Cyclosporines classification mechanism of action dosage usage uses in Orthopedics side effects preventions everything related to this with appropriate illustrative images and flowcharts
cyclosporine calcineurin inhibitor mechanism of action T cell activation NFAT
cyclosporine orthopedics bone joint immunosuppression
cyclosporine drug interactions CYP3A4 side effects nephrotoxicity hirsutism gingival
cyclosporine uses orthopedics rheumatoid arthritis psoriatic arthritis reactive arthritis 2024 2025
cyclosporine rheumatoid arthritis methotrexate combination
| Section | Content |
|---|---|
| 1. Classification | Chemical origin, drug class, position in immunosuppressant hierarchy |
| 2. Mechanism of Action | Detailed step-by-step intracellular pathway with diagram |
| 3. Visual flowchart | Bailey & Love's T-cell activation diagram showing CsA's exact site of action |
| 4. Pharmacokinetics | Formulations, bioavailability, metabolism, excretion |
| 5. Dosage | Indication-specific doses, monitoring targets |
| 6. Uses — including Orthopedics | Full table including RA, psoriatic arthritis, perioperative management, GVHD, heterotopic ossification |
| 7. Side Effects | Flowchart + clinical photo of gingival hyperplasia |
| 8. Drug Interactions | CYP3A4 inducers/inhibitors, additive toxicities |
| 9. Monitoring | Parameters, frequency, targets |
| 10–11. Contraindications & Prevention | What to avoid, how to manage side effects |
| 12. Comparison Table | CsA vs other immunosuppressants |
| 13. Orthopedic Flowchart | Decision tree for CsA use in inflammatory joint disease |
Cyclosporines classification mechanism of action dosage usage uses in Orthopedics side effects preventions everything related to this with appropriate illustrative images and flowcharts
cyclosporine calcineurin inhibitor mechanism T cell NFAT IL-2 cyclophilin pathway diagram
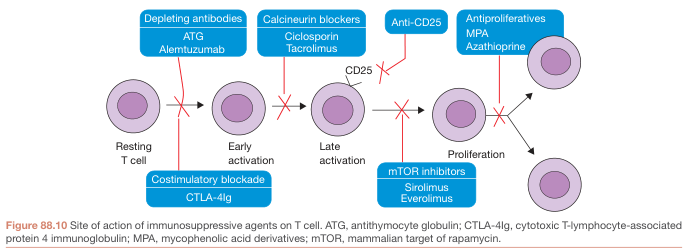
immunosuppressant drugs classification calcineurin mTOR antiproliferative site of action T cell
cyclosporine gingival hyperplasia nephrotoxicity clinical photo side effect
cyclosporine drug interactions CYP3A4 pharmacokinetics table
rheumatoid arthritis joint destruction treatment DMARD flowchart algorithm
cyclosporine rheumatoid arthritis psoriatic arthritis efficacy
cyclosporine orthopedics uses perioperative management transplant patients 2024
🔬 CYCLOSPORINE (Cyclosporin A / CsA) — Complete Clinical Reference
SECTION 1 — CLASSIFICATION
Origin
Pharmacological Classification
IMMUNOSUPPRESSANT DRUGS
│
├── 1. CALCINEURIN INHIBITORS (CNIs) ◄─── CYCLOSPORINE is here
│ ├── Cyclosporine (binds CYCLOPHILIN)
│ └── Tacrolimus (binds FKBP-12)
│
├── 2. mTOR INHIBITORS
│ ├── Sirolimus (Rapamycin)
│ └── Everolimus
│
├── 3. COSTIMULATION BLOCKERS
│ └── Belatacept
│
├── 4. ANTIPROLIFERATIVES / ANTIMETABOLITES
