Carpal Tunnel syndrome definition eloborate signs symptoms investigation treatment options comparison between minimally invasive versus endoscopic and procedure for endoscopic and steps everything in detail with appropriate images and illustration
"carpal tunnel syndrome" AND "endoscopic" AND "open release"
"carpal tunnel syndrome" AND surgery AND outcomes
carpal tunnel syndrome anatomy median nerve transverse carpal ligament
endoscopic carpal tunnel release procedure technique
"carpal tunnel" AND "endoscopic release" AND "open release"
Phalen test Tinel sign carpal tunnel clinical examination
carpal tunnel syndrome nerve conduction EMG electrophysiology
"endoscopic" AND "open" AND "carpal tunnel release" AND comparison
PMID: 40473869
PMID: 35255490
Carpal Tunnel Syndrome (CTS) — Comprehensive Clinical Guide
1. Definition
"Carpal tunnel syndrome is the most common nerve entrapment syndrome encountered in primary care" — Textbook of Family Medicine 9e
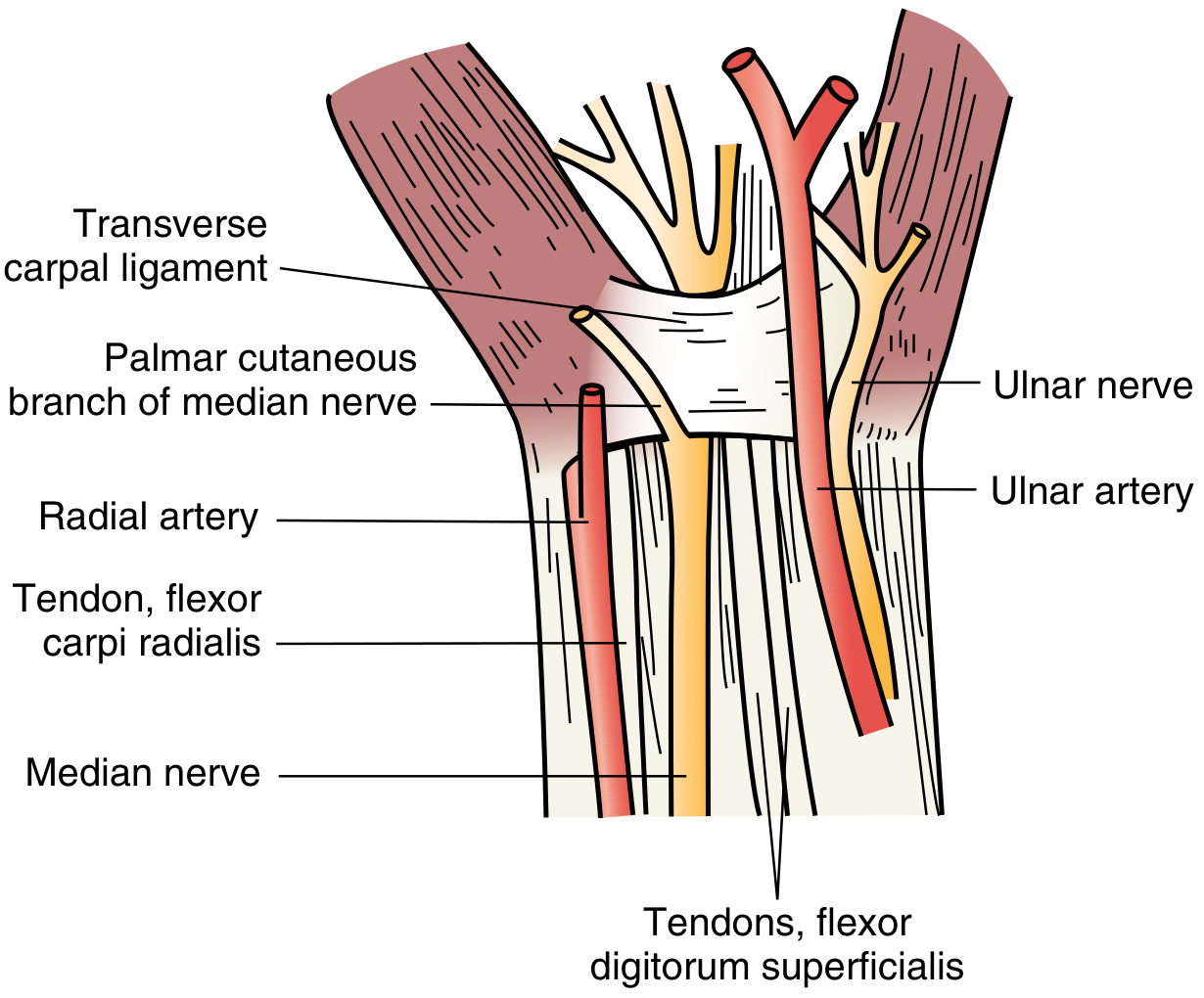
2. Anatomy of the Carpal Tunnel
| Boundary | Structure |
|---|---|
| Radial wall | Scaphoid bone (tubercle) |
| Ulnar wall | Hook of hamate, pisiform |
| Dorsal floor | Carpal bones (lunate, capitate) |
| Volar roof (ceiling) | Transverse carpal ligament (flexor retinaculum) |
- Median nerve — relatively superficial and radial
- Flexor pollicis longus (FPL) tendon × 1
- Flexor digitorum superficialis (FDS) tendons × 4
- Flexor digitorum profundus (FDP) tendons × 4
3. Epidemiology & Risk Factors
- Prevalence: ~53 per 10,000 working adults
- More common in women and during pregnancy
- Accepted occupational hazard with repetitive wrist/hand activity
| Category | Examples |
|---|---|
| Mechanical/Occupational | Repetitive wrist flexion/extension, vibrating tools, keyboard work |
| Metabolic | Diabetes mellitus, hypothyroidism (myxedema), pregnancy (fluid retention), acromegaly, amyloidosis |
| Inflammatory | Rheumatoid arthritis (synovial thickening), sarcoidosis |
| Structural | Carpal dislocations, distal radius malunion, ganglion cysts, lipomas, anomalous muscles |
| Developmental | Anomalous muscles within the tunnel |
4. Pathophysiology
- Elevated tunnel pressure → venous congestion → epineural edema
- Chronic ischemia → segmental demyelination → slowed conduction velocity
- Prolonged compression → Wallerian degeneration and axonal death → denervation of thenar muscles
5. Clinical Features
5a. Symptoms
- Paresthesias (tingling, numbness, "pins and needles") in the thumb, index, and middle fingers, and the radial half of the ring finger (median nerve distribution)
- Symptoms worse at night (nocturnal awakening is classic — flexed wrist posture during sleep raises tunnel pressure)
- Worsened by: prolonged activity, driving, holding a phone/book, using a hair dryer
- "Flick sign": patient shakes/flicks the wrist to relieve symptoms
- Subjective numbness may extend into the ulnar digits and proximally to the shoulder ("brachialgia")
- Clumsiness, tendency to drop objects
- Difficulty with fine motor tasks: buttons, coins, jewelry clasps
- Thenar atrophy (abductor pollicis brevis, opponens pollicis) — a late, serious finding
- Weakness of thumb opposition and abduction
Key diagnostic point: The thenar eminence skin is NOT numb (palmar cutaneous branch exits proximal to the tunnel). If the thenar skin is numb, consider a more proximal median nerve lesion.
