Brain hemangioblastoma imaging
Reading File
Finding Sources
Searching PubMed
hemangioblastoma brain MRI imaging
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Finding Sources
Reading File
Searching the Web
hemangioblastoma brain MRI imaging features CT angiography 2024
Reading Web Page
https://www.ncbi.nlm.nih.gov/books/NBK606126
Finding Sources
Reading File
Now I have comprehensive information from multiple authoritative sources. Let me compile the full answer.
Brain Hemangioblastoma - Imaging
Overview
Hemangioblastomas are benign (WHO Grade I) highly vascular tumors of uncertain histogenesis. They are the most common primary cerebellar neoplasm in adults, with peak incidence at age 40. About 10-20% are associated with von Hippel-Lindau (VHL) disease; the remainder are sporadic. Males are more commonly affected.
Anatomical Distribution
| Location | Frequency | Notes |
|---|---|---|
| Cerebellum | ~60% | Most common site; often hemisphere |
| Spinal cord | ~30% | Posterior columns; frequently associated with syringomyelia (>70%) |
| Brainstem / medulla | ~5-10% | Less common |
| Supratentorial | ~2-10% | Rare variant |
| Retina | Variable | More common with VHL |
MRI - The Preferred Modality
MRI is the gold standard for evaluation due to detailed soft tissue characterization.
Classic Pattern: Cyst with Mural Nodule (~60% of cases)
The hallmark appearance is a large, well-demarcated cyst with a small, intensely enhancing mural nodule along the cyst wall.
| Sequence | Cyst | Mural Nodule |
|---|---|---|
| T1 (unenhanced) | Hypointense (follows CSF) | Iso- to hypointense |
| T2 | Markedly hyperintense | Variable; may show flow voids (large feeding vessels) |
| FLAIR | Hyperintense (protein content slightly > CSF) | - |
| Post-Gd T1 | Cyst wall does NOT enhance | Intense, homogeneous enhancement |
| DWI | No restriction | No restriction (unlike metastasis) |
Key point: The non-enhancing cyst wall helps distinguish hemangioblastoma from a pilocytic astrocytoma, in which the cyst wall may enhance.
Solid Variant (~40%)
In solid tumors (more common with VHL and spinal/brainstem location):
- T1: Iso- to hypointense
- T2: Hyperintense with prominent flow voids (tortuous feeding/draining vessels - a distinguishing feature)
- Post-Gd T1: Avid, homogeneous enhancement
Advanced MRI Features
- Flow voids: Prominent serpiginous signal voids on T2 around or within the nodule, reflecting the tumor's rich arterial supply and enlarged draining veins - highly characteristic
- Peritumoral edema: Present but often less than expected for tumor size
- Hemorrhage: May occur; T1 hyperintensity if subacute blood
- MR Spectroscopy: Elevated choline, reduced NAA; high lipid peak (from lipid-laden stromal cells)
- DSC Perfusion: Very high rCBV reflecting hypervascularity
CT Findings
| Feature | Finding |
|---|---|
| Unenhanced | Mural nodule isodense to brain; cyst fluid hypodense |
| Enhanced | Mural nodule shows intense homogeneous enhancement |
| Cyst wall | Does NOT enhance |
| Calcification | Absent (helps distinguish from craniopharyngioma) |
| Bone | No erosion |
Angiography / DSA
Conventional angiography shows the tumor's characteristically prominent vascularity:
- Enlarged feeding arteries (usually from posterior inferior cerebellar artery / PICA or superior cerebellar artery)
- Dense tumor blush in the arterial phase
- Dilated draining veins
- Cluster of small vessels forming a compact mass 1-2 cm in diameter
This is important for pre-operative embolization planning.