│ ├── Mycophenolate mofetil (MMF)
│ └── Azathioprine
│
└── 5. CORTICOSTEROIDS
└── Prednisolone, Methylprednisolone
SECTION 2 — MECHANISM OF ACTION
Visual Diagram (Fitzpatrick's Dermatology, Fig. 192-2):
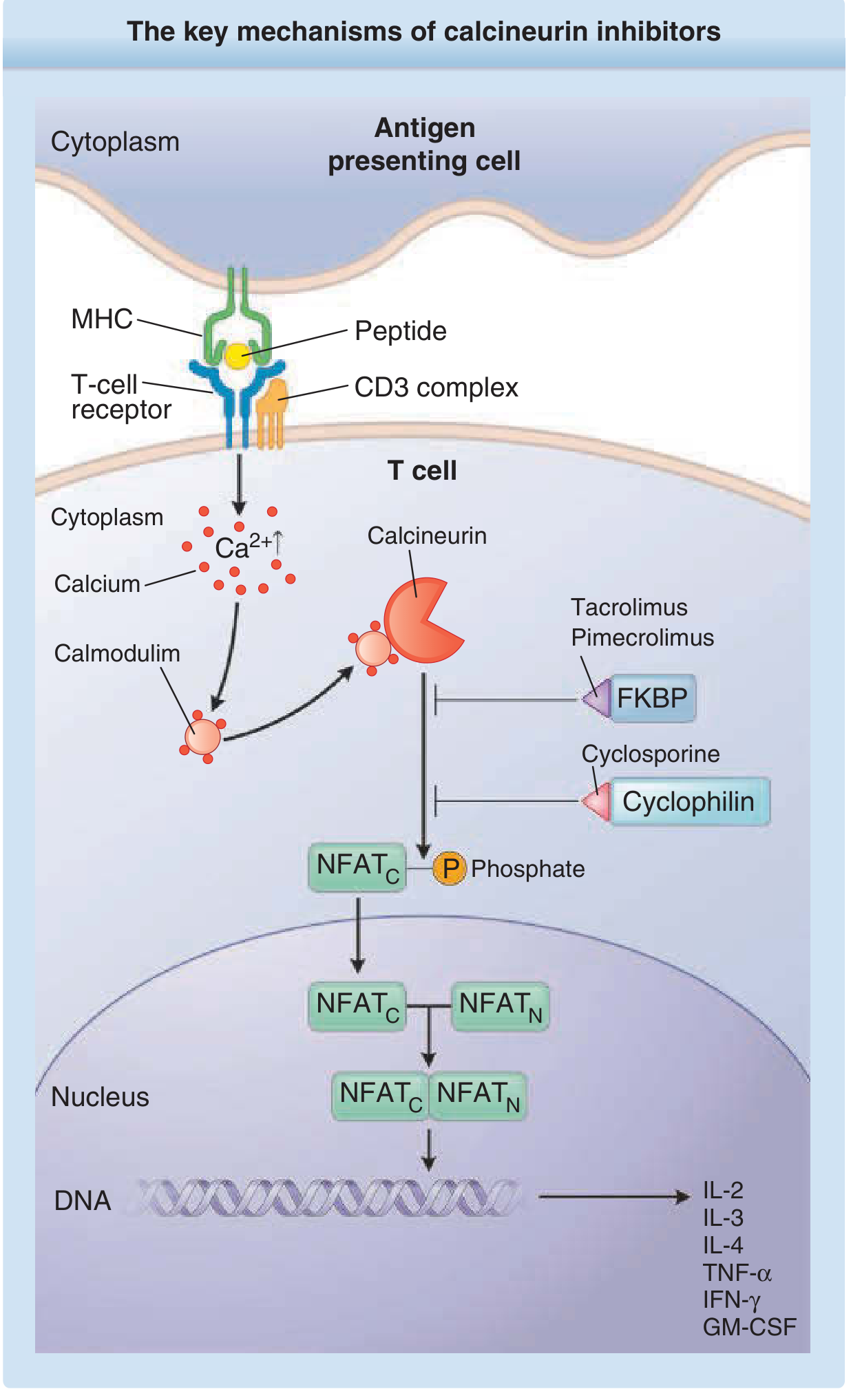
Step-by-Step Molecular Cascade
NORMAL T-CELL ACTIVATION:
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
APC presents peptide (in MHC groove) to T-cell receptor
↓
TCR + CD3 complex activation
↓
Transmembrane signalling → ↑↑ intracellular Ca²⁺
↓
Ca²⁺ binds CALMODULIN
↓
Ca²⁺–Calmodulin activates CALCINEURIN
(serine/threonine phosphatase: CnA catalytic + CnB regulatory subunits)
↓
Calcineurin DEPHOSPHORYLATES cytoplasmic NFAT (NFATc)
↓
NFATc translocates to NUCLEUS
↓
NFATc + NFATn complex → binds cytokine gene promoters
↓
TRANSCRIPTION: IL-2, IL-3, IL-4, TNF-α, IFN-γ, GM-CSF
↓
T-cell ACTIVATION → PROLIFERATION → IMMUNE RESPONSE
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
HOW CYCLOSPORINE BLOCKS THIS:
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
CsA (lipophilic) → freely diffuses into T-cell cytoplasm
↓
Binds CYCLOPHILIN (immunophilin receptor, high affinity)
↓
CsA–Cyclophilin complex → BINDS CALCINEURIN
↓
CALCINEURIN IS INHIBITED (phosphatase activity blocked)
↓
NFATc remains PHOSPHORYLATED → CANNOT enter nucleus
↓
NO cytokine gene transcription
↓
NO IL-2 production → T-cell NOT activated
↓
IMMUNOSUPPRESSION achieved
"CsA inhibits T-cell activation mediated by antigens by blocking the downstream signalling cascade of the T-cell receptor, but it does not inhibit the early phases of T-lymphocyte signal transduction." — Fitzpatrick's Dermatology, p. 3550
Additional Immune Effects
| Effect | Details |
|---|---|
| Cyclophilin–apoptosis | Cyclophilin also mediates apoptosis and degranulation of cytotoxic T-lymphocytes — CsA inhibits this |
| TGF-β upregulation | CsA increases TGF-β, which further inhibits IL-2–stimulated T-cell proliferation |
| Humoral immunity | Partially suppressed (B-cell dependent on T-helper cells) |
| Antiapoptotic proteins | Blunts expression in lymphocytes |
SECTION 3 — SITE OF ACTION AMONG IMMUNOSUPPRESSANTS
SECTION 4 — FORMULATIONS & PHARMACOKINETICS (ADME)
Formulations
| Product | Description | Note |
|---|---|---|
| SANDIMMUNE | Original soft gelatin capsule + oral solution | Erratic bioavailability (20–50%); AVOID switching |
| NEORAL | Modified microemulsion — most widely used | More uniform, slightly higher bioavailability; 25 mg & 100 mg capsules; 100 mg/mL solution |
| GENGRAF | Second modified formulation | Also NOT interchangeable with Sandimmune |
| IV formulation | Ethanol + polyoxyethylated castor oil vehicle; dilute in NS or D5W before injection | Discontinue IV → switch to oral ASAP; more adverse effects with IV route |
