripancreatic Fluid Collection (APFC) - homogeneous, non-encapsulated fluid collection adjacent to pancreas; <4 weeks from onset
- Pancreatic Pseudocyst - encapsulated fluid collection with well-defined wall, no necrosis; >4 weeks from onset
Necrotizing Pancreatitis:
- Acute Necrotic Collection (ANC) - heterogeneous fluid + necrosis, intrapancreatic and/or extrapancreatic
- Walled-Off Necrosis (WON) - heterogeneous fluid + necrosis with well-defined wall; >4 weeks from onset
Clinical Features
Symptoms:
- Persistent, moderate-to-severe epigastric or left upper quadrant pain radiating to the back, chest, or flanks
- Pain often worse in supine position; relieved by leaning forward
- Nausea, vomiting, anorexia
Signs:
- Fever, tachycardia, elevated respiratory rate
- Jaundice (suggests biliary obstruction)
- Shallow respirations from pain splinting; basilar crackles or reduced breath sounds (pleural effusion)
- Cullen sign - bluish periumbilical discoloration (hemoperitoneum)
- Grey Turner sign - reddish-brown flank discoloration (retroperitoneal bleeding)
- Both are late findings (sign of hemorrhagic pancreatitis)
- In severe cases: hypotension, signs of shock
Local structural complications (late): Bowel necrosis, splenic/portal vein thrombosis, GI bleeding, gastric outlet obstruction
Diagnosis
Diagnostic Criteria
Diagnosis requires 2 of 3 of the following:
- Abdominal pain strongly suggestive of acute pancreatitis
- Serum amylase and/or lipase ≥3× upper limit of normal
- Characteristic imaging findings
Laboratory Tests
| Test | Notes |
|---|---|
| Serum lipase | Preferred - more sensitive and specific than amylase; remains elevated ~1-2 weeks |
| Serum amylase | Less specific (also elevated in salivary disease, renal failure, appendicitis, cholecystitis, liver disease); elevated ~3-5 days; may be falsely negative in alcohol/hypertriglyceridemia-induced pancreatitis |
| ALT | >3× normal suggests biliary (gallstone) etiology (>150 U/L has ~95% PPV) |
| BUN, creatinine | Elevated BUN linked to worse outcomes; rising creatinine indicates renal failure |
| CBC | Leukocytosis common; elevated hematocrit (hemoconcentration) suggests necrosis |
| CRP | Most useful 24-48h after admission as severity marker |
| Procalcitonin | Predictor of severe AP and infected necrosis |
| Triglycerides, calcium | If metabolic etiology suspected |
| LFTs, bilirubin | Elevated suggest biliary obstruction |
Testing both amylase and lipase together does not improve sensitivity or specificity. Use lipase alone.
Imaging
Abdominal Ultrasound:
- First-line to evaluate for biliary/gallstone etiology
- Limited for direct pancreatic visualization (obscured by bowel gas)