5b. Physical Signs
| Sign | Technique | Positive Result | Sensitivity/Specificity |
|---|---|---|---|
| Tinel's Sign | Percuss/tap over the median nerve at the wrist crease | Paresthesia radiates into the median nerve distribution | Moderate (~60%); high interexaminer variability |
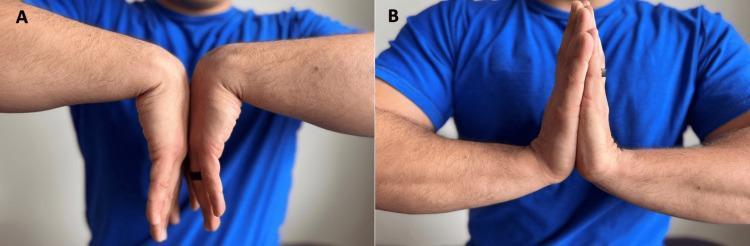
| Phalen's Test | Wrist in complete flexion for 60 seconds | Reproduction of numbness/tingling in median distribution | Sensitivity ~74%, false-positive ~25% |
| Reverse Phalen's (Prayer Test) | Wrists in maximum extension, palms together for 60 seconds | Paresthesia in median distribution | Additive to Phalen's |
| Durkan's Sign (Carpal Compression Test) | Direct pressure over the carpal tunnel for 30 seconds | Paresthesia reproduced — highest sensitivity among provocative tests | Sensitivity ~87% |
| Thenar Wasting | Inspection of thenar eminence | Muscle atrophy | Indicates chronic/severe disease |
| 2-Point Discrimination | Static 2-point discrimination on fingertips | Widened (>6 mm) | Indicates significant sensory fiber loss |
6. Investigations
6a. Nerve Conduction Studies (NCS) — Gold Standard
- Prolonged distal sensory latency (most sensitive early finding; >3.5 ms over 14 cm)
- Prolonged distal motor latency to abductor pollicis brevis (>4.2 ms)
- Reduced sensory nerve action potential (SNAP) amplitude in severe cases
6b. Electromyography (EMG)
- Polyphasic reinnervation potentials in abductor pollicis brevis (APB)
- Fibrillation potentials = active denervation (severe/chronic disease)
- Normal EMG does not exclude CTS if NCS is abnormal
6c. Ultrasound
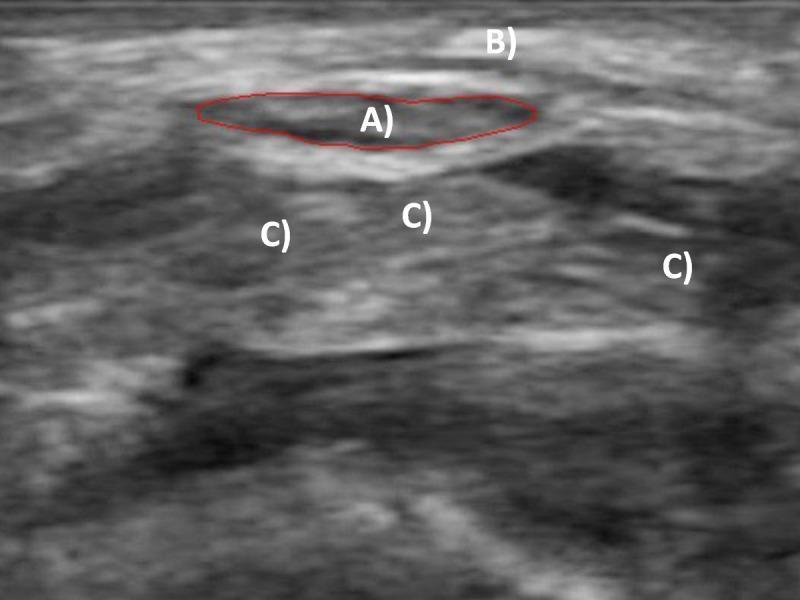
- Median nerve cross-sectional area (CSA) ≥ 10 mm² at the tunnel inlet = diagnostic threshold for CTS
- Shows nerve swelling, flattening, and increased vascularity (power Doppler)
- Useful when NCS is inconclusive or unavailable
- Can identify structural causes (ganglion, anomalous muscle)
6d. MRI
- Not routinely required
- Used in atypical cases or when structural lesion (e.g., tumor, amyloid deposition, post-traumatic) is suspected
- Shows nerve signal changes and any compressive mass
6e. Blood Tests (Screen for systemic causes)
- Fasting glucose / HbA1c — diabetes
- TSH — hypothyroidism
- Rheumatoid factor / ANA — inflammatory arthritis
- Serum calcium, ACE — sarcoidosis
- IGF-1 — acromegaly
- Serum/urine protein electrophoresis — amyloidosis (in elderly)
6f. Plain Radiographs
- When bony cause suspected (old fracture, carpal malalignment, arthritis)
7. Severity Classification
| Grade | Features |
|---|---|
| Mild | Intermittent paresthesias, symptoms only with provocation, normal EMG |
| Moderate | Frequent/persistent paresthesias, nocturnal symptoms, abnormal sensory NCS |
| Severe | Constant numbness, thenar weakness/wasting, abnormal motor NCS, denervation on EMG |
8. Treatment
8a. Conservative (Non-Surgical) Treatment
- Neutral wrist splint (0–20° extension) worn at nighttime (avoids the flexed posture during sleep)
- Can provide years of symptom relief in mild cases
- Daytime wear for those with activity-related symptoms
- Injected into (not into) the carpal tunnel, ulnar to the palmaris longus tendon
- Methylprednisolone 40 mg ± local anaesthetic
- Provides temporary but often significant relief (weeks to months)
- Strong correlation: patients who respond to injection respond well to surgical release
- Local anaesthetic relief immediately confirms correct placement (anesthesia in median distribution)
- Repeat injections are possible; typically limited to 2–3
- Ergonomic assessment and modification of repetitive tasks
- Avoidance of sustained wrist flexion/extension
- Tendon and nerve gliding exercises (mobilize nerve within tunnel)
- Yoga, manual therapy — systematic reviews show modest short-term benefit for pain and function
- Ultrasound therapy, laser — limited evidence
- NSAIDs: modest short-term analgesia
- Oral corticosteroids: short course can provide temporary relief
- Vitamin B6: not established
- Emerging technique; some RCT data showing benefit for perineural hydrodissection
8b. Surgical Treatment — Indications
- Conservative treatment has failed or symptoms persist > 3–6 months
- Initial presentation with severe CTS (thenar atrophy, constant numbness, denervation on EMG)
- Progressive neurological deficit
- Confirmed electrophysiological evidence of nerve damage
9. Surgical Techniques: Open vs. Endoscopic vs. Minimally Invasive
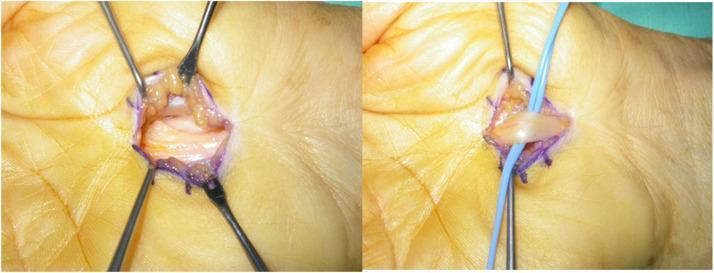
9a. Open Carpal Tunnel Release (OCTR)
- Regional or local anaesthesia (wrist/digital block), tourniquet applied
- Longitudinal incision in the palm — in line with the ring finger pad touching the proximal palm in flexion (avoids the palmar cutaneous branch of the median nerve)
- Incision extends from the wrist crease to 3–4 cm in the palm
- Palmar fascia divided
- Carpal tunnel contents visualized as they exit distally
- Transverse carpal ligament divided longitudinally under direct vision, with median nerve visible and protected at all times
- Wound closed; hand elevated
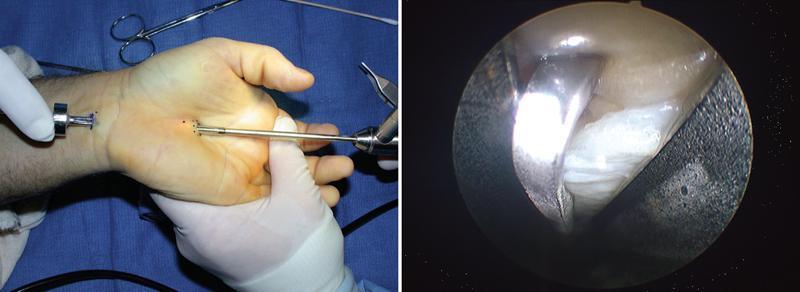
9b. Endoscopic Carpal Tunnel Release (ECTR)

Two Main Endoscopic Techniques:
| Chow Technique (Two-Portal) | Agee Technique (Single-Portal) | |
|---|---|---|
| Portals | Proximal (wrist crease) + distal (palm) | Proximal only (wrist crease) |
| Direction of cut | Retrograde (distal to proximal) | Antegrade (proximal to distal) |
| Visualization | Enters from proximal, views through scope toward palm | Blade and scope in same assembly |
| Instrument | Rigid endoscope + separate cutting blade | Proprietary single-assembly device (Agee device) |
| Advantage | Two-portal visualization confirms complete release | Single small incision, faster setup |
10. Detailed Step-by-Step Procedure: Endoscopic Carpal Tunnel Release (Chow Two-Portal Technique)
Pre-operative Preparation
- Consent: discuss risks including median nerve injury, incomplete release, conversion to open
