Can you tell me common ecg to learn about it with images and which help full fir icu to diagnose the disease which are helpful
Reading File
Finding Sources
Finding Sources
Searching the Web
common ECG patterns ICU diagnosis with images 2024
Finding Sources
Finding Sources
Reading Web Page
https://litfl.com/killer-ecg-patterns-part-1
Reading File
Finding Sources
Finding Sources
Loading Image
Loading Image
Finding Sources
Finding Sources
Searching the Web
STEMI ECG pattern image site:litfl.com OR site:ecg-library.com
Searching the Web
ECG patterns ICU critical care atrial fibrillation ventricular tachycardia pulmonary embolism complete heart block images
Loading Image
Loading Image
Loading Image
Loading Image
Now I have excellent visual material and textbook content. Let me compile a comprehensive, well-illustrated guide.
Common ECG Patterns for the ICU - A Visual Guide
Understanding ECGs is one of the most important skills in the ICU. Below is a structured guide covering the patterns you must recognise, with images and clinical context.
The ECG Basics - What Each Wave Represents

| Wave/Interval | What it represents |
|---|---|
| P wave | Atrial depolarization (SA node firing) |
| PR interval | Conduction delay at the AV node (normal 120-200 ms) |
| QRS complex | Ventricular depolarization (normal <120 ms) |
| ST segment | Early ventricular repolarization - KEY for ischemia |
| T wave | Ventricular repolarization |
| QT interval | Total ventricular electrical activity (normal <440 ms men, <460 ms women) |
- Miller's Anesthesia, 10e
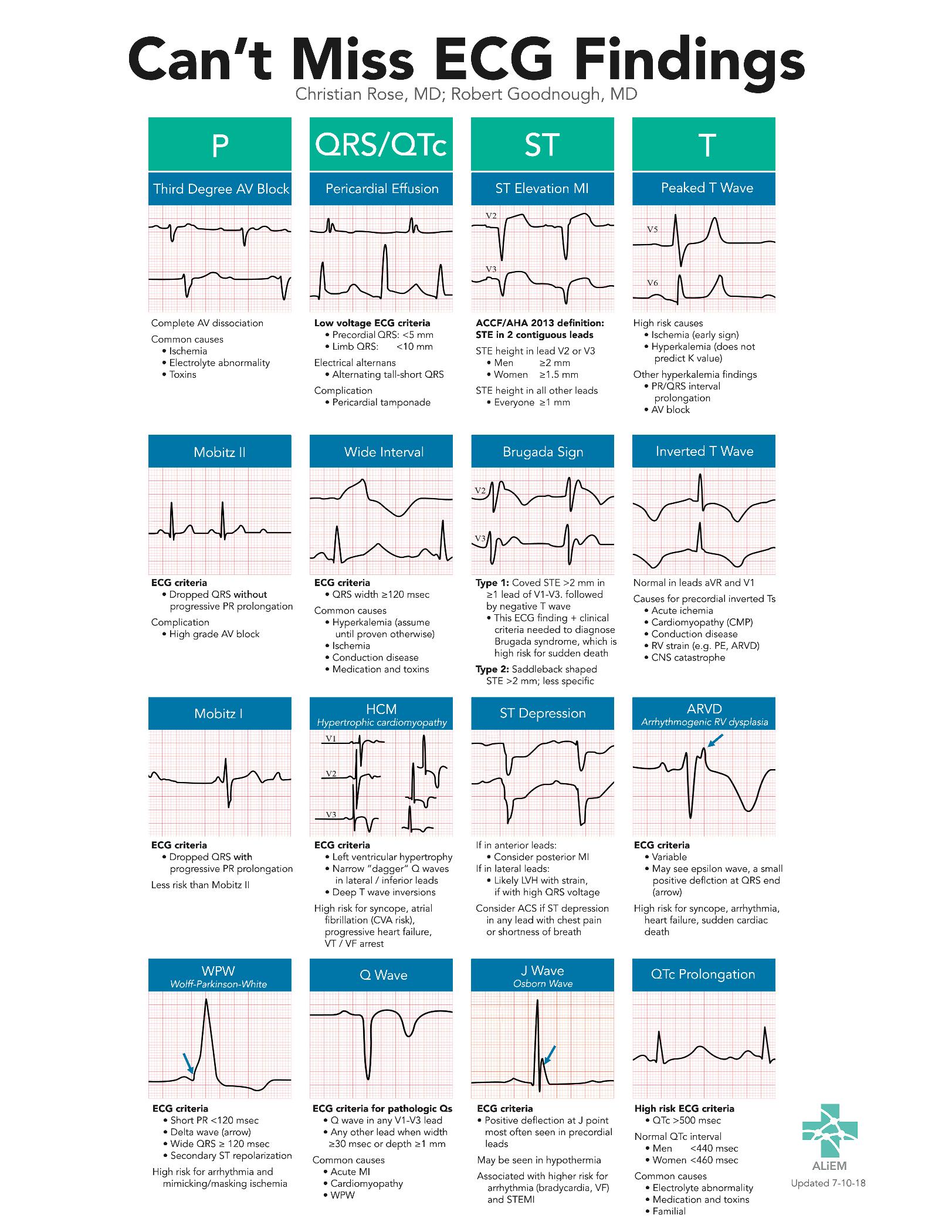
"Can't Miss" ECG Findings - The Master Reference
This chart from the LITFL / ALiEM library summarizes the most critical patterns organized by ECG component:
1. STEMI - ST-Elevation Myocardial Infarction
Why it matters in ICU: Most common time-critical diagnosis. Every minute of delay = more myocardium lost.
ECG criteria (ACC/AHA):
- ST elevation at J point in ≥2 contiguous leads
- Men: ≥2 mm in V2-V3, ≥1 mm elsewhere
- Women: ≥1.5 mm in V2-V3
Territory localization:
| Leads with ST elevation | Territory | Artery |
|---|---|---|
| V1-V4 | Anterior | LAD |
| II, III, aVF | Inferior | RCA (80%) or LCx |
| I, aVL, V5-V6 | Lateral | LCx or diagonal |
| V1-V2 (ST depression) | Posterior | RCA / LCx |