- Can identify cholelithiasis, bile duct dilation; guides need for MRCP/EUS
CT (contrast-enhanced):
- NOT routine upfront; reserve for:
- Diagnostic uncertainty or atypical presentation
- Rule out other serious intra-abdominal pathology
- Assess complications in patients not improving after 48-72 hours
- Best performed 3-7 days after onset (necrosis evolves; early CT can miss it)
-
90% sensitivity and specificity
- Shows: parenchymal enlargement, loss of texture/borders, peripancreatic fat stranding, areas of non-enhancement (necrosis)
CT appearance of acute interstitial pancreatitis (arrows = peripancreatic fluid and fat stranding):
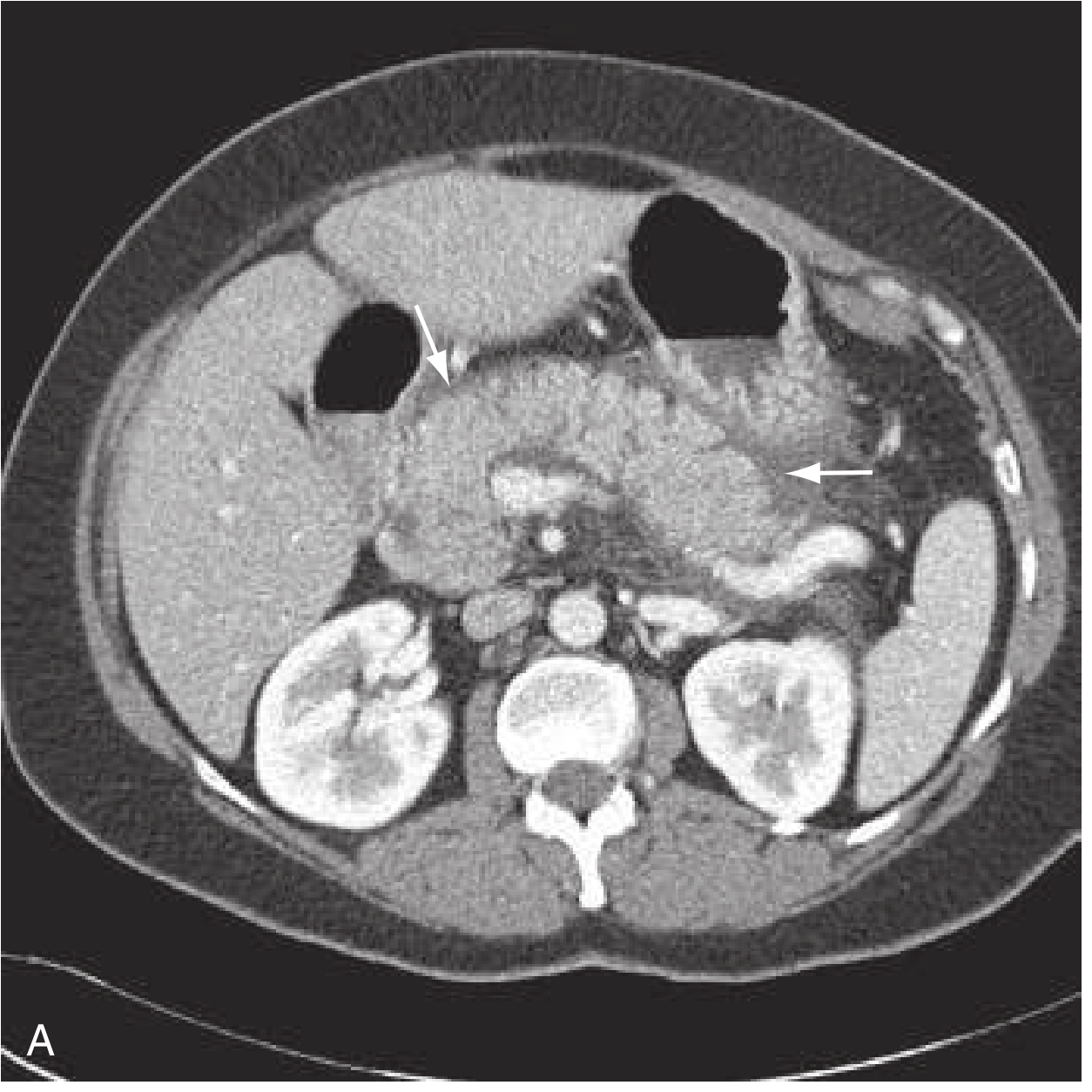 Rosen's Emergency Medicine, Fig. 77.2 - Axial view: swollen pancreas with peripancreatic fluid and fat stranding
Rosen's Emergency Medicine, Fig. 77.2 - Axial view: swollen pancreas with peripancreatic fluid and fat stranding
MRI/MRCP:
- Similar diagnostic utility to CT; superior for gallbladder and biliary tract
- Preferred when contrast is contraindicated
- MRI is more costly and less available
Chest X-ray if pulmonary complications are suspected. Plain abdominal films show only non-specific findings.
Severity Scoring Systems
| System | Key Features |
|---|---|
| Ranson's Criteria | 11 parameters assessed at admission (5) and at 48h (6); ≥3 = severe; complex, requires 48h wait |
| APACHE-II | Validated, can be calculated anytime; >8 = severe; complex |
| BISAP | 5 bedside factors (BUN >25, impaired mental status, SIRS, age >60, pleural effusion); ≥3 = high risk; calculable in ED |
| HAPS | 3 factors (no rebound/guarding, creatinine normal, hematocrit normal); if all normal = 97% specific for mild disease (not sensitive) |
| CT Severity Index (CTSI) | Based on degree of necrosis, inflammation, and fluid collections on CT; grades A-E |
| PASS | Dynamic continuous monitoring throughout illness; includes organ failure, SIRS, pain, medications, diet tolerance |
These scoring systems show similar predictive accuracy. Procalcitonin and CRP (at 24-48h) are useful additional severity markers.
Differential Diagnosis
Abdominal:
Peptic ulcer disease, gastritis, gastroenteritis, cholecystitis, choledocholithiasis, cholangitis, nephrolithiasis, bowel obstruction, perforated viscus, mesenteric ischemia, abdominal aortic aneurysm, ectopic pregnancy
Cardiopulmonary:
Myocardial infarction, pneumonia, pericarditis, pleural effusion
Systemic:
Sickle cell crisis, diabetic ketoacidosis
Management
General Principles
Treatment is mainly supportive. The pillars are: fluid resuscitation, analgesia, nutritional support, and treatment of the underlying cause.