- Anaesthesia: local infiltration + wrist block or IV regional (Bier block); tourniquet applied at forearm/upper arm
- Positioning: patient supine, forearm supinated on hand table
- Equipment: rigid endoscope (2.7–4 mm), camera system, specialized slotted cannula system, reverse-cutting blade
Step-by-Step Procedure
- Mark the proximal wrist crease (site of proximal portal)
- Mark the axis of the ring finger extended to the wrist — this corresponds to the ulnar edge of the median nerve and is the safe zone for the distal portal
- Mark the hook of hamate (palpated as a bony prominence in the palm)
- A 1.5–2 cm transverse incision is made at or just proximal to the wrist crease, between the flexor carpi ulnaris and palmaris longus tendons
- Blunt dissection to the level of the flexor retinaculum, protecting the palmar cutaneous branch of the median nerve (which lies radially)
- A trocar and slotted cannula (synovial elevator) are inserted into the carpal tunnel just beneath the transverse carpal ligament (subligamentous space)
- The instrument is directed distally toward the palm, staying in the subsynovial plane (superficial to the flexor tendons, deep to the ligament)
- The trocar is exchanged for the endoscope
- The endoscope light transilluminates through the palm — the surgeon confirms the instrument tip location by visualizing the light through the skin
- The surgeon palpates the palm to identify the distal portal site — typically at the level of the fully abducted ring finger, just distal to the distal edge of the ligament
- A 1 cm transverse incision is made at the distal portal site in the palm
- A probe/trocar exits through this portal, converting to a two-portal system with the cannula spanning the carpal tunnel
- The rigid endoscope is inserted through the proximal portal
- The transverse carpal ligament is visualized as a dense, white, fibrous band on the underside of the cannula's viewing slot
- The median nerve and ulnar neurovascular bundle are identified and confirmed to be safely lateral to the cannula — critical safety check before cutting
- A reverse-cutting hook blade is introduced through the distal portal
- The ligament is incised under direct endoscopic vision, progressing from distal to proximal (retrograde cut)
- The cut is completed in segments, confirming fiber-by-fiber division
- Release is confirmed when the white fibrous ligament fibers are fully separated and the surrounding palmar fat is visible — indicating complete decompression
- The endoscope is advanced to confirm no residual intact ligament fibers remain
- The tourniquet is deflated; haemostasis confirmed
- Both portal sites are irrigated
- Both portal incisions are closed with 1–2 absorbable sutures
- Bulky soft dressing applied (no cast)
- Immediate finger movement encouraged
Post-operative Care
- Elevation of the hand for 24–48 hours
- Immediate active finger exercises to prevent stiffness
- Light use of the hand within days; return to desk work within 1–2 weeks
- Full return to manual labour: typically 2–4 weeks (versus 4–8 weeks for OCTR)
- Formal hand therapy if thenar weakness is present pre-operatively
11. Minimally Invasive vs. Endoscopic vs. Open: Detailed Comparison
11a. Open vs. Endoscopic — Head-to-Head Summary
| Parameter | Open CTR (OCTR) | Endoscopic CTR (ECTR) |
|---|---|---|
| Incision size | 3–5 cm palmar | 1–2 small portals (wrist ± palm) |
| Direct nerve visualization | ✅ Full exposure throughout | ⚠️ Indirect (endoscopic view) |
| Completeness of release | Very high | High (in experienced hands) |
| Learning curve | Low (accessible to all hand surgeons) | Steep — not for the occasional CTR surgeon |
| Symptom relief at 3 months | Excellent | Equally excellent or superior |
| Long-term outcomes | Equivalent | Equivalent |
| Postoperative pain | More; pillar pain common | Less intense, shorter duration |
| Return to work | 4–8 weeks | 1–3 weeks (key advantage) |
| Scar/pillar tenderness | More frequent | Less frequent |
| Risk of nerve injury | Lower | ⚠️ Slightly higher transient nerve injury risk (in inexperienced hands) |
| Risk of incomplete release | Very low | Slightly higher in early learning curve |
| Wound complications | Occasional | Less (smaller incision) |
| Direct cost | Lower | Higher (equipment) |
| Ability to address additional pathology | ✅ Yes | ❌ Limited |
| Anaesthesia requirement | Local/regional | Local/regional |
11b. Minimally Invasive Techniques (Beyond Standard ECTR)
- Emerging technique gaining rapid popularity
- Ultrasound provides real-time visualization of the median nerve without portals or endoscope
- Hook knife or specialized blade is inserted through a single small incision and guided by ultrasound to divide the ligament under continuous nerve visualization
- Advantages: real-time nerve visualization, no endoscopic equipment, can be performed in office/clinic setting
- Evidence (2025 Network Meta-Analysis, PMID 40473869): CTR-US showed highest patient satisfaction (OR = 6.89; 95% CI: 1.87–25.43) and shortest return-to-work duration among all techniques evaluated
- A modified approach dividing the carpal ligament through two separate tunnel passages
- Lowest risk of adverse events per the 2025 NMA (OR = 0.05; 95% CI: 0.01–0.42)
- Less widely adopted
- Blind percutaneous techniques exist but carry higher risk of median nerve injury when not ultrasound-guided
- Not recommended without image guidance
11c. Evidence Summary (Network Meta-Analysis 2025 — 32 RCTs, 2,916 patients)
One-port and two-port ECTR demonstrated superior symptom relief vs. conventional open CTR at 3 months (two-port ECTR: SMD = −4.47; 95% CI: −5.67 to −3.26). One-port ECTR showed better grip (SMD = 1.37) and pinch strength. Ultrasound-guided CTR had the highest patient satisfaction. The double-tunnel technique had the fewest complications. Long-term outcomes were equivalent across all techniques.