⚠️ Critical safety point: SANDIMMUNE and NEORAL are NOT bioequivalent and cannot be substituted without close monitoring. Inadvertent substitution can cause graft loss or toxicity. — Goodman & Gilman's, p. 793
Pharmacokinetics Summary
| PK Parameter | Detail |
|---|---|
| Absorption | Oral: incomplete, highly variable; food delays and reduces absorption (AUC ↓13%, Cmax ↓33% with high-fat meal) |
| Peak plasma level (Neoral) | 1.5–4 hours post-dose |
| C2 level | Level at 2 h post-dose — better AUC correlate than trough C0 level |
| Volume of Distribution | 3–5 L/kg (IV) in transplant recipients; 13 L/kg (Fitzpatrick's) — extensive extravascular distribution |
| Blood binding | Binds to lymphocytes, granulocytes, erythrocytes + plasma lipoproteins; whole blood levels preferred for monitoring |
| Half-life (t½) | 5–18 hours (biphasic elimination); ~6–12 h in healthy subjects |
| Metabolism | Hepatic CYP3A4 primarily; also GI tract/kidneys; >30 metabolites (partially active) |
| Excretion | >90% biliary/fecal; only ~6% urinary; renal failure does not substantially alter clearance |
| Special populations | Hepatic dysfunction → dose reduction required; dialysis/renal failure → NO adjustment needed |
SECTION 5 — DOSAGE
| Indication | Standard Dose | Notes |
|---|---|---|
| Renal transplant | 3–5 mg/kg/day PO ÷ 2 doses | Delay initiation until threshold renal function reached; guided by trough levels |
| Liver / Heart transplant | Protocol-dependent; typically 2–5 mg/kg/day | Combined with steroids ± MMF or azathioprine |
| Rheumatoid arthritis | 2.5–4 mg/kg/day PO ÷ 2 doses | Severe RA unresponsive to MTX; can combine with MTX with close monitoring |
| Psoriasis (severe plaque) | 2.5–5 mg/kg/day; optimal control up to 4–5 mg/kg/day | Short courses; avoid continuous use >1 year |
| Psoriatic arthritis | 2.5–4 mg/kg/day | GRAPPA-recommended DMARD |
| Nephrotic syndrome | 3–5 mg/kg/day | Minimal change disease, FSGS |
| Pediatric | Weight-based; adjusted to trough; monthly BP monitoring | JDM, MAS, JIA |
| IV (when oral not possible) | ~⅓ of oral dose | Switch to oral as soon as feasible |
Therapeutic Drug Monitoring Targets
| Timeframe | Trough (C0) Target |
|---|---|
| 0–3 months post-transplant | 250–300 ng/mL |
| 3–6 months | 200–300 ng/mL |
| 6–12 months | 150–250 ng/mL |
| >12 months | 100–150 ng/mL |
SECTION 6 — THERAPEUTIC USES
6A — Transplantation
- Kidney, liver, heart transplant: cornerstone CNI immunosuppression in combination regimens
- Bone marrow / stem cell transplant: GVHD prophylaxis (combined with methotrexate — standard regimen)
- Initial dose delayed in renal transplant until threshold renal function attained
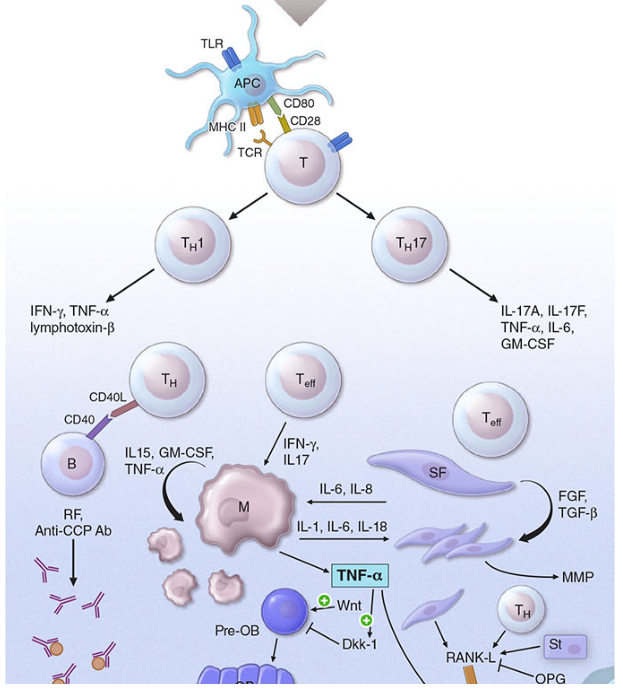
6B — Rheumatologic / Musculoskeletal Conditions
Rheumatoid Arthritis — the Inflammation Cascade CsA Targets:
| Condition | Role of Cyclosporine |
|---|---|