Reciprocal changes (mirror-image ST depression) are strong confirmatory signs, especially in inferior STEMI where aVL shows reciprocal depression.
STEMI equivalents you must also know:
- Wellens syndrome - Biphasic or deeply inverted T waves in V2-V3 = critical LAD stenosis, even when pain-free
- De Winter pattern - Upsloping ST depression + tall T waves in V1-V6 = LAD occlusion without classic STE
- Posterior STEMI - ST depression in V1-V3 (look for R>S in V1-V2) - do posterior leads (V7-V9)
- Left main / proximal LAD - ST elevation in aVR + diffuse ST depression
2. Common Heart Rhythms and Blocks

Atrial Fibrillation (AF)
- ECG features: Absent P waves, irregularly irregular RR intervals, fibrillatory baseline
- ICU significance: Most common sustained arrhythmia. Causes in ICU: sepsis, hypoxia, electrolyte imbalance, post-cardiac surgery, thyroid storm
- Requires rate control (beta-blockers, diltiazem) and anticoagulation assessment
Atrial Flutter
- ECG features: Sawtooth flutter waves at 300 bpm, regular ventricular response at 2:1 or 3:1 ratio (~150 bpm at 2:1)
- Tip: Rate of exactly 150 bpm should always make you suspect flutter with 2:1 block
AV Heart Blocks
| Type | ECG finding | Clinical action |
|---|---|---|
| 1st degree | PR >200 ms, every P conducts | Usually benign, monitor |
| 2nd degree Mobitz I (Wenckebach) | Progressive PR lengthening, then dropped QRS | Usually benign, may see in inferior MI |
| 2nd degree Mobitz II | Constant PR, sudden dropped QRS - no warning | High risk - pacing often needed |
| 3rd degree (Complete) | Complete AV dissociation - P and QRS independent | Emergency - transcutaneous pacing |
Ventricular Tachycardia (VT)
- ECG: Wide QRS (>120 ms), rate >100 bpm, AV dissociation, fusion/capture beats
- ICU significance: Life-threatening. Pulseless VT = defibrillation. Stable VT = amiodarone, cardioversion
- Torsades de Pointes = polymorphic VT twisting around the axis, associated with long QT
Ventricular Fibrillation (VF)
- ECG: Chaotic, irregular waveforms, no organized QRS
- Action: Immediate defibrillation + CPR
3. Hyperkalemia - The "Silent Killer" in ICU
Hyperkalemia is extremely common in the ICU (renal failure, rhabdomyolysis, acidosis) and produces progressive ECG changes.