"ECTR is equally effective as open CTR for alleviating symptoms with no differences in long-term outcomes. ECTR has increased risk of transient nerve injury; open CTR has increased risk of wound/scar complications. ECTR has higher direct costs but earlier return to work."
Surgical treatment is superior to non-surgical treatment for symptom relief in CTS, with better long-term outcomes.
12. Complications of Surgical Release
| Complication | Open | Endoscopic |
|---|---|---|
| Incomplete release / symptom recurrence | Rare | Slightly higher in inexperienced hands |
| Median nerve injury (transient neurapraxia) | Lower | Higher (key concern with ECTR) |
| Palmar cutaneous nerve injury | Possible | Less common |
| Superficial palmar arch injury | Rare | Rare |
| Pillar pain (scar tenderness) | Common (6–12 months) | Less common |
| Bowstringing of flexor tendons | If incision too proximal | Very rare |
| Wound infection | Occasional | Less common |
| Complex Regional Pain Syndrome | Rare | Rare |
13. Special Situations
- Pregnancy-associated CTS: conservative (splinting) first; usually resolves postpartum. Surgery rarely needed.
- Diabetes mellitus: patients do comparably well after carpal tunnel release as normoglycaemic patients.
- Bilateral CTS: staged bilateral surgery (one hand at a time) is standard practice.
- Recurrent/Persistent CTS after surgery: revision open surgery with neurolysis; adhesiolysis of perineural fibrosis required.
Summary Flowchart
Diagnosis: Clinical + NCS/EMG
↓
Severity Assessment
↓
MILD/MODERATE SEVERE / Failed conservative
↓ ↓
Conservative: Surgical Release:
• Night splint ├── Open CTR (OCTR)
• Steroid injection │ • Experienced; any surgeon
• Activity modification │ • Direct visualization
• Physio/exercises │ • Best for additional pathology
│
├── Endoscopic CTR (ECTR)
│ • Agee (1-portal)
│ • Chow (2-portal)
│ • Faster return to work
│ • Experienced surgeons only
│
└── Ultrasound-guided CTR (CTR-US)
• Highest patient satisfaction
• Real-time nerve visualization
• Shortest return to work
- Sabiston Textbook of Surgery, 21e — Carpal Tunnel Syndrome & Nerve Compression Syndromes
- Schwartz's Principles of Surgery, 11e — Upper Extremity Nerve Compression
- Bradley and Daroff's Neurology in Clinical Practice — Carpal Tunnel Syndrome
- Goldman-Cecil Medicine — Compressive Mononeuropathy
- Elrosasy A et al., Neurosurg Rev 2025 — Network meta-analysis of 7 surgical CTR techniques [PMID: 40473869]
- Hacquebord JH et al., JAAOS 2022 — ECTR: Techniques and comparison to open [PMID: 35255490]
- Lusa V et al., Cochrane Database Syst Rev 2024 — Surgical vs. non-surgical CTS [PMID: 38189479]
Carpal Tunnel syndrome definition eloborate signs symptoms investigation treatment options comparison between minimally invasive versus endoscopic and procedure for endoscopic and steps everything in detail with appropriate images and illustration
"carpal tunnel" AND "endoscopic" AND "open release" AND comparison
carpal tunnel syndrome anatomy cross section median nerve transverse carpal ligament flexor retinaculum
"endoscopic carpal tunnel" AND "open carpal tunnel" AND outcomes
PMID: 38768022
"carpal tunnel syndrome" AND surgical treatment AND network meta-analysis
Tinel sign Phalen test carpal tunnel clinical examination wrist
PMID: 40473869
endoscopic carpal tunnel release Agee single portal Chow two portal technique steps
carpal tunnel syndrome median nerve distribution sensory map hand fingers thenar atrophy
open carpal tunnel release surgical incision palmar fascia flexor retinaculum division
🖐 CARPAL TUNNEL SYNDROME — Complete Clinical Reference
1. DEFINITION
"Carpal tunnel syndrome is the most common nerve entrapment syndrome... caused by compression of the median nerve at the wrist." — Goldman-Cecil Medicine & Sabiston Textbook of Surgery
2. SURGICAL ANATOMY
The Carpal Tunnel
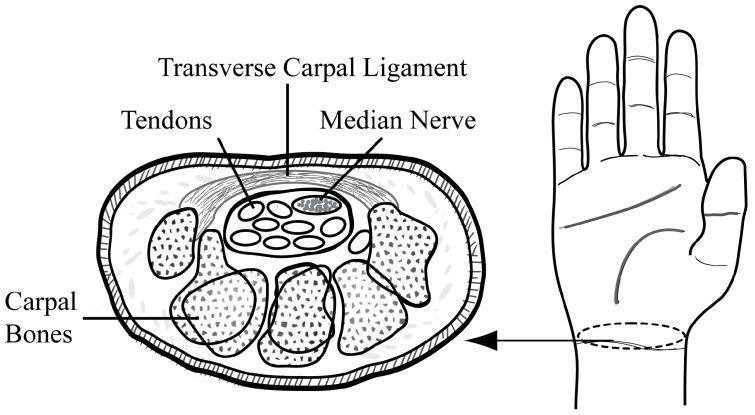
Boundaries of the Carpal Tunnel
| Wall | Structure |
|---|---|
| Roof (volar) | Transverse carpal ligament (flexor retinaculum) |
| Floor (dorsal) | Carpal bones (scaphoid, lunate, capitate) |
| Radial wall | Scaphoid tubercle |
| Ulnar wall | Hook of hamate + pisiform |
Contents — 10 Structures
- 1 × Median nerve (most superficial and radial — the most vulnerable)
- 4 × Flexor digitorum superficialis tendons (FDS)
- 4 × Flexor digitorum profundus tendons (FDP)
- 1 × Flexor pollicis longus tendon (FPL)
Normal carpal tunnel pressure = 20–30 mmHg. Pressure above this threshold causes compressive ischemic injury → demyelination → axonal death.