MRI Table Summary (from Bradley and Daroff's Neurology in Clinical Practice)
| Feature | Hemangioblastoma |
|---|---|
| Typical location | Posterior fossa, cystic with mural nodule |
| T1 signal | Hypointense (cyst); variable nodule |
| T2 signal | Hyperintense (cyst); flow voids near nodule |
| Enhancement | Intense nodule enhancement; no cyst wall enhancement |
Imaging from Adams and Victor's Neurology
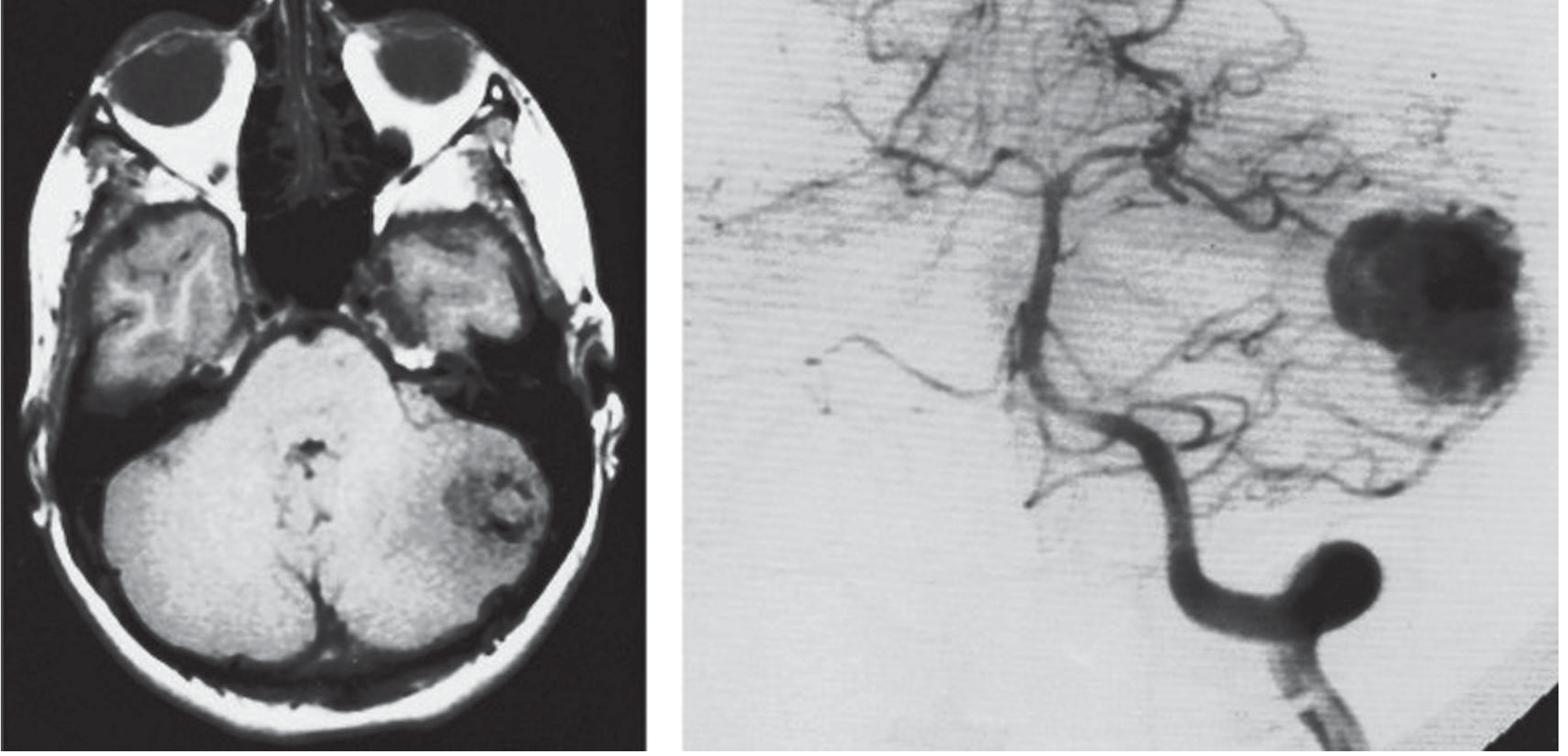
Hemangioblastoma. Left: Contrast-enhanced MRI (axial) showing the vascular tumor in the left cerebellar hemisphere. Right: Selective left vertebral angiogram showing the hypervascular nodule with dilated draining veins.
VHL-Associated vs. Sporadic
| Feature | VHL-associated | Sporadic |
|---|---|---|
| Age at onset | Earlier (20s-30s) | Peak ~40 years |
| Multiplicity | Multiple lesions common | Usually solitary |
| Locations | Cerebellum, spine, retina, brainstem | Mainly cerebellum |
| Recurrence | High; new lesions form | Low after complete resection |
| Associated findings | Renal cell carcinoma, pheochromocytoma, pancreatic cysts | None |
In VHL patients, surveillance MRI of the entire neuraxis is essential as new lesions develop over time.
Differential Diagnosis on Imaging
| Diagnosis | Key differentiating features |
|---|---|
| Pilocytic astrocytoma | Younger age; cyst wall may enhance; lower vascularity |
| Metastasis | Usually supratentorial; ring enhancement; clinical history; DWI may show restriction in necrotic center |
| Medulloblastoma | Children; midline/vermis; restricted diffusion on DWI; hyperdense on CT |
| Ependymoma | 4th ventricle; "plastic" extension through foramina; ependymal origin |
| AVM | No solid enhancing nodule; flow voids predominate; no cystic component |
| Renal cell carcinoma metastasis | Critical to exclude in VHL; may look identical - use inhibin/brachyury IHC on pathology |
| Abscess | Ring-enhancing; DWI restriction inside; clinical sepsis |
Key Imaging Pearls
- Cyst wall non-enhancement is characteristic - if the cyst wall enhances, favor pilocytic astrocytoma or metastasis
- Flow voids on T2 around the mural nodule are pathognomonic of the tumor's hypervascularity
- The nodule is the tumor - the cyst is reactive; surgical resection of the nodule alone (leaving the cyst wall) is curative
- In VHL, always image the full spine - spinal hemangioblastomas frequently cause syringomyelia
- No calcification on CT - presence of calcium suggests an alternative diagnosis
Sources: Bradley and Daroff's Neurology in Clinical Practice; Adams and Victor's Principles of Neurology, 12th Ed.; Schwartz's Principles of Surgery, 11th Ed.; StatPearls - Hemangioblastoma (2024)
Why epidermoid cyst commonly occurs in cp angle region logic ?