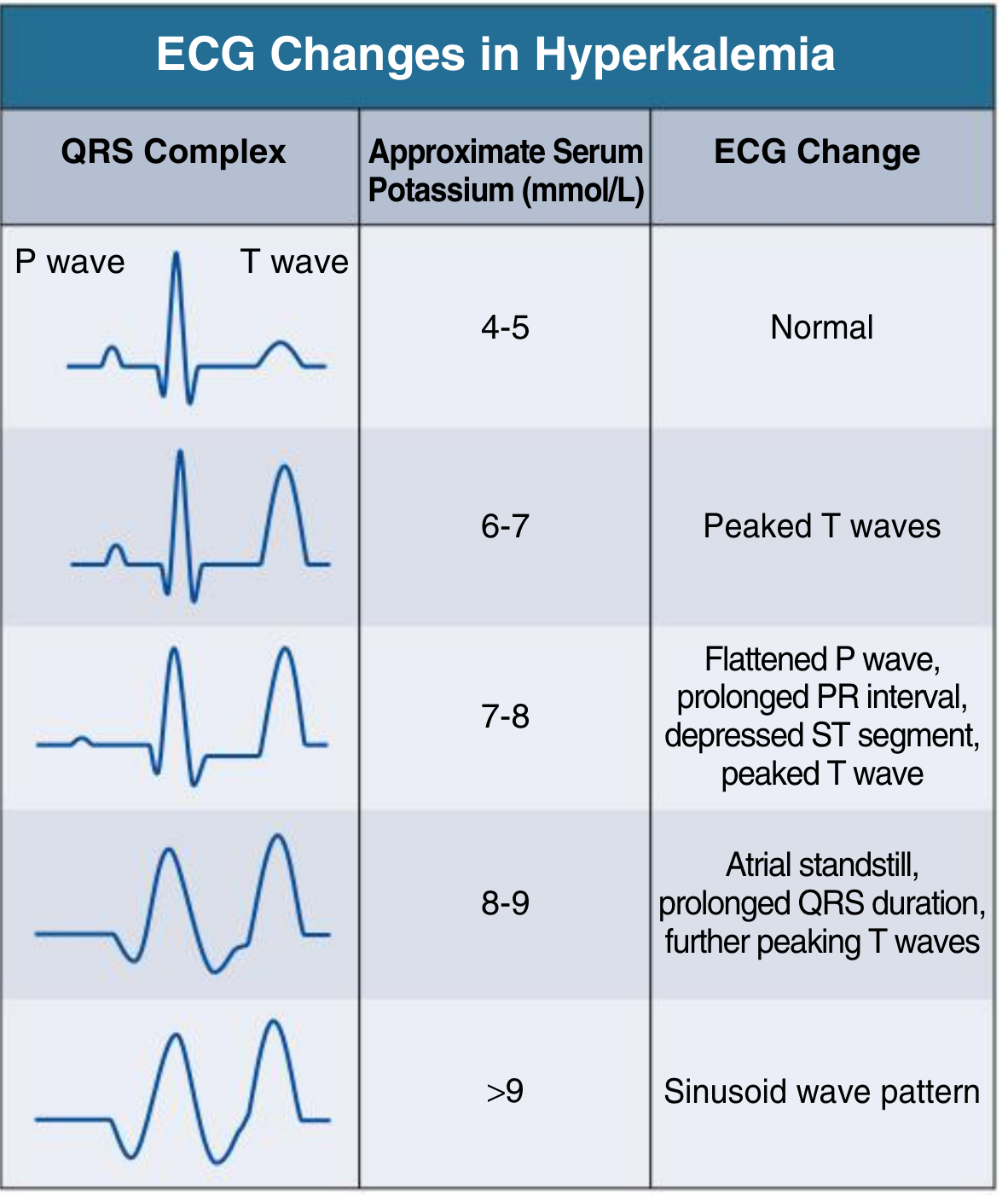
Progressive stages (Comprehensive Clinical Nephrology, 7e):
| K+ level (mmol/L) | ECG change |
|---|---|
| 4-5 | Normal |
| 6-7 | Peaked (tented) T waves - narrow, tall, symmetric |
| 7-8 | Flattened P waves, prolonged PR, depressed ST, peaked T |
| 8-9 | Atrial standstill, widened QRS |
| >9 | Sinusoidal (sine wave) pattern → VF |
Treatment: Calcium gluconate (membrane stabilization), insulin + dextrose, sodium bicarbonate, dialysis.