3. EPIDEMIOLOGY & RISK FACTORS
- Prevalence: ~53 per 10,000 working adults
- More common in women and during pregnancy
- Recognized as an occupational hazard with repetitive wrist loading
| Category | Examples |
|---|---|
| Occupational / Mechanical | Repetitive flexion-extension, vibrating tools, keyboard/mouse use |
| Metabolic | Diabetes mellitus, hypothyroidism (myxedema), acromegaly, amyloidosis |
| Hormonal | Pregnancy (fluid balance → increased tunnel pressure), oral contraceptives |
| Inflammatory | Rheumatoid arthritis (synovial hypertrophy), sarcoidosis |
| Structural / Traumatic | Carpal dislocations, distal radius malunion, Colles fracture |
| Space-occupying | Ganglion cysts, lipomas, anomalous muscles, giant cell tumors |
| Developmental | Anomalous muscles within the tunnel |
Diabetes mellitus patients respond equally well to carpal tunnel release as normoglycaemic patients. — Sabiston Textbook of Surgery
4. PATHOPHYSIOLOGY
↑ Tunnel pressure
↓
Venous congestion → epineural edema
↓
Chronic ischemia of median nerve
↓
Segmental demyelination
→ Slowed sensory/motor conduction velocity
→ Prolonged latencies on NCS
↓
Axonal degeneration (severe/chronic)
→ Denervation of thenar muscles
→ Fibrillations on EMG
→ Permanent thenar atrophy
5. CLINICAL FEATURES
5A. Symptoms — Sensory (Early)
- Paresthesias (tingling, numbness, "pins and needles") in the thumb, index, middle fingers, and radial half of ring finger — classic median nerve distribution
- Nocturnal awakening is the hallmark — flexed wrist posture during sleep raises tunnel pressure
- "Flick sign": patient shakes or flicks the wrist to relieve symptoms
- Activity-related worsening: driving, holding a phone, hair drying, reading
- Subjective numbness may radiate into the entire hand and even proximally to the shoulder (diffuse brachialgia)
Key diagnostic point: The thenar skin is NOT numb in CTS. The palmar cutaneous branch exits proximal to the tunnel and is spared. If thenar skin is numb, suspect a more proximal median nerve lesion (cervical radiculopathy C6/C7, pronator syndrome). — Bradley and Daroff's Neurology
5B. Symptoms — Motor (Late)
- Clumsiness and tendency to drop objects
- Difficulty with fine tasks: buttons, coins, jewelry clasps
- Weakness of thumb opposition and abduction
- Thenar atrophy (APB, opponens pollicis) — the classic late sign

6. PHYSICAL EXAMINATION SIGNS
Provocative Tests
| Sign | Technique | Positive Result | Sensitivity | Specificity |
|---|---|---|---|---|
| Phalen's Test | Wrists in maximal flexion for 60 s | Paresthesia in median distribution | ~74% | ~80% |
| Tinel's Sign | Tap/percuss median nerve at wrist crease | Electric shooting sensation into median digits | ~60% | ~67% |
| Reverse Phalen's (Prayer Test) | Wrists in maximal extension, palms pressed together for 60 s | Paresthesia in median distribution | ~75% | Variable |
| Durkan's Sign (Carpal Compression Test) | Direct thumb pressure over carpal tunnel for 30 s | Paresthesia reproduced — highest sensitivity | ~87% | ~90% |
| Thenar wasting | Inspection of thenar eminence | Flattened thenar bulk | Late sign | High specificity |
| 2-Point Discrimination | Static 2-point on fingertips | >6 mm | Indicates significant fiber loss | High |
| Thumb abduction weakness | Test abductor pollicis brevis strength | Reduced power | Motor involvement | High |
7. SEVERITY CLASSIFICATION
| Grade | Sensory | Motor | NCS/EMG |
|---|---|---|---|
| Mild | Intermittent paresthesias only with provocation | Normal | NCS borderline; normal EMG |
| Moderate | Frequent/nocturnal paresthesias; hypoesthesia on exam | Possible subtle weakness | Prolonged sensory latency; EMG may be normal |
| Severe | Constant numbness; objective sensory loss; widened 2-point discrimination | Thenar weakness/atrophy | Prolonged motor + sensory latency; fibrillations on EMG |
8. INVESTIGATIONS
Gold Standard: Nerve Conduction Studies (NCS) + EMG
- Prolonged distal sensory latency — most sensitive early marker (>3.5 ms over 14 cm)
- Prolonged distal motor latency to abductor pollicis brevis (>4.2 ms)
- Reduced sensory nerve action potential (SNAP) amplitude in moderate/severe cases
- Comparison with the ulnar nerve (internal control) improves sensitivity
- Polyphasic reinnervation potentials in APB (chronic denervation/reinnervation)
- Fibrillation potentials in APB = active axonal denervation (severe disease)
- Normal EMG does not exclude CTS if NCS is already abnormal
"Confirmation of the diagnosis is provided by nerve conduction studies and EMG: distal motor and sensory latencies are prolonged, and polyphasic reinnervation potentials are seen in the abductor pollicis brevis." — Bradley and Daroff's Neurology
Ultrasound of the Wrist
- Median nerve cross-sectional area (CSA) ≥ 10 mm² at the tunnel inlet = diagnostic threshold
- Hypoechoic swelling of the nerve with loss of normal fascicular pattern
- Palmar bowing of the flexor retinaculum
- Power Doppler: hypervascularity within compressed nerve
- Identifies structural causes (ganglion, lipoma, anomalous muscle)
- Guides injections and ultrasound-guided release procedures
MRI
- Not routinely required
- Reserved for atypical presentations or suspected structural mass (amyloid, tumor, post-traumatic)
