Tell me about vagus nerve
Reading File
Finding Sources
Searching the Web
vagus nerve anatomy functions clinical significance
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have rich, comprehensive content from multiple authoritative textbooks. Let me compose the full answer.
Vagus Nerve (Cranial Nerve X)
The vagus nerve is the 10th cranial nerve and the longest of all cranial nerves. Its name comes from the Latin vagus, meaning "wandering," which perfectly describes its extensive course from the brainstem all the way to the abdominal viscera. It is a mixed nerve carrying four fiber types: parasympathetic (preganglionic), branchial motor, general visceral afferent, and general somatic sensory fibers.
Origin and Nuclei
The vagus has four associated nuclei in the medulla oblongata:
| Nucleus | Fiber Type | Function |
|---|---|---|
| Dorsal motor nucleus of CN X | Parasympathetic preganglionic | Heart, lungs, GI tract to splenic flexure |
| Nucleus ambiguus | Branchial motor | Pharynx, larynx, soft palate, upper esophagus |
| Nucleus solitarius | Visceral sensory (afferent) | Taste from epiglottis/palate, visceral sensation |
| Spinal trigeminal nucleus | General somatic sensory | Skin near external auditory meatus (Arnold's nerve) |
The dorsal motor nucleus sits on the floor of the fourth ventricle forming the "vagal trigone," just lateral to the hypoglossal trigone near the obex. The nucleus ambiguus lies in the reticular formation of the medulla, medial to the spinal trigeminal tract. - Localization in Clinical Neurology, 8e, p. 867; Neuroanatomy through Clinical Cases 3rd Edition
