CKD mbd details, take reference from standard textbook
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive data from multiple standard textbooks. Let me compile the full detailed answer:
CKD-MBD (Chronic Kidney Disease - Mineral and Bone Disorder)
Primary references: Brenner & Rector's The Kidney (2-Volume Set), National Kidney Foundation Primer on Kidney Diseases (8th Ed), Comprehensive Clinical Nephrology (7th Ed), Tietz Textbook of Laboratory Medicine (7th Ed)
1. Definition (KDIGO, 2006)
CKD-MBD is a systemic disorder of mineral and bone metabolism due to CKD, manifested by one or a combination of the following:
| Component | Description |
|---|---|
| Biochemical | Abnormalities of calcium, phosphorus, PTH, or vitamin D metabolism |
| Skeletal | Abnormalities in bone turnover, mineralization, volume, linear growth, or strength |
| Extraskeletal | Vascular or other soft tissue calcification |
Renal Osteodystrophy is the skeletal component only - an alteration of bone morphology in CKD patients, quantifiable by histomorphometry of bone biopsy. It is one measure of the broader CKD-MBD syndrome.
- Brenner & Rector's The Kidney, Table 53.1
2. Pathophysiology
Normal Mineral Homeostasis
Serum phosphorus (2.5-4.5 mg/dL) and calcium are maintained through interaction of three hormones acting on four target organs (bone, kidney, intestine, parathyroid glands):
- PTH (parathyroid hormone)
- Calcitriol [1,25(OH)₂D₃] - active vitamin D
- FGF-23 (fibroblast growth factor 23)
- Klotho (co-receptor/circulating factor)
Sequence of Events in CKD
Early CKD (Stage 3-4) - Compensatory phase:
- Reduced renal mass → decreased phosphate excretion → mild phosphate retention
- Declining renal mass → reduced 1α-hydroxylase activity → decreased calcitriol synthesis
- Low calcitriol + hyperphosphatemia → hypocalcemia (reduced intestinal Ca²⁺ absorption)
- Bone secretes FGF-23 (earliest detectable change) → phosphaturia via downregulation of NaPi-IIa transporters; also inhibits calcitriol synthesis
- PTH rises (secondary hyperparathyroidism) → increases phosphaturia + bone resorption
- Together PTH and FGF-23 maintain near-normal serum phosphorus in stages 3-4
