pneumoniae pathology
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Pneumonia pathology, in exam-style summary:
Core definition
Pneumonia is acute infection of lung parenchyma causing inflammation and alveolar air-space filling (consolidation).
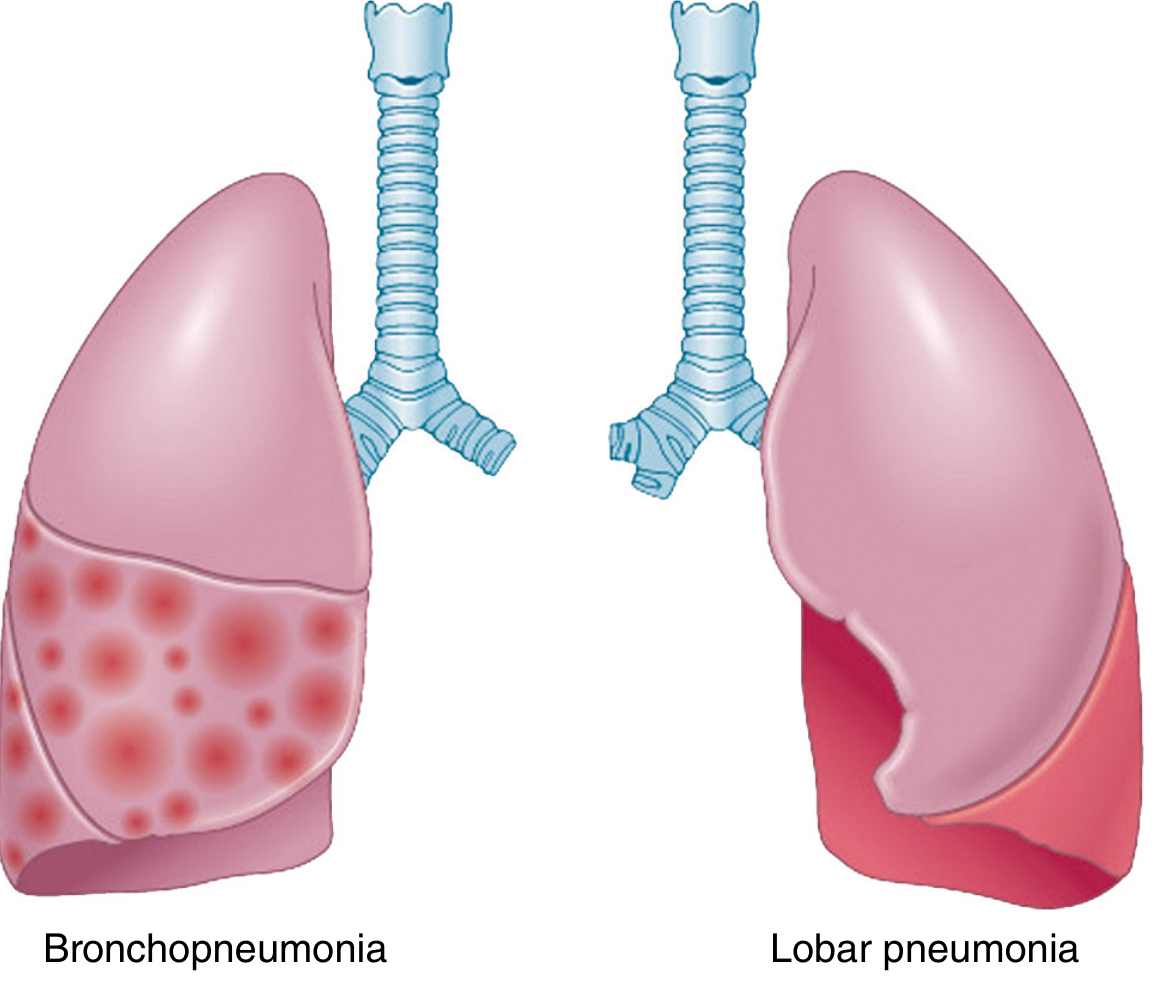
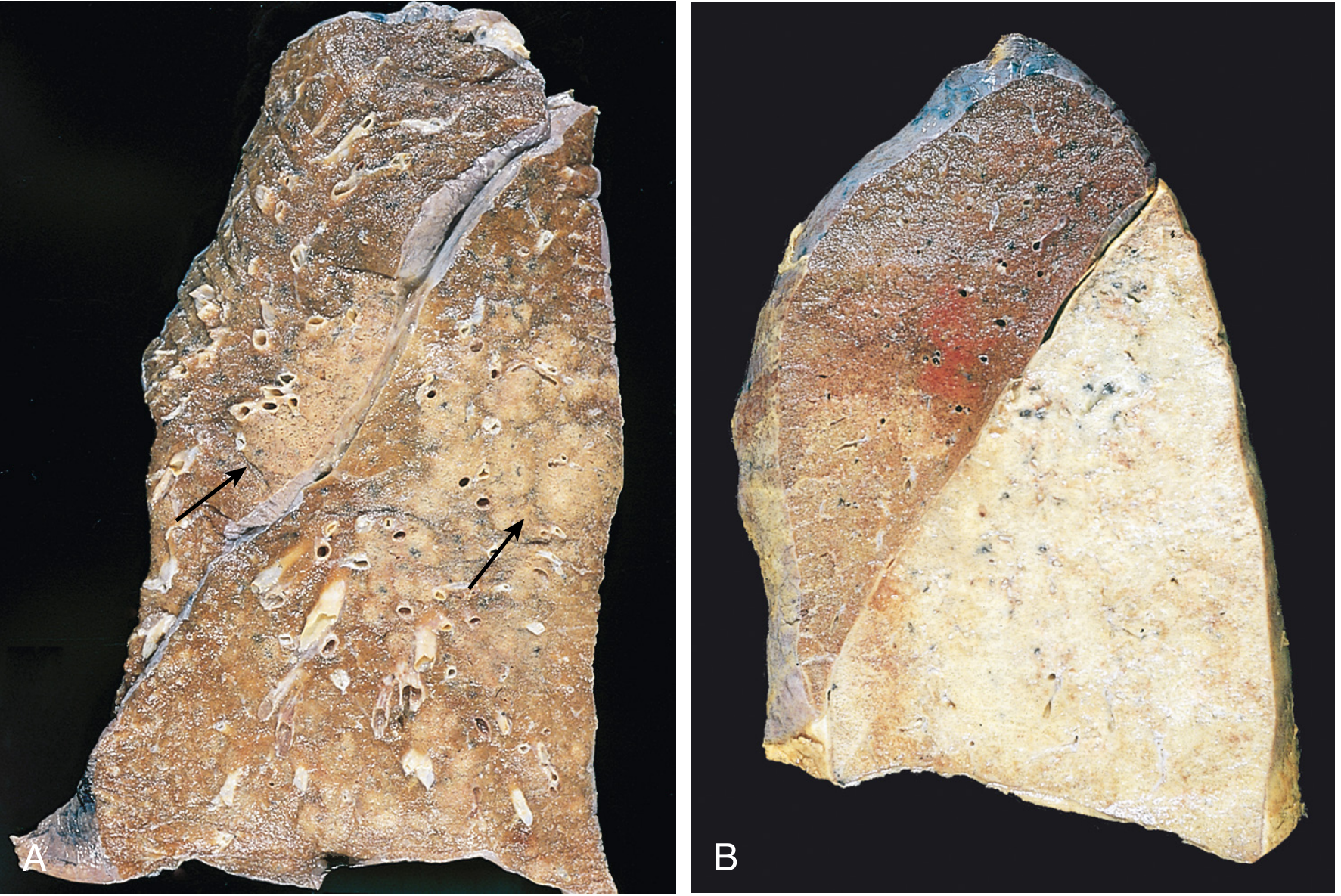
Main morphologic patterns (bacterial)
-
Bronchopneumonia (lobular, patchy)
- Patchy, often multilobar, commonly bilateral and basal consolidation
- Centered on bronchi/bronchioles with spread to adjacent alveoli
- Histology: neutrophil-rich suppurative exudate in bronchi, bronchioles, and alveolar spaces
-
Lobar pneumonia
- Confluent consolidation of a large part of a lobe or an entire lobe
- Classic sequence of 4 stages:
- Congestion: heavy, boggy, red lung; vascular engorgement, edema, few neutrophils
- Red hepatization: alveoli packed with neutrophils, RBCs, fibrin; firm “liver-like” lung
- Gray hepatization: RBC breakdown with persistent fibrinopurulent exudate; gray-brown color
- Resolution: enzymatic digestion and clearance of intraalveolar exudate (macrophage removal, expectoration, resorption; sometimes organization)
Viral pneumonia pathology
- Predominantly interstitial inflammation (alveolar septal widening/edema)
- Mononuclear infiltrate (lymphocytes, macrophages, occasional plasma cells)
- Alveoli may be relatively free early, then proteinaceous/cellular exudate may appear
- Severe injury can show diffuse alveolar damage with hyaline membranes (ARDS pattern)
- Superadded bacterial infection shifts to mixed or neutrophilic suppurative pattern
Common complications
- Lung abscess/necrosis
- Empyema (fibrinopurulent pleural involvement)
- Bacteremic spread causing metastatic infection (e.g., endocarditis, meningitis, brain/kidney/splenic abscesses)
- Pleural fibrosis/adhesions after organization
Etiology-pathology associations (high yield)
- S. pneumoniae: most common CAP; often lobar pattern
- Staph/Klebsiella/Pseudomonas: often severe necrotizing or suppurative disease in high-risk hosts
- Aspiration pneumonia: often polymicrobial, frequently necrotizing, abscess-prone
Source: Robbins, Cotran & Kumar Pathologic Basis of Disease, Ch. Lung infections (pp. 662–665 equivalent block lines).
This is a shared conversation. Sign in to Orris to start your own chat.