| Rheumatoid Arthritis | Used in severe RA unresponsive to methotrexate; can combine CsA + MTX (both levels monitored closely) — FDA-approved |
| Psoriatic Arthritis | GRAPPA strongly recommends CsA as a DMARD; controls skin + joint disease |
| Psoriasis (severe plaque) | Adult immunocompetent patients with severe, disabling disease where other systemic therapies contraindicated or failed |
| Behçet's disease | Especially for ocular and joint manifestations |
| Endogenous uveitis | Well-established |
| Atopic dermatitis | Established evidence |
| SLE (lupus) | ACR-recognized; especially renal and cutaneous involvement |
| Juvenile dermatomyositis (JDM) | Most common pediatric rheumatology use |
| Macrophage Activation Syndrome (MAS) | Associated with systemic JIA — rescue therapy |
| Inflammatory bowel disease | Rescue therapy for severe refractory Crohn's/UC |
| Nephrotic syndrome | Steroid-dependent / frequently relapsing minimal change disease, FSGS |
| Dry eye (xerophthalmia) | FDA-approved ophthalmic formulation (Restasis 0.05%) |
6C — 🦴 Uses Specific to Orthopedics
| Orthopedic Context | Role & Significance |
|---|---|
| Rheumatoid Arthritis (erosive joint disease) | Reduces synovial T-cell–driven inflammation; slows joint space narrowing in severe, MTX-refractory RA; used as DMARD before biologics |
| Psoriatic Arthritis with joint involvement | Controls both skin and joint disease; reduces enthesitis, dactylitis, and erosive damage; combined DMARD option |
| Reactive / inflammatory arthritis | Adjunct immunosuppression in refractory cases |
| Gout (secondary hyperuricemia) | CsA itself causes hyperuricemia → gout flares; orthopedic surgeons must recognize CsA as a cause of acute gout in transplant patients |
| Perioperative management of transplant recipients undergoing orthopedic surgery | CsA must be continued perioperatively (transplant patients); blood levels monitored daily; adjust for fluid dilution, drug interactions, and NPO status |
| GVHD (bone marrow transplant) | Prevents GVHD affecting musculoskeletal tissues (myopathy, fasciitis, arthropathy) |
| Macrophage Activation Syndrome (systemic JIA) | Rescue therapy affecting joints, bone marrow |
| Heterotopic ossification (emerging evidence) | NFAT pathway modulation by CNIs may affect ectopic bone formation; experimental data only — not standard of care |
TRANSPLANT PATIENT ON CYCLOSPORINE → ORTHOPEDIC SURGERY
│
┌───────────────┼───────────────┐
│ │ │
CONTINUE MONITOR AVOID
CsA throughout blood levels NSAIDs
perioperative daily (additive
period perioperatively nephrotoxicity)
│ │ │
If NPO → Adjust dose for Use
IV CsA fluid dilution paracetamol/
(~1/3 oral) and drug opioids
interactions post-op
"Patients with organ transplants should be continued on immunosuppressant medications unless directed otherwise by transplant physician." — Froedtert Hospital Perioperative Medication Guidelines