- Shows nerve T2 signal changes and compressive lesions
Blood Tests — Screen for Systemic Causes
| Test | Purpose |
|---|---|
| Fasting glucose / HbA1c | Diabetes mellitus |
| TSH | Hypothyroidism |
| Rheumatoid factor / anti-CCP / ANA | Inflammatory arthropathy |
| Serum calcium + ACE | Sarcoidosis |
| IGF-1 | Acromegaly |
| Serum/urine protein electrophoresis | Amyloidosis (especially in elderly) |
Plain Radiographs
- When bony cause suspected: old fractures, carpal malalignment, degenerative arthritis
9. TREATMENT
9A. CONSERVATIVE (NON-SURGICAL) TREATMENT
1. Wrist Splinting
- Neutral wrist splint (0–20° extension) worn at night
- Prevents the flexed wrist posture during sleep that raises tunnel pressure
- Can provide symptom relief lasting years in mild CTS
- Daytime use for activity-related symptoms
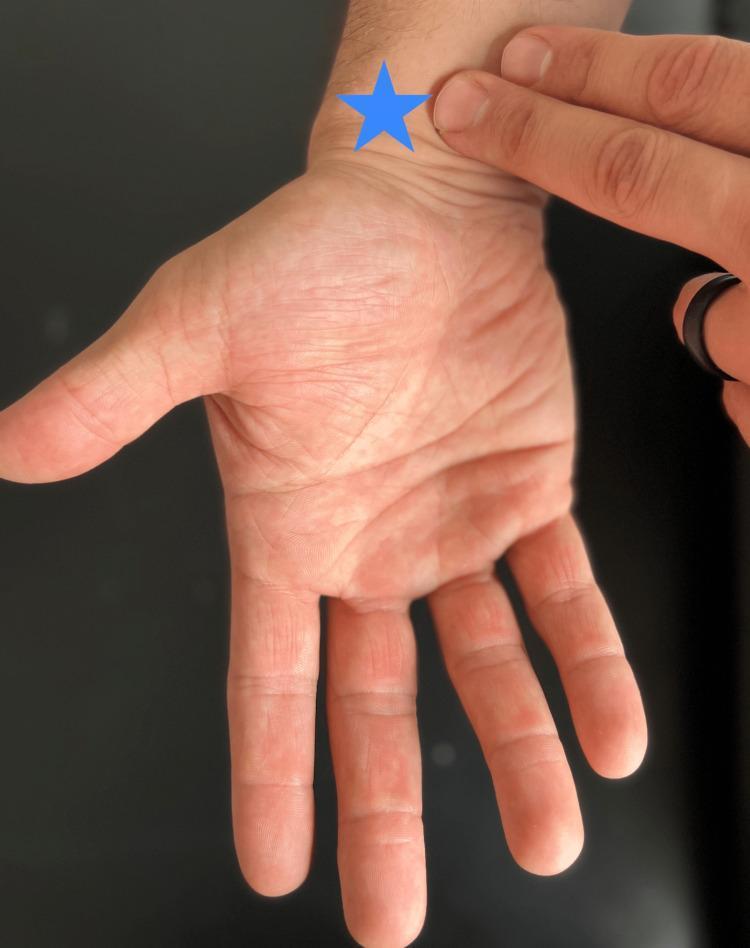
2. Corticosteroid Injection
- Injected into (not into) the carpal tunnel, ulnar to the palmaris longus tendon, proximal to the wrist crease
- Methylprednisolone 40 mg ± local anaesthetic (lidocaine)
- Local anaesthetic in the injection confirms correct placement — immediate anaesthesia in median nerve distribution
- Steroids take 3–7 days to reach peak effect
- Strong predictor: patients who respond well to injection do well with surgical release
- Typically limited to 2–3 injections; repeated injections carry risk of tendon rupture and fat atrophy
3. Activity Modification
- Ergonomic assessment: keyboard tilt, mouse grip, wrist position
- Avoidance of sustained wrist flexion/extension and repetitive loading
- Job modification or temporary work restriction
4. Physical Therapies
- Tendon and nerve gliding exercises (mobilise nerve within tunnel)
- Manual therapy: systematic review (PMID 34862562) shows modest short-term benefit for pain and function
- Physiotherapy/occupational therapy for strengthening and ergonomic education
5. Oral Medications
- NSAIDs: modest short-term analgesia
- Short oral corticosteroid course: temporary relief
- Vitamin B6: no established benefit
6. Ultrasound-Guided Hydrodissection with 5% Dextrose (D5W)
- Emerging technique; perineural injection of D5W separates the nerve from the ligament
- Systematic review & NMA (PMID 39894044) shows benefit over corticosteroid injection in some outcomes
- Non-steroid option safe for diabetic patients
9B. SURGICAL TREATMENT — INDICATIONS
- Conservative treatment has failed after 3–6 months
- Initial presentation with severe CTS (thenar atrophy, constant numbness, denervation on EMG)
- Progressive neurological deficit
- Confirmed electrophysiological nerve damage
- Structural cause identified requiring operative removal
Cochrane Review 2024 (PMID 38189479): Surgical treatment is superior to non-surgical treatment for long-term symptom relief in CTS.
10. SURGICAL TECHNIQUES IN DETAIL
The Common Goal
10A. OPEN CARPAL TUNNEL RELEASE (OCTR)
- Regional or local anaesthesia; tourniquet applied at the forearm or upper arm
- Longitudinal incision 3–5 cm in the palm — in line with the ring finger pad touching the proximal palm (avoids the palmar cutaneous branch of the median nerve, which runs radially)
- Skin → subcutaneous fat → palmar fascia divided
- Carpal tunnel contents visualized distally; median nerve identified and protected
- Transverse carpal ligament divided longitudinally from distal to proximal under direct vision
- Haemostasis; wound closed; bulky dressing; no cast
- Immediate finger movement encouraged
- Incision reduced to 1.5–2.5 cm
- Uses smaller retractors; slightly longer learning curve
- Comparable outcomes to standard open with less scar burden
10B. ENDOSCOPIC CARPAL TUNNEL RELEASE (ECTR)
Two Main Techniques:
| Agee (Single-Portal) | Chow (Two-Portal) | |
|---|---|---|
| Developer | Agee JM, 1992 | Chow JCY, 1989 |
| Portals | 1 (proximal wrist crease) | 2 (proximal wrist + distal palm) |
| Approach | Antegrade — scope + blade in one assembly | Retrograde — scope from proximal, blade from distal |
| Direction of cut | Proximal to distal | Distal to proximal |
| Instrument | Proprietary Agee endoscopic device | Slotted cannula + rigid endoscope + reverse-cutting blade |
| Visualization | Single assembly provides scope and blade | Two portals allow cross-verification of release |
| Learning curve | Moderate | Steeper |
| Advantage | Single small incision; faster setup | Better visualization of distal ligament; two-portal confirmation |
11. STEP-BY-STEP ENDOSCOPIC PROCEDURE (Chow Two-Portal Technique)
Pre-Operative Preparation
- Patient counselling: risks include median nerve injury, incomplete release, palmar arch injury, conversion to open
- Anaesthesia: local infiltration ± wrist block (median + ulnar nerve blocks), or IV regional (Bier block)
- Tourniquet: forearm or upper arm, inflated to 250 mmHg
- Position: patient supine, forearm fully supinated on a radiolucent hand table; wrist extended over a padded roll
- Equipment checklist: 2.7–4 mm rigid 0° endoscope, fibreoptic light source, camera system + monitor, slotted cannula assembly (synovial elevator + trocar), reverse-cutting hook blade
Step 1 — Surface Landmark Mapping
- Proximal wrist crease — site of proximal portal
- Kaplan's cardinal line — drawn from the apex of the first web space to the pisiform; intersection with the ring finger axis marks the distal portal
- Hook of hamate — palpated as a prominence in the ulnar palm; key safety landmark (ulnar neurovascular bundle lies ulnar to this)
- Axis of ring finger extended to the wrist — defines the safe corridor for cannula passage (ulnar border of median nerve)
Step 2 — Proximal Portal Incision
- Make a 1.5 cm transverse incision at the wrist crease, between the flexor carpi ulnaris and palmaris longus tendons
- Blunt dissect through subcutaneous fat using scissors; spread down to the level of the antebrachial fascia (do not incise yet — confirm layer)
- Divide the antebrachial (forearm) fascia transversely to enter the subretinacular space
- Protect the palmar cutaneous branch of the median nerve, which runs radially in this region
Step 3 — Tunnel Creation (Entry into Carpal Tunnel)
- Insert the blunt trocar + slotted cannula into the proximal incision
- Direct the instrument distally, staying in the subsynovial plane (superficial to the flexor tendons, deep to the transverse carpal ligament)
- Advance the cannula the full length of the transverse carpal ligament (~3–4 cm)
- Feel the resistance of the tunnel floor (flexor tendons) beneath and the ligament above
- Remove the trocar and replace with the rigid endoscope
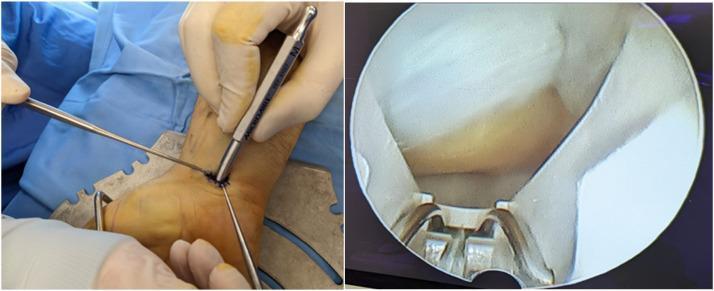
Step 4 — Transillumination (Chow Technique — Key Safety Step)
- The endoscope's light transilluminates through the palm skin with the room lights dimmed
- The surgeon palpates the palm to identify the bright spot — confirming the instrument tip is within the tunnel at the correct location
- This step confirms: the cannula is within the tunnel (not in the superficial fat), and the distal portal can be safely created
Step 5 — Distal Portal Creation
- Make a 1 cm transverse incision at the distal portal site (guided by transillumination and Kaplan's line)
- Insert a blunt probe through this incision to exit through the slotted cannula's distal opening
- The system now bridges the full length of the transverse carpal ligament between two small portals
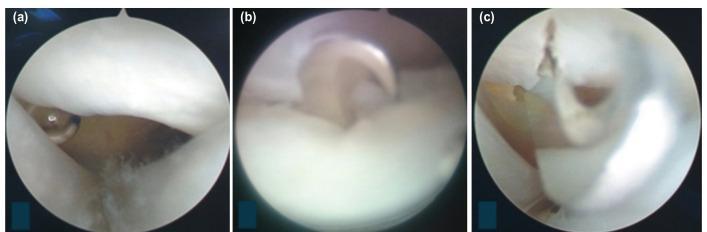
Step 6 — Endoscopic Visualization and Safety Check
- Insert the endoscope through the proximal portal and visualise the inside of the cannula
- The transverse carpal ligament appears as a dense, pale-white, fibrous band on the upper (dorsal) surface of the cannula slot
- Confirm the median nerve is NOT within the viewing slot (it must be lateral/radial to the cannula)
- Confirm the ulnar neurovascular bundle is medial to the hook of hamate (not in the operative corridor)
- The flexor tendons should be visible below — confirm the instrument is not inadvertently in a tendon sheath
Step 7 — Division of the Transverse Carpal Ligament
- Insert the reverse-cutting hook blade through the distal portal
- Under direct endoscopic vision, hook the blade onto the distal edge of the ligament
- Draw the blade from distal to proximal (retrograde cut) through the fibres of the transverse carpal ligament
- The fibres divide progressively under continuous endoscopic monitoring
- Continue until the proximal end of the ligament is fully divided
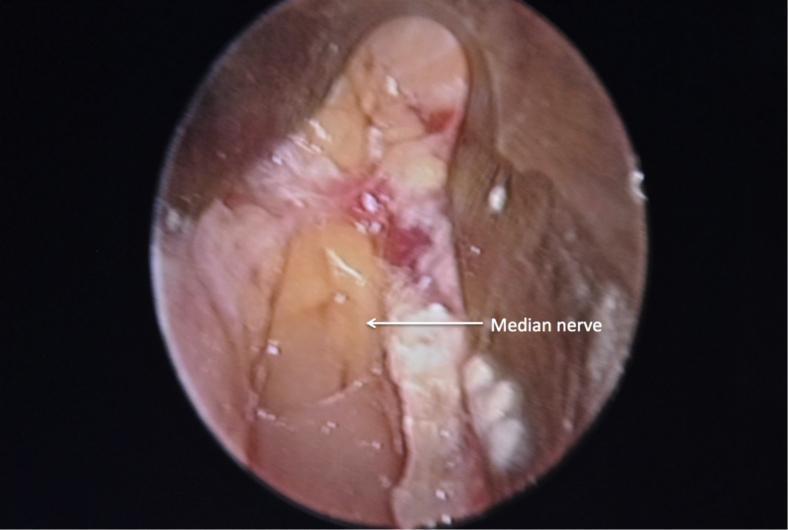
Step 8 — Confirmation of Complete Release
- The ligament edges should be fully separated — no residual intact fibres visible
- Palmar fat becomes visible through the divided ligament, confirming adequate superficial decompression
- The median nerve should be visible lying decompressed in the floor of the tunnel
- If any doubt about completeness: advance the scope to inspect the entire length of the release
Step 9 — Closure, Dressing, and Post-Operative Care
- Tourniquet released; active haemostasis confirmed
- Both portal incisions irrigated with saline
- Closed with 1–2 absorbable interrupted sutures per portal
- Bulky soft dressing applied (no plaster/cast)
- Elevate hand for 24–48 hours
- Begin active finger exercises immediately (prevents stiffness, promotes tendon gliding)
- Wrist can be used for light activity within days
- Desk/office work: 1–2 weeks
- Light manual work: 2–3 weeks
- Heavy manual work: 4–6 weeks (versus 6–12 weeks for open CTR)
12. COMPARISON: OPEN vs. ENDOSCOPIC vs. MINIMALLY INVASIVE
Head-to-Head Comparison Table
| Parameter | Open CTR (OCTR) | Endoscopic CTR (ECTR) | Ultrasound-Guided CTR (CTR-US) |
|---|---|---|---|
| Incision size | 3–5 cm palmar | 2 portals × 1–1.5 cm | 1 small wrist incision |
| Direct nerve visualization | ✅ Full throughout | Indirect (endoscopic) | Real-time ultrasound |
| Learning curve | Low — all hand surgeons | Steep — experienced only | Moderate (US skills needed) |
| Symptom relief (early: 1–3 months) | Excellent | Superior to open | Superior |
| Long-term outcomes (6–12 months) | Equivalent | Equivalent | Equivalent |
| Postoperative pain | More; longer duration | Less intense, shorter | Least |
| Pillar pain / scar tenderness | Common (6–12 months) | Less common | Minimal |
| Return to work | 4–8 weeks | 1–3 weeks | Shortest |
| Pinch strength recovery | Slower | Faster (significant at 3 & 6 months) | Faster |
| Grip strength recovery | Slower | Faster | Faster |
| Risk of transient nerve injury | Lower | ⚠️ Slightly higher | Real-time avoidance |
| Risk of incomplete release | Very low | Higher in inexperienced hands | Lower with real-time US |
| Wound complications | Higher | Lower | Minimal |
| Patient satisfaction | High | High | Highest |
| Equipment cost | Low | Higher (endoscopic tower) | Moderate (ultrasound) |
| Applicability | Universal | Experienced centres only | Increasing availability |
| Address additional pathology | ✅ Yes (synovectomy, mass removal) | ❌ Limited | ❌ Limited |
| Anaesthesia | Local/regional | Local/regional | Local |
Evidence Summary from Recent High-Quality Studies
📊 Umbrella Review + Meta-Analysis (El Masri J et al., Ann Plast Surg 2024 — 9 meta-analyses; PMID 38768022):
- ECTR showed significantly better pinch strength at 3 months (MD = 0.70; 95% CI: 0.00–1.40) and 6 months (MD = 0.77; 95% CI: 0.14–1.40)
- OCTR was associated with significantly longer return to work than ECTR (MD = −10.89 days; 95% CI: −15.14 to −6.64; p < 0.00001)
- No significant differences in symptom severity, grip strength, pain, or operation time
- Differences in nerve injury rates were unclear due to statistical inconsistency
📊 Network Meta-Analysis of 7 Surgical Techniques (Elrosasy A et al., Neurosurg Rev 2025 — 32 RCTs, 2,916 patients; PMID 40473869):
- One-port and two-port ECTR: superior symptom relief at 3 months vs. conventional open CTR (two-port ECTR: SMD = −4.47; 95% CI: −5.67 to −3.26)
- One-port ECTR: best functional outcomes including grip (SMD = 1.37) and pinch strength across all timepoints
- Ultrasound-guided CTR: highest patient satisfaction (OR = 6.89; 95% CI: 1.87–25.43) and shortest return to work
- Double Tunnel Technique (DTT): lowest adverse event rate (OR = 0.05; 95% CI: 0.01–0.42)
- Operative time and scar tenderness: comparable across all techniques
- Long-term outcomes equivalent across all procedures
📊 Cochrane Systematic Review (Lusa V et al., 2024; PMID 38189479):
Surgical treatment is superior to non-surgical treatment for sustained relief of CTS.
📊 JAAOS Review (Hacquebord et al., J Am Acad Orthop Surg 2022; PMID 35255490):
"ECTR is equally effective as OCTR for alleviating CTS symptoms with no differences in long-term outcomes. ECTR has increased risk of transient nerve injury; OCTR has increased risk of wound and scar complications. ECTR has higher direct costs but is associated with earlier return to work. ECTR is safe and effective in experienced hands — it is not for the occasional carpal tunnel surgeon."
13. COMPLICATIONS OF SURGICAL RELEASE
| Complication | Open | Endoscopic |
|---|---|---|
| Incomplete release / recurrence | Rare | Higher in inexperienced hands |
| Transient median nerve neurapraxia | Lower | ⚠️ Slightly higher (instrument pressure) |
| Palmar cutaneous nerve injury | Possible with incorrect incision | Less common |
| Injury to superficial palmar arch | Rare | Rare |
| Pillar pain (scar/thenar-hypothenar tenderness) | Common; can last 6–12 months | Less common |
| Bowstringing of flexor tendons | If incision too proximal | Very rare |
| Wound infection / dehiscence | Occasional | Less common |
| Complex Regional Pain Syndrome | Rare | Rare |
| Conversion to open | N/A | Intraoperative safety concern |
14. SPECIAL POPULATIONS
| Population | Management Note |
|---|---|
| Pregnancy | Conservative (splinting) first; usually resolves postpartum. Surgery rarely needed. |
| Diabetes mellitus | Outcomes post-surgery equivalent to non-diabetic patients |
| Bilateral CTS | Staged procedures — one hand at a time is standard |
| Elderly with amyloidosis | Search for systemic AL amyloid; bilateral CTS in elderly with heart failure is a red flag |
| Recurrent CTS post-surgery | Revision open surgery with neurolysis; adhesiolysis of perineural fibrosis |
15. CLINICAL DECISION PATHWAY
History + Physical Examination
↓
High clinical suspicion of CTS
↓
NCS + EMG
(confirm diagnosis & severity)
↓
Blood tests (glucose, TSH, RF, etc.)
to exclude systemic cause
↓
┌─────────────────────────────────────┐
│ │
MILD / MODERATE SEVERE
Initial presentation (atrophy, constant
or mild-moderate NCS numbness, EMG
denervation)
↓ ↓
CONSERVATIVE: SURGICAL RELEASE
• Night wrist splint ↓
• Steroid injection ┌──────────┼────────────┐
• Activity modification │ │ │
• Exercise / physio OPEN CTR ECTR CTR-US
• D5W hydrodissection (standard) (Agee/Chow) (emerging)
↓
Failure at 3–6 months
↓
SURGICAL RELEASE
- Sabiston Textbook of Surgery 21e — Carpal Tunnel Syndrome & Nerve Compression Syndromes
- Schwartz's Principles of Surgery 11e — Upper Extremity Nerve Compression
- Bradley and Daroff's Neurology in Clinical Practice 8e — Median Nerve / CTS
- Goldman-Cecil Medicine — Compressive Mononeuropathy
- Gray's Anatomy for Students — Carpal Tunnel Syndrome
- El Masri J et al. Umbrella Review + Meta-analysis, Ann Plast Surg 2024 [PMID: 38768022]
- Elrosasy A et al. Network Meta-Analysis 32 RCTs, Neurosurg Rev 2025 [PMID: 40473869]
- Hacquebord JH et al. ECTR Techniques & Comparison, JAAOS 2022 [PMID: 35255490]
- Lusa V et al. Cochrane Review Surgical vs Non-surgical CTS 2024 [PMID: 38189479]