Late CKD (Stage 4-5D) - Decompensation:
- GFR <30 mL/min → compensatory mechanisms fail
- Hyperphosphatemia develops; hypocalcemia worsens
- Secondary hyperparathyroidism (2°HPT) becomes severe
- Parathyroid glands develop nodular hyperplasia, decreased VDR expression, decreased CaSR expression, decreased klotho expression - making them resistant to calcitriol and calcimimetic therapies (tertiary hyperparathyroidism)
- Vascular calcification and extraskeletal calcification ensue
The FGF-23/Klotho Axis (Key)
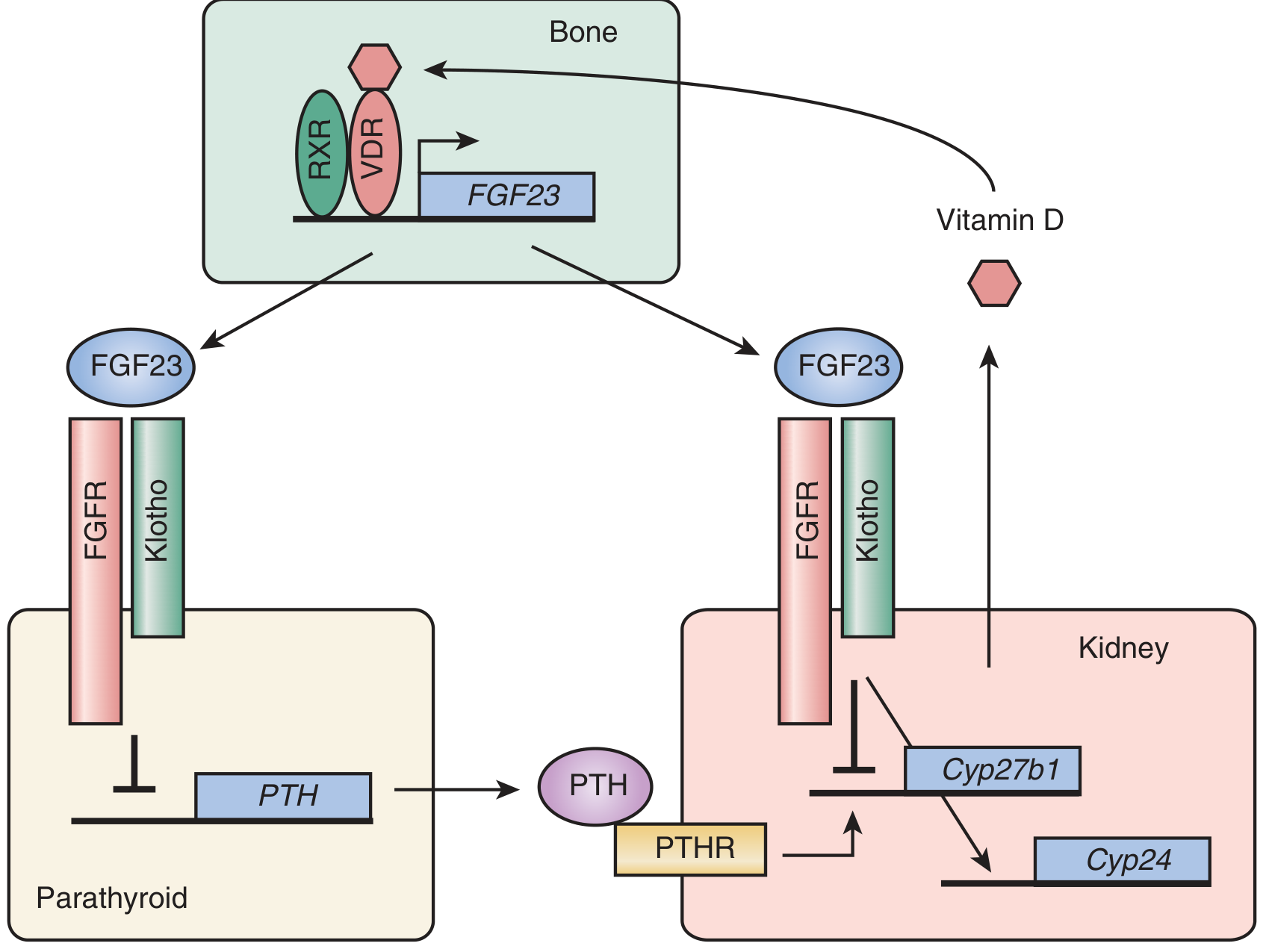
FGF-23 is produced by osteocytes and osteoblasts during active bone remodeling. It:
- Acts on kidney via the FGFR-Klotho co-receptor complex
- Inhibits Cyp27b1 (↓ calcitriol synthesis)
- Upregulates Cyp24 (↑ calcitriol catabolism)
- Suppresses PTH gene expression
In CKD, klotho expression is reduced, impairing FGF-23 signaling and contributing to phosphate retention. α-Klotho is expressed in kidney and parathyroid glands.
- Brenner & Rector's The Kidney, p. 2395
Parathyroid Gland Abnormalities in CKD (Box 88.1)
-
Parathyroid gland hyperplasia: diffuse, then nodular (monoclonal expansion)
-
Decreased expression of vitamin D receptors (VDR)
-
Decreased expression of calcium-sensing receptors (CaSR)
-
Decreased expression of α-klotho
-
Increased set-point of calcium-regulated PTH secretion
-
Comprehensive Clinical Nephrology, 7th Ed, Box 88.1
3. Biochemical Abnormalities
| Parameter | Change in CKD | Clinical Significance |
|---|---|---|
| Phosphorus | ↑ (hyperphosphatemia) | Stimulates PTH; vascular calcification risk |
| Calcium | ↓ (hypocalcemia) in later stages | Drives 2°HPT |
| PTH | ↑↑ (secondary, tertiary HPT) | Bone resorption, cardiovascular risk |
| Calcitriol [1,25(OH)₂D] | ↓↓ | Reduced gut Ca absorption; worsens HPT |
| 25(OH)D | Often ↓ | Substrate deficiency |
| FGF-23 | ↑↑ (rises earliest in CKD) | Phosphaturia, ↓calcitriol; cardiac hypertrophy |
| Klotho | ↓ | Impaired FGF-23 signaling |
Serum calcium and phosphate levels are usually normal in mild-moderate CKD. Hypercalcemia may occur with excessive calcium binders or vitamin D analogues.