Ganglia
Two sensory ganglia sit on the nerve as it exits the jugular foramen:
- Superior (jugular) ganglion - cell bodies for general somatic afferents (meningeal and auricular branches), derived from neural crest
- Inferior (nodose) ganglion - cell bodies for general visceral afferents and taste from the epiglottis, derived from placodal cells
Course
The vagus exits the ventrolateral medulla as multiple rootlets just below CN IX (between the inferior olive and inferior cerebellar peduncle), crosses the subarachnoid space, and exits the skull through the jugular foramen together with CNs IX and XI. It then runs posteriorly in the carotid sheath, between the internal jugular vein (laterally) and the common carotid artery (medially). - Scott-Brown's Otorhinolaryngology, p. 602
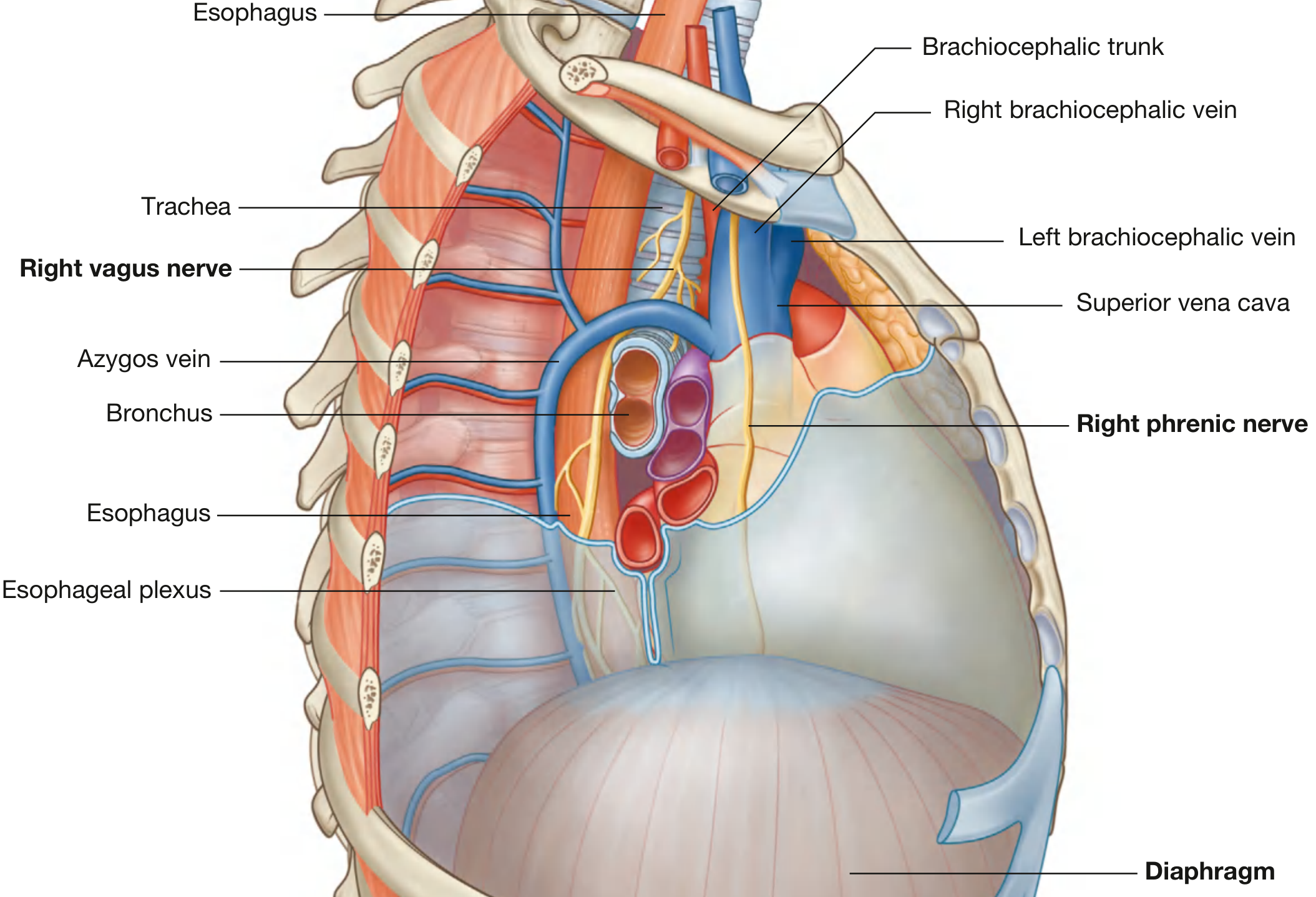
Right vs. Left Course in the Thorax
Right vagus nerve enters the superior mediastinum between the right brachiocephalic vein and brachiocephalic trunk, crosses the lateral surface of the trachea, is crossed by the arch of the azygos vein, and reaches the esophagus posteriorly.
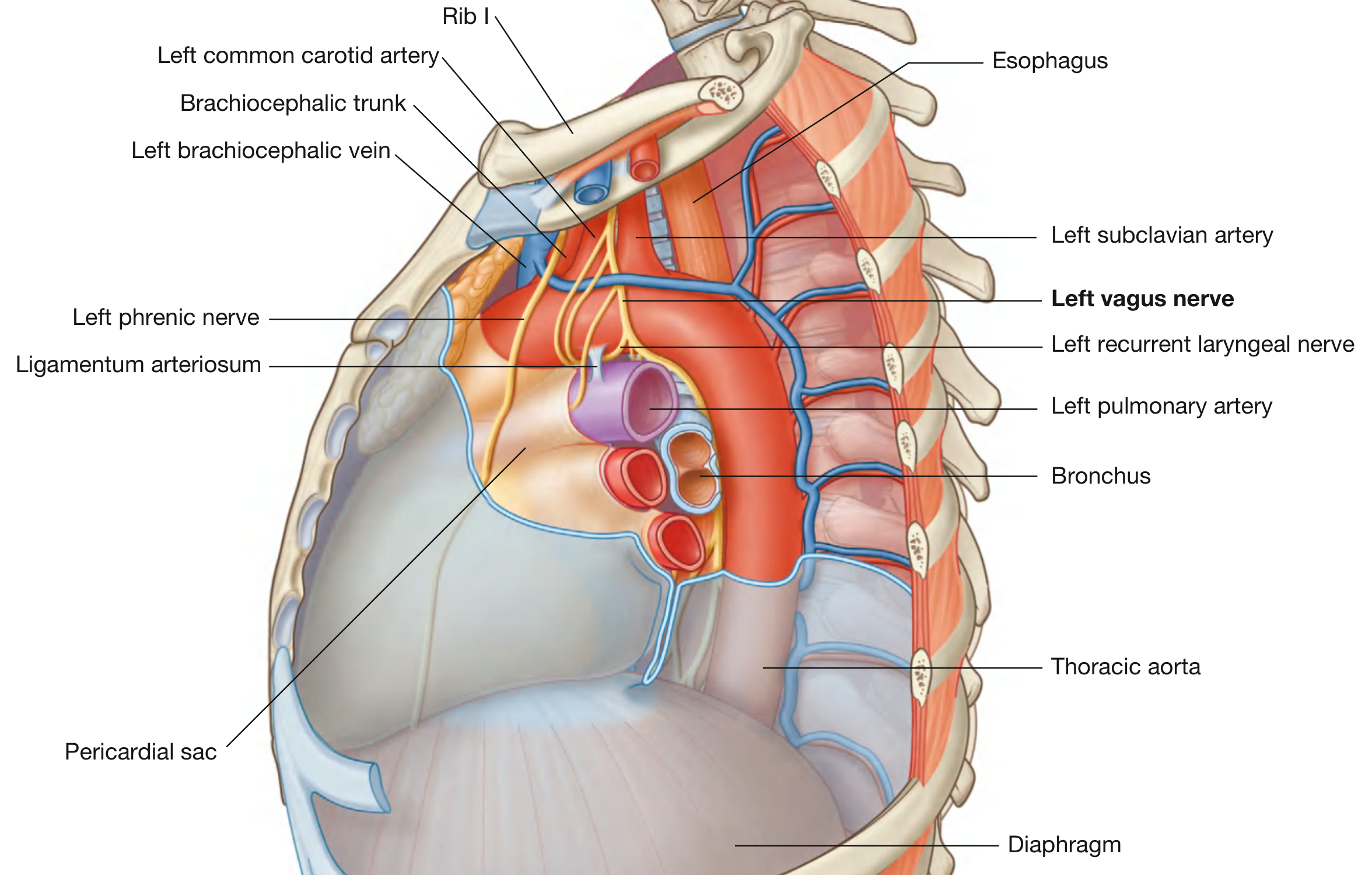