"Clinically significant reductions of cyclosporine blood levels can be caused by dilution with massive fluid infusion perioperatively and cardiopulmonary bypass." — IARS Anesthesia & Analgesia
SECTION 7 — SIDE EFFECTS
Master Adverse Effects Flowchart
CYCLOSPORINE ADVERSE EFFECTS
│
┌─────────┼──────────────────────┐
│ │ │
RENAL CARDIOVASCULAR METABOLIC
│ │ │
Nephrotoxicity Hypertension ┌───┴────────────────────┐
(majority of (~50% renal tx; │ Hyperlipidemia (↑LDL) │
patients) ~100% cardiac) │ Hyperkalemia │
│ │ Hyperuricemia → GOUT │
Acute: │ Hyperglycemia / DM │
renal vasoconstriction │ Hypomagnesemia │
(reversible with └────────────────────────┘
dose reduction)
Chronic:
interstitial fibrosis
│
┌─────────┼────────────────────────┐
│ │ │
COSMETIC NEUROLOGICAL ONCOLOGICAL
│ │ │
Hirsutism Tremor (common) ↑ Lymphoma risk
Gingival Headache Post-transplant
hyperplasia Paresthesias lymphoproliferative
Mental confusion disorder (PTLD)
Hallucinations Skin malignancy
Seizures (rare) (SCC > BCC)
PRES
│
┌─────────┼─────────────┐
│ │ │
INFECTIONS GI OTHER
│ │ │
Opportunistic Nausea Pancreatitis
infections Vomiting Hepatotoxicity
(fungal, Diarrhea Dyspnea
bacterial,
viral — CMV)
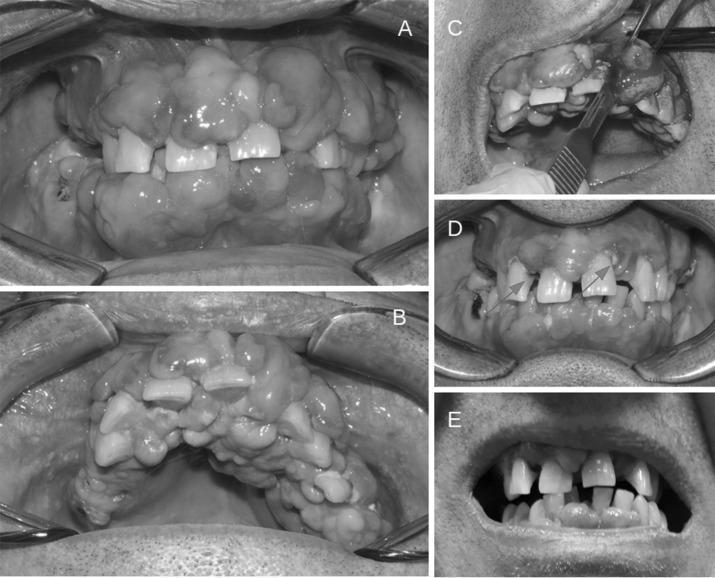
Gingival Hyperplasia — Clinical Photographs

Comparison: Cyclosporine vs. Tacrolimus Side Effects
| Side Effect | Cyclosporine | Tacrolimus |
|---|---|---|
| Nephrotoxicity | ✅ Yes (major) | ✅ Yes (major) |
| Hypertension | ✅ ~50% renal, ~100% cardiac | ✅ Yes |
| Hirsutism | ✅ More common | ✗ Less; hair loss instead |
| Gingival hyperplasia | ✅ Yes | ✗ No |
| Hyperlipidemia (LDL ↑) | ✅ More | Less |
| Hyperglycemia / DM | ✅ (less than tacrolimus) | ✅ More diabetogenic |
| Neurotoxicity | ✅ Tremor, seizures | ✅ More tremor, headache |
| Alopecia | ✗ No | ✅ Yes |
| Diarrhea | Less | More |
SECTION 8 — DRUG INTERACTIONS
From Fitzpatrick's Dermatology (comprehensive table):
| Interaction Type | Drug Class | Examples |
|---|---|---|
| ↑ CsA levels (CYP3A4 inhibitors — ↑ toxicity risk) | Ca²⁺ channel blockers | Diltiazem, nicardipine, verapamil |
| Antibiotics | Erythromycin, clarithromycin, azithromycin, quinupristin | |
| Antifungals | Fluconazole, itraconazole, ketoconazole, voriconazole | |
| Antivirals (HIV) | Ritonavir, indinavir, saquinavir, nelfinavir | |
| Glucocorticoids | Methylprednisolone | |
| Other | Allopurinol, amiodarone, bromocriptine, colchicine, danazol, metoclopramide, oral contraceptives | |
| Food | GRAPEFRUIT JUICE ⚠️ (CYP3A4 + P-gp inhibition) | |
| ↓ CsA levels (CYP3A4 inducers — ↓ efficacy) | Antibiotics | Rifampin, nafcillin |
| Anticonvulsants | Carbamazepine, phenobarbital, phenytoin, oxcarbazepine | |
| Other | St. John's wort, bosentan, orlistat, octreotide, terbinafine | |