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is the full logical explanation:
Why Epidermoid Cysts Commonly Occur in the CP Angle - The Logic
Step 1 - The Root Cause: Ectodermal Inclusion During Neural Tube Closure
The entire story starts in the 3rd-5th week of embryonic development when the neural plate folds inward to form the neural tube (neurulation). During this process:
- Surface ectoderm (which will become skin) must separate cleanly from the neuroectoderm (which will become the brain/spinal cord)
- This separation happens as the neural folds fuse together
If small nests of ectodermal cells get pinched off and trapped inside the developing CNS during this fusion, they are carried along into the subarachnoid space. These misplaced cells retain their normal behavior - they continue to shed keratin and desquamate - and slowly accumulate into an epidermoid cyst.
"The cause of the congenital type is inclusion of ectodermal tissue during embryonic closure of the neural groove or during coalescence of epithelial fusion lines in the cranium." - Bradley and Daroff's Neurology in Clinical Practice
Step 2 - Why the CP Angle Specifically?
The cerebellopontine angle is a natural predilection site for THREE converging anatomical/embryological reasons:
Reason 1: It is a Complex Epithelial Fusion Zone
The CP angle region lies at the junction of:
- The rhombencephalon (future pons + cerebellum)
- The developing skull base (petrous temporal bone)
- Multiple cranial nerve exit points (V, VII, VIII)
During embryogenesis, this region requires the fusion of multiple epithelial planes simultaneously - the neural folds, the surface ectoderm, and the notochordal derivatives of the skull base. More fusion lines = more opportunity for ectodermal cells to be misincorporated.
Reason 2: The "Eccentric" / Off-Midline Principle
There is a fundamental anatomical rule distinguishing epidermoids from dermoids:
| Lesion | Embryological origin | Location |
|---|---|---|
| Epidermoid | Inclusion of epidermal ectoderm only (surface epithelium) | Eccentric / off-midline (CP angle, middle cranial fossa, Sylvian fissure) |
| Dermoid | Inclusion of cutaneous ectoderm (full skin elements: hair, glands) | Midline (vermis, sellar, frontonasal) |
Epidermoid inclusions occur along the lateral neural tube closure lines - which are off-midline. The CP angle, being a lateral posterior fossa recess, is exactly where these lateral ectopic rests deposit. This is why the CP angle accounts for 40-50% of all intracranial epidermoids.
"Epidermoid cysts can be central (chiasmatic and quadrigeminal cisterns) or eccentric (cerebellopontine angle, middle cranial fossa, Sylvian fissure)." - Grainger & Allison's Diagnostic Radiology
Reason 3: Passive Accumulation in a Spacious Cistern
Once trapped cells are deposited, the lesion only grows if there is space. The CP angle cistern is:
- A large, open subarachnoid CSF cistern
- Without significant parenchymal resistance
- Rich in CSF flow that does not wash away the accumulated keratin
Epidermoids grow extremely slowly by accumulating desquamated keratin and they conform to the shape of the subarachnoid space they occupy, wrapping around cranial nerves and vessels. The capacious CP angle cistern allows this passive, years-long accumulation to proceed without causing symptoms until the cyst is very large.
Summary of the Logic Chain
Neural tube closure (week 3-5)
↓
Multiple epithelial fusion planes converge laterally
↓
Ectodermal cells pinched off → misplaced in subarachnoid space
↓
Preferentially at LATERAL fusion lines → CP angle / middle cranial fossa
↓
Large open cistern allows slow, silent growth for decades
↓
Presents in adulthood (epidermoid grows ~1 mm/year)
Why Not the Midline? (The Dermoid Contrast)
Dermoids form at midline fusion lines (e.g., the neural groove closing in the midline posteriorly), where cutaneous ectoderm with full dermal appendages gets incorporated. This is why dermoids go to the cerebellar vermis, fourth ventricle, and sellar region - the midline structures. Epidermoids, trapping only flat surface epithelium at lateral closure sites, end up in the CP angle.
Bonus: Why CP Angle > Parasellar for Epidermoids?
The CP angle tends to dominate because:
- The rhomboencephalic flexure creates an especially complex folding geometry at this location
- The petrous bone develops from multiple ossification centres meeting here, creating additional epithelial interfaces
- It is the most spacious lateral posterior fossa cistern, allowing the largest accumulation before symptoms appear
Sources: Bradley and Daroff's Neurology in Clinical Practice; Grainger & Allison's Diagnostic Radiology; Bradley and Daroff's Neurology (Epidermoid and Dermoid Cysts section)
This is a shared conversation. Sign in to Orris to start your own chat.