1. Fluid Resuscitation
- Most critical in the first 24 hours
- Inadequate resuscitation → increased SIRS, organ failure, pancreatic necrosis, ICU admission
- Overly aggressive resuscitation → increased mechanical ventilation, abdominal compartment syndrome, earlier sepsis
- IAP/APA: Goal-directed 5-10 mL/kg/h targeting HR <120/min, MAP 65-85 mmHg, urine output >0.5-1 mL/kg/h
- ACG: 250-500 mL/h
- Preferred fluid: Lactated Ringer's (LR) over normal saline - LR may provide anti-inflammatory benefits; large volumes of NS cause hyperchloremic metabolic acidosis which activates trypsinogen and worsens inflammation
- Colloids not generally recommended; consider if Hct <24% or albumin <2 g/dL
- Monitor with Hct, BUN, creatinine
2. Pain Management
- IV opioids (e.g., morphine, hydromorphone) are acceptable
- Goal: adequate analgesia to allow normal respiratory effort
3. Nothing by Mouth (NPO) / Nutrition
- NPO initially; reinstate oral feeding as soon as tolerated (once pain subsides, nausea/vomiting resolves)
- Mild AP: Early oral feeding (within 24h) is safe and reduces hospital stay
- Severe/prolonged AP: Early enteral nutrition (via nasojejunal or nasogastric tube) is preferred over parenteral nutrition - reduces infectious complications, maintains gut barrier, decreases bacterial translocation
- Total parenteral nutrition (TPN) reserved for those who cannot tolerate enteral feeding
4. Antibiotics
- Not indicated for prophylaxis in sterile pancreatitis (even necrotizing)
- Indicated for documented infected pancreatic necrosis or other concurrent infection (e.g., cholangitis)
- Organisms: gram-negative predominate; increasing gram-positive organisms also seen
- Use broad-spectrum IV antimicrobials with good pancreatic tissue penetration (e.g., carbapenems, fluoroquinolones + metronidazole)
5. Biliary Pancreatitis / ERCP
- Abdominal ultrasound early for all patients to identify gallstones
- Urgent ERCP (within 24-72h) indicated if there is concurrent acute cholangitis or persistent biliary obstruction
- Not indicated for mild gallstone pancreatitis without cholangitis
- Cholecystectomy should be performed during the same admission or shortly after for gallstone pancreatitis (prevents recurrence)
6. Management of Local Complications
Pseudocysts:
- Most resolve spontaneously; intervention only if symptomatic (pain, obstruction, infection)
- Drainage options: endoscopic (EUS-guided cystgastrostomy), percutaneous, or surgical
Infected Pancreatic Necrosis ("Step-Up Approach"):
- Step 1: Broad-spectrum IV antibiotics
- Step 2: Percutaneous catheter drainage or endoscopic (transgastric/transduodenal) drainage
- Step 3: If no improvement → minimally invasive necrosectomy: VARD (video-assisted retroperitoneal debridement), MIRP, or endoscopic direct necrosectomy (DEN)
- Open necrosectomy reserved for failure of minimally invasive approaches; associated with substantial morbidity
- The PANTER trial demonstrated the step-up approach reduced major complications vs. open necrosectomy (12% vs. 50%) with similar mortality
7. ICU Care
- Continuous monitoring of organ function in severe AP
- Ventilatory support for ARDS
- Vasopressors for refractory shock
- Renal replacement therapy for acute kidney injury
Systemic Complications
| System | Complication |
|---|---|
| Pulmonary | ARDS, pleural effusion (up to 50%, left > right), atelectasis |
| Cardiovascular | Shock, decreased MAP |
| Renal | Acute kidney injury |
| Hematologic | DIC, thrombocytopenia |
| Metabolic | Hyperglycemia, hypocalcemia, hypoalbuminemia |
Prognosis & Disposition
- Mild AP: Most resolve within 3-7 days; low mortality (<5%); can often manage with supportive care
- Severe AP: Mortality 30-50%; extremely high with infected necrosis
- Persistent organ failure >48h is the strongest predictor of death
- Most patients require hospital admission; ICU for severe/complicated disease
- Reassess severity at 24h, 48h, 7 days, and weekly
Recurrence Prevention
- Gallstones: Cholecystectomy (same admission or early outpatient)
- Alcohol: Abstinence counseling and addiction support
- Hypertriglyceridemia: Lipid-lowering therapy (fibrates), dietary changes
- Medications: Identify and discontinue offending drug
- Idiopathic/Recurrent: Consider EUS, MRCP, genetic testing (SPINK1, CFTR, PRSS1 mutations)
Sources: Rosen's Emergency Medicine, 9th ed. | Sleisenger and Fordtran's Gastrointestinal and Liver Disease | Current Surgical Therapy, 14th ed. | Mulholland & Greenfield's Surgery, 7th ed. | Grainger & Allison's Diagnostic Radiology
This is a shared conversation. Sign in to Orris to start your own chat.