| Additive TOXICITY | NSAIDs | Diclofenac, naproxen, sulindac, colchicine ⚠️ Nephrotoxicity |
| Antibiotics | Ciprofloxacin, gentamicin, vancomycin, TMP-SMX | |
| Antifungals | Amphotericin B | |
| Immunosuppressants | Tacrolimus (synergistic nephrotoxicity — avoid) | |
| Antimetabolites | Methotrexate (↑ MTX levels), fibrates | |
| CsA as inhibitor (CYP3A4 + P-gp) | CsA ↑ levels of: | Statins (↑ myopathy risk), prednisolone, digoxin, MTX |
⚠️ Orthopedic Alert — NSAIDs + Cyclosporine: Additive nephrotoxicity. Commonly used post-op analgesics (diclofenac, naproxen, ketorolac) must be avoided or used with extreme caution in patients on cyclosporine. — Goodman & Gilman's, p. 794
SECTION 9 — MONITORING
Monitoring Protocol Flowchart
INITIATE CYCLOSPORINE
│
BASELINE ASSESSMENTS
─────────────────────────────────────────────
• Blood pressure (both arms)
• Serum creatinine + eGFR
• Full blood count (CBC)
• Liver function tests
• Fasting lipid panel
• Uric acid
• Blood glucose / HbA1c
• Urinalysis (proteinuria)
• CsA baseline levels (trough C0 or C2)
• Dermatologic exam (skin cancer baseline)
│
FIRST 3 MONTHS (most intensive)
─────────────────────────────────────────────
• BP: at each visit
• Creatinine: every 2 weeks
• CsA trough (C0): weekly → every 2 weeks
• C2 if used: exactly 2 h after dose
• CBC + LFTs: monthly
│
MONTHS 3–12 (stable phase)
─────────────────────────────────────────────
• BP + Creatinine: monthly
• CsA trough: monthly
• Lipids + uric acid: every 3–6 months
• Annual skin surveillance (SCC risk)
│
TARGETS / ACTION THRESHOLDS
─────────────────────────────────────────────
• Creatinine rise >30% from baseline
→ REDUCE DOSE or STOP
• BP >130/80 → Antihypertensive (amlodipine
preferred; avoid diltiazem/verapamil)
• eGFR declining trend → Consider switch
to tacrolimus or non-CNI
SECTION 10 — CONTRAINDICATIONS
| Contraindication | Rationale |
|---|---|
| Uncontrolled hypertension | CsA worsens; increased stroke/renal risk |
| Significant renal impairment at baseline | Additive nephrotoxicity; may cause irreversible damage |
| Active uncontrolled infection | Immunosuppression will exacerbate |
| Current malignancy (especially lymphoma/skin) | CsA promotes tumor growth |
| Concomitant tacrolimus | Synergistic nephrotoxicity |
| Concomitant sirolimus (simultaneous) | Must time-separate (cyclosporine worsens sirolimus-induced hyperlipidemia; sirolimus worsens CsA nephrotoxicity) |
| Pregnancy | Teratogenic; discuss risk/benefit; ACR advises avoid |
| Breastfeeding | Excreted in breast milk |
| Hypersensitivity to polyoxyethylated castor oil | (IV formulation only) |
SECTION 11 — PREVENTION & MANAGEMENT OF SIDE EFFECTS
| Side Effect | Prevention | Management |
|---|---|---|