Left vagus nerve enters posterior to the left brachiocephalic vein, between the left common carotid and left subclavian arteries, crosses the arch of the aorta (where it gives off the left recurrent laryngeal nerve), and reaches the esophagus posterior to the root of the left lung.
Both vagal trunks form the esophageal plexus in the posterior mediastinum and enter the abdomen through the esophageal hiatus (left nerve anterior, right nerve posterior). - Gray's Anatomy for Students
Branches and Their Functions
In the Neck
-
Auricular branch (Arnold's nerve) - passes between the mastoid and tympanic plate; provides sensory supply to the tympanic membrane, posterior pinna, and posterior external auditory canal. Stimulating this nerve (e.g., syringing the ear) can trigger cough or even bradycardia (Arnold's reflex).
-
Pharyngeal branches - join the pharyngeal plexus with CN IX and the sympathetic trunk to provide motor innervation to the pharyngeal constrictors and soft palate.
-
Superior laryngeal nerve - divides into two branches at the level of the hyoid:
- Internal laryngeal nerve - sensory to the laryngeal and piriform fossa mucosa above the vocal folds; penetrates the thyrohyoid membrane
- External laryngeal nerve - motor to the cricothyroid muscle (the only intrinsic laryngeal muscle it supplies; all others come from the recurrent laryngeal nerve)
-
Cardiac branches - leave low in the neck to contribute to the cardiac plexus (parasympathetic slowing of heart rate).
-
Carotid body branches - supplement the CN IX supply to the carotid body chemoreceptors.