- Comprehensive Clinical Nephrology, 7th Ed, Chapter 88
4. Renal Osteodystrophy: Histologic Classification
The KDIGO TMV system (Turnover, Mineralization, Volume) is the current recommended classification. Traditional categories remain clinically useful:
A. High-Turnover Bone Disease
1. Osteitis Fibrosa (Osteitis Fibrosa Cystica) - Most common form
- Caused by excess PTH (secondary hyperparathyroidism)
- Histology: Increased osteoclasts + osteoblasts; dissecting lacunae; peritrabecular fibrosis; woven (disorganized) collagen; "brown tumors" in severe disease
- Radiology: Subperiosteal erosions (radial aspect of middle phalanges - pathognomonic), "Rugger-jersey spine," "Pepper-pot skull," resorption of terminal digits, distal clavicle erosion
- Mechanism: Excess PTH → increased bone resorption → fibrous tissue replaces bone marrow
2. Mixed Uremic Osteodystrophy
- Features of both osteitis fibrosa AND osteomalacia
- Increased osteoid with features of hyperparathyroidism
- May represent a normal response to increased turnover rather than a distinct entity
B. Low-Turnover Bone Disease
3. Osteomalacia
- Histology: Excessive unmineralized osteoid (wide osteoid seams); prolonged mineralization lag time; absent cellular activity
- Causes: Vitamin D deficiency (↓ calcitriol synthesis in CKD), aluminum toxicity (historically major cause - aluminum from dialysate or Al-containing antacids)
- Aluminum deposits at the mineralization front (detected by special staining)
- Aluminum disease is less common today due to improved dialysate purification
4. Adynamic (Aplastic) Bone Disease
-
Histology: Near-total absence of osteoblast and osteoclast activity; minimal osteoid; no fibrosis
-
Essentially a disorder of decreased bone formation
-
Osteoid is normal or low (distinguishes from osteomalacia)
-
Causes: Calcium supplementation, excessive vitamin D, overtreatment of hyperparathyroidism (calcimimetics, calcitriol), diabetes, corticosteroids, advanced age, immobilization
-
Epidemiology: More common in White vs. Black ESKD patients; may be a consequence of overtreatment of 2°HPT
-
Risk: Fractures AND vascular calcification (adynamic bone cannot buffer calcium-phosphate load)
-
Brenner & Rector's The Kidney, p. 2403; National Kidney Foundation Primer, 8th Ed, p. 557
5. Clinical Manifestations
Musculoskeletal
- Bone pain: Lower back, hips, legs; aggravated by weight-bearing
- Fractures: 4.4-fold increased hip fracture risk in dialysis vs. general population; both high AND low PTH levels increase fracture risk
- Muscle weakness: Gradual onset; involves hyperparathyroidism + vitamin D deficiency
- Periarticular pain/acute arthritis: Due to calcium-phosphate crystal deposition; mimics gout/pseudogout
- Growth retardation: In children; slipped epiphysis
- Brown tumors: Localized, lytic bone lesions from osteoclast activity in severe osteitis fibrosa
Extraskeletal (Cardiovascular)
- Vascular calcification - Two patterns:
- Intimal (atherosclerotic): Focal calcification in plaques - increases plaque fragility
- Medial (Mönckeberg sclerosis): Diffuse, non-atherosclerotic; increases vascular stiffness, pulse pressure, cardiac afterload → LVH
- Cardiac valve calcification
- Calciphylaxis (Calcific Uremic Arteriolopathy): Rare but devastating; skin necrosis from small vessel calcification
- Pruritus: From skin calcium-phosphate deposition
CVD accounts for approximately half of all deaths in dialysis patients. Coronary artery calcification can be documented in dialysis patients before 30 years of age.
- National Kidney Foundation Primer, 8th Ed
6. Vascular Calcification - Inhibitors and Promoters
Normally, calcification is actively inhibited:
| Inhibitor | Mechanism |
|---|---|
| Fetuin-A | Binds Ca and Pi → forms "calciparticles" removed by reticuloendothelial system; reverse acute-phase reactant |
| Matrix Gla Protein (MGP) | Locally produced; inhibits calcification at arterial sites |
| Osteoprotegerin (OPG) | RANK-L decoy receptor; also inhibits vascular calcification |
In CKD: promoters increase + inhibitors decrease → net calcification. VSMCs undergo phenotypic switch to osteoblast-like cells and release matrix vesicles that nucleate calcium-phosphate crystal deposition.
- Brenner & Rector's The Kidney, p. 2403
7. Diagnosis
Biochemical Monitoring (KDIGO)
- CKD Stages G3a-G5: Monitor Ca, Pi, PTH, and alkaline phosphatase
- Frequency increases with worsening CKD stage
- Use the same PTH assay serially; evaluate trends rather than absolute values
PTH Assay Generations
- 1st generation: Radioimmunoassays (unreliable, no longer used)
- 2nd generation (Intact PTH assay): Detects PTH(1-84) + large C-terminal fragments; most commonly used clinically
- 3rd generation (Whole/Bioactive PTH): Detects PTH(1-84) exclusively; uses N-terminal antibody (epitopes 1-4)
- C-terminal fragments represent ~80% of circulating PTH in healthy persons and ~95% in CKD → explains why "elevated PTH is normal in CKD"
- Brenner & Rector's The Kidney, p. 2399
Bone Biopsy (Gold Standard)
- Double tetracycline labeling required to assess dynamic bone formation rate
- Indicates quantitative histomorphometry: osteoid thickness, fibrosis, mineralization lag time
- TMV classification: Turnover (low/normal/high), Mineralization (normal/abnormal), Volume (low/normal/high)
- Required in clinical practice when: aluminum toxicity suspected; unexplained fractures; before bisphosphonate use in CKD
Radiology
- Subperiosteal erosions: radial aspect of middle phalanges (2°HPT)
- Rugger-jersey spine; pepper-pot skull
- Vascular calcification by CT or plain film
- DXA: Predicts fracture risk in CKD (as in general population)
8. Management
A. Control Serum Phosphorus
Step 1 - Dietary Restriction:
- Target: 800-1000 mg phosphorus/day
- Avoid phosphate additives (up to 100% bioavailable vs. natural food phosphate)
- Protein-phosphorus balance is challenging (malnutrition in ~50% of dialysis patients)
- More frequent/prolonged dialysis lowers phosphorus
Step 2 - Phosphate Binders (taken WITH