| Nephrotoxicity | Lowest effective dose; avoid NSAIDs, aminoglycosides, amphotericin; baseline renal assessment | Dose reduction (reversible); if graft dysfunction: biopsy to differentiate rejection vs. toxicity; switch to tacrolimus if persistent |
| Hypertension | Avoid high-sodium diet; monitor BP at every visit | Amlodipine (preferred CCB — no CYP3A4 interaction); ACE inhibitors; avoid diltiazem/verapamil |
| Gingival hyperplasia | Strict oral hygiene; regular dental review | Gingivoplasty/gingivectomy if severe; switch to tacrolimus (reverses overgrowth) |
| Hirsutism | Counsel patient pre-treatment | Cosmetic management; switch to tacrolimus if socially unacceptable |
| Hyperlipidemia | Low-fat diet; monitor lipids 3–6 monthly | Statins (pravastatin preferred — least CYP3A4 interaction); avoid lovastatin/simvastatin (high myopathy risk with CsA) |
| Hyperuricemia / Gout | Avoid allopurinol (unless dose-adjusted — allopurinol ↑ CsA levels); low-purine diet | Colchicine (caution: CsA ↑ colchicine toxicity → use low dose); dose reduction |
| Hyperkalemia | Low-potassium diet; avoid K-sparing diuretics | Kayexalate; dose reduction |
| Infection risk | PCP prophylaxis (TMP-SMX); CMV prophylaxis post-transplant; antifungal prophylaxis | Treat aggressively; consider dose reduction |
| Malignancy | Sun protection (SPF 50+); annual skin surveillance; avoid prolonged high-dose use; avoid combination with UV therapy | Dermatology surveillance; switch immunosuppression class; consider mTOR inhibitors (sirolimus has antitumor properties) |
| Neurotoxicity (tremor, seizures) | Maintain therapeutic drug levels | Dose reduction; if seizures: avoid hyperventilation perioperatively; lower seizure threshold with CsA |
SECTION 12 — MAINTENANCE IMMUNOSUPPRESSANT COMPARISON TABLE
| Drug | Class | Key Indications | PK | Adverse Effects |
|---|---|---|---|---|
| Cyclosporine | CNI | SOT, psoriasis, RA, GVHD | CYP3A4; P-gp inhibitor | HTN, nephrotoxicity, hirsutism, gingival hyperplasia, HLD, neurotoxicity |
| Tacrolimus | CNI | SOT, GVHD | CYP3A4 | HTN, nephrotoxicity, DM, alopecia, neurotoxicity |
| Sirolimus | mTOR inhibitor | SOT (renal, heart), GVHD | CYP3A4 | Impaired wound healing ⚠️, HLD, proteinuria, myelosuppression |
| Everolimus | mTOR inhibitor | SOT, oncology | CYP3A4 | Same as sirolimus; stomatitis |
| Mycophenolate | Antiproliferative | SOT, SLE | Glucuronidation | Myelosuppression, GI effects |
| Azathioprine | Antiproliferative | SOT, RA, lupus | Thiopurine pathway | Myelosuppression, hepatotoxicity, pancreatitis |
| Corticosteroids | Corticosteroid | Many | — | HTN, osteoporosis, DM, Cushing's |
| Belatacept | Costimulation blocker | SOT (renal) | t½ ~10 days | ↑ PTLD risk, anemia |
Orthopedic Note on Sirolimus: Unlike cyclosporine, sirolimus significantly impairs wound healing — this is a critical distinction when managing post-surgical patients.
SECTION 13 — CLINICAL DECISION FLOWCHART: Cyclosporine in Orthopedic / Rheumatologic Practice
PATIENT WITH INFLAMMATORY JOINT DISEASE
(RA / Psoriatic Arthritis / Reactive Arthritis)
│
▼
┌───────────────────────────────┐
│ STEP 1: FIRST-LINE DMARDs │
│ Methotrexate (MTX) │
│ Sulfasalazine │
│ Hydroxychloroquine │
└───────────────┬───────────────┘
│
Adequate response?
YES ─────┴────── NO
│ │
Continue 3–6 months
& Monitor inadequate
│
▼
┌─────────────────────────────────────┐
│ STEP 2: CONSIDER CYCLOSPORINE │
│ Indication: │
│ • RA refractory to MTX │
│ • Severe psoriatic arthritis │
│ • Cannot use biologics │
│ Dose: 2.5–4 mg/kg/day PO ÷ 2 │
└────────────────┬────────────────────┘
│
Can add MTX to CsA? YES — monitor BOTH levels
│
┌─────────────▼────────────────────┐
│ BASELINE ASSESSMENTS │
│ BP, Cr, eGFR, CBC, LFTs, │
│ Lipids, Uric acid, UA, CsA level │
└─────────────┬────────────────────┘
│
Monitor q2 weeks × 3 months
then monthly
│
┌──────────┴──────────┐
│ │
Adequate response Inadequate response
& tolerable or side effects
│ │
Continue at ┌────┴──────────────┐
lowest effective │ │
dose Dose Switch to:
adjust • Tacrolimus
• Biologic DMARD
(TNF-i, IL-17-i)
• JAK inhibitor
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
PERIOPERATIVE PATHWAY (Orthopedic Surgery)
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
Patient on CsA → ELECTIVE ORTHO SURGERY
│
├─ TRANSPLANT patient → CONTINUE CsA throughout
│ (consult transplant team)
│
├─ RA/PsA patient (non-severe SLE) → CONTINUE CsA
│ (ACR guidelines)
│
├─ NPO perioperatively → SWITCH to IV CsA (~1/3 oral dose)
│
├─ AVOID NSAIDs postoperatively (additive nephrotoxicity)
│ → Use paracetamol, opioids, COX-2 (with caution)
│
├─ Monitor CsA blood levels DAILY perioperatively
│
└─ Check for drug interactions with anesthetic agents
and antibiotics used
KEY CLINICAL PEARLS — Quick Reference
| Situation | Key Point |
|---|---|
| NSAIDs + CsA | Additive nephrotoxicity — use paracetamol instead post-op |
| Formulation switch | SANDIMMUNE ≠ NEORAL — never switch without close monitoring |
| Grapefruit | Inhibits CYP3A4 → ↑ CsA levels → toxicity |
| Rifampin / Phenytoin | Dramatically ↓ CsA levels → rejection risk |
| Statin choice | Use pravastatin (least CYP3A4); avoid lovastatin/simvastatin |
| Gout flare on CsA | CsA causes hyperuricemia; recognize as CsA complication; low-dose colchicine |
| BP management | Amlodipine preferred; NOT diltiazem/verapamil (↑ CsA levels) |
| Wound healing | CsA does NOT impair wound healing (unlike sirolimus/everolimus) |
| Creatinine ↑ >30% | Reduce dose immediately; if persistent → biopsy or switch |
| Gingival hyperplasia | Switch to tacrolimus — resolves within months |
References
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, 14th ed., Chapter 39
- Fitzpatrick's Dermatology, 9th ed., Chapter 192 (Calcineurin Inhibitors)
- Lippincott Illustrated Reviews: Pharmacology, 8th ed., Chapter 38
- Harrison's Principles of Internal Medicine, 22nd ed. (2025)
- Bailey & Love's Short Practice of Surgery, 28th ed., Chapters 88–89
- Sabiston Textbook of Surgery, 21st ed.
- National Kidney Foundation Primer on Kidney Diseases, 8th ed.
- ACR 2017 Guideline — Perioperative Management of Antirheumatic Medications
- ACR Patient Education — Cyclosporine (updated February 2025)
- GRAPPA Guidelines for Psoriatic Arthritis