Recurrent Laryngeal Nerve (RLN)
The RLN has an asymmetric course due to embryological development:
- Right RLN: loops around the right subclavian artery (artery of the 4th arch on the right); takes a more direct, shorter course; in ~1% of individuals it is non-recurrent
- Left RLN: loops around the arch of the aorta and ligamentum arteriosum (persistent ductus arteriosus = left 6th arch artery), ascending in the tracheo-oesophageal groove
The RLN supplies all intrinsic laryngeal muscles except cricothyroid and sensory innervation to the laryngeal mucosa below the vocal folds. Its relationship to the inferior thyroid artery is variable, making it vulnerable during thyroid surgery - it may pass deep to, superficial to, or between the artery's branches. Beahr's triangle (bounded by the common carotid artery laterally, and the inferior thyroid vessels and RLN) is a key surgical landmark. - Scott-Brown's Otorhinolaryngology, p. 602
Functions Summary
| System | Vagal Action |
|---|---|
| Heart | Slows heart rate (SA node), slows AV conduction |
| Lungs | Bronchoconstriction, increases secretions |
| GI tract | Stimulates peristalsis, increases secretions; extends to the splenic flexure |
| Pharynx/larynx | Motor control for swallowing and phonation |
| Soft palate | Elevation (palatoglossus, levator veli palatini) |
| Esophagus | Upper esophageal motor control |
| Visceral sensation | Transmits physiological reflex information (not pain) |
| Taste | From epiglottis, pharynx, and hard/soft palate |
The vagal visceral afferents relay information about normal physiological processes and reflex activities - they do not transmit pain sensation. - Gray's Anatomy for Students
The parasympathetic supply does not extend below the splenic flexure; the descending colon, sigmoid, rectum, and urogenital organs are served by the sacral parasympathetics (S2-S4). - Neuroanatomy through Clinical Cases
Clinical Correlations
Unilateral Vagal Lesion
- Ipsilateral flattening of the palatal arch
- With phonation: ipsilateral palate fails to elevate; uvula deviates toward the non-paralyzed (normal) side
- Hoarseness (ipsilateral vocal cord palsy)
- Dysphagia and "nasal twang" to voice
- Loss of gag reflex on ipsilateral side
- Localization in Clinical Neurology, 8e, p. 868
Bilateral Vagal Damage
- Severe dysphagia and aspiration risk
- Cardiac irregularities
Recurrent Laryngeal Nerve Injury
- Most commonly damaged in thyroid/parathyroid surgery, esophageal surgery, or by apical lung tumors and mediastinal lymphadenopathy
- Causes hoarseness (unilateral) or respiratory distress (bilateral)
- Left RLN is more commonly affected by thoracic pathology (aortic aneurysm, Pancoast tumors, lymphoma)
Referred Otalgia
- Chest neoplasms can cause referred ear pain via infiltration of vagal branches connected through the trigeminal nuclear system to Arnold's nerve. - Bradley and Daroff's Neurology
Vasovagal Syncope
- Excessive vagal activation slows the heart and reduces blood pressure, causing transient loss of consciousness.
Hiccup (Singultus)
- Involves a reflex arc partly mediated by the vagus.
Vagus Nerve Stimulation (VNS)
VNS is an established neuromodulation therapy. A device is implanted to deliver electrical pulses to the left vagus nerve in the neck. Approved uses include:
- Refractory epilepsy (FDA-approved)
- Treatment-resistant depression
- Investigational use in inflammatory conditions, cluster headaches, and heart failure
The left vagus is chosen over the right to avoid cardiac effects, since the right vagus has more direct cardiac innervation (right vagal fibers preferentially reach the SA node). - Bradley and Daroff's Neurology in Clinical Practice
Sources used: Gray's Anatomy for Students, Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Localization in Clinical Neurology 8e, Neuroanatomy through Clinical Cases 3rd Edition, Bradley and Daroff's Neurology in Clinical Practice, Medical Physiology (Boron & Boulpaep)
This is a shared conversation. Sign in to Orris to start your own chat.