Hypokalemia ECG: U waves, flattened T waves, ST depression, prolonged QT - predisposes to arrhythmia especially with digoxin.
4. Killer Patterns - The LITFL "Danger ECGs"
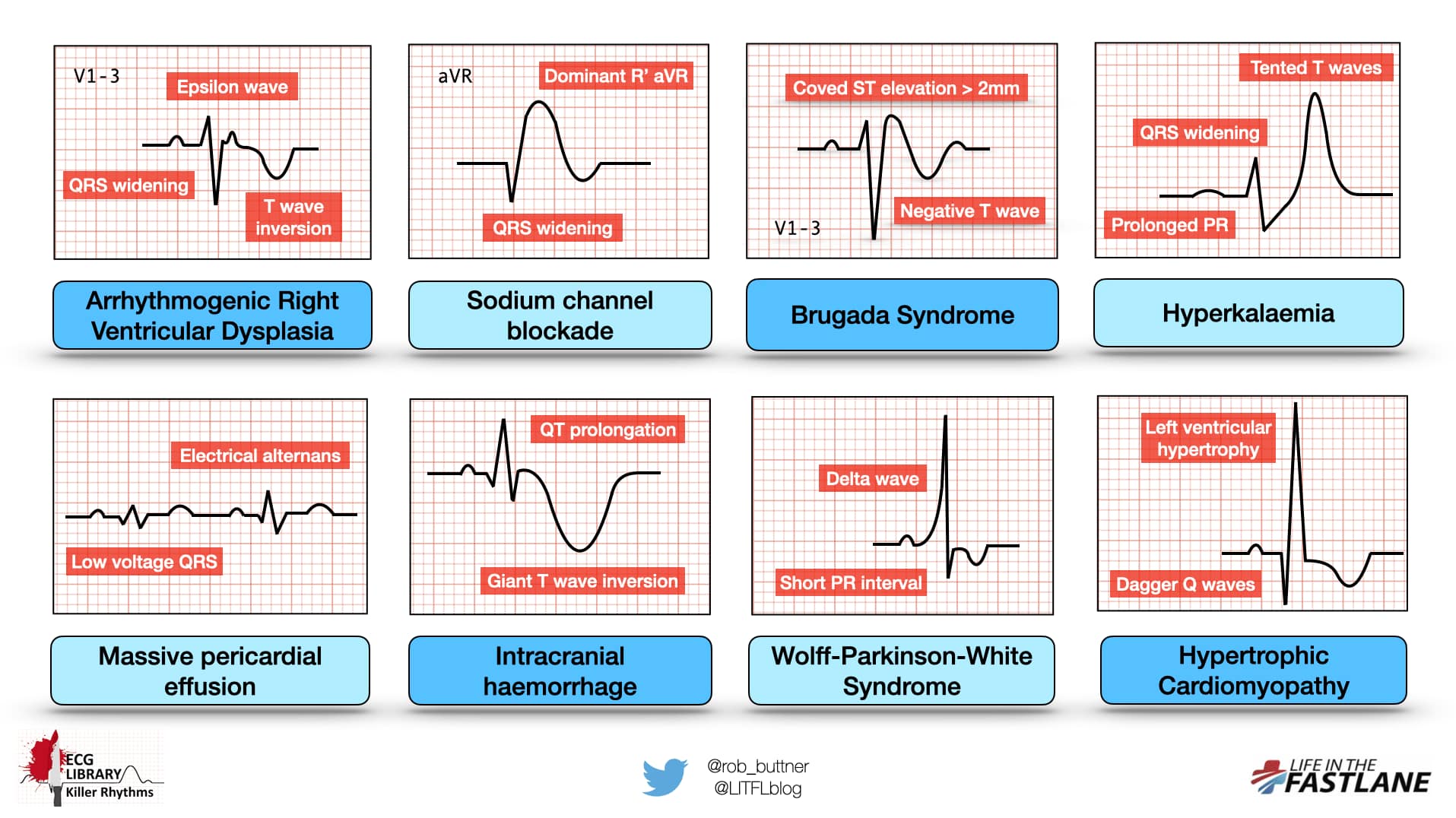
Brugada Syndrome
- Type 1 (diagnostic): Coved ST elevation >2 mm in V1-V3 followed by negative T wave
- ICU trigger: Fever can unmask Brugada pattern - common in febrile ICU patients
- Risk of sudden VF - ICD indication
Massive Pericardial Effusion / Cardiac Tamponade
- ECG: Low voltage QRS (<5 mm in limb leads, <10 mm precordial) + electrical alternans (alternating tall/short QRS) = classic sign of tamponade
- Action: Urgent echo + pericardiocentesis
Wolff-Parkinson-White (WPW)
- ECG: Short PR (<120 ms) + delta wave (slurred QRS upstroke) + wide QRS
- ICU danger: If AF develops in WPW, do NOT give AV nodal blockers (adenosine, digoxin, verapamil) - can cause VF via rapid conduction down the accessory pathway
Intracranial Hemorrhage / Raised ICP
- ECG: Giant diffuse T-wave inversions ("cerebral T waves"), QT prolongation
- Seen in subarachnoid hemorrhage especially
- Do NOT confuse with ischemia - look at clinical context
Sodium Channel Blockade Toxicity (TCA overdose)
- ECG: Broad QRS + dominant R' wave in aVR
- Treatment: Sodium bicarbonate IV
Arrhythmogenic Right Ventricular Dysplasia (ARVD)
- ECG: Epsilon wave (small deflection after QRS in V1-V3), T-wave inversion V1-V3, QRS widening
- Cause of sudden death in young athletes
5. Pulmonary Embolism (PE)
- Classic (but uncommon) S1Q3T3 pattern: S wave in lead I, Q wave and inverted T in lead III
- More common ECG findings in PE:
- Sinus tachycardia (most common)
- Right heart strain: T-wave inversion in V1-V4
- New right bundle branch block (RBBB)
- Right axis deviation
- P pulmonale (peaked P in II)
- ECG alone cannot rule in or rule out PE - use Wells score + CT-PA
6. Pericarditis
- ECG: Diffuse concave ("saddle-shaped") ST elevation in most leads (except aVR, V1 where it is depressed)
- PR depression in multiple leads - pathognomonic
- Differentiate from STEMI: pericarditis has diffuse leads, no reciprocal changes, no Q waves
Quick ICU ECG Checklist (Systematic Approach)
When you pick up an ICU ECG, read it in this order:
- Rate - bradycardia (<60) or tachycardia (>100)?
- Rhythm - regular or irregular? P waves present?
- PR interval - <120 ms (WPW/pre-excitation) or >200 ms (heart block)?
- QRS width - >120 ms = LBBB / RBBB / VT / hyperkalemia / toxin
- QT interval - prolonged? (risk of torsades)
- ST segments - elevation (STEMI / pericarditis) or depression (ischemia / posterior MI)?
- T waves - peaked (hyperkalemia), inverted (ischemia, PE, ARVD, raised ICP)?
- Voltage - low (effusion / tamponade, COPD, obesity)?
Most Useful ECG Resources for ICU Learners
- LITFL ECG Library - the best free ECG image bank online
- EMCrit ECG Guide - critical care focused, systematic approach
- REBEL EM - Five ECG Patterns You Must Know - quick summary of STEMI equivalents
- Goldman-Cecil Medicine, 26e - comprehensive STEMI/NSTEMI ECG sections
- Tintinalli's Emergency Medicine - excellent arrhythmia and Brugada coverage
- Miller's Anesthesia, 10e - perioperative ECG and cardiac physiology
This is a shared conversation. Sign in to Orris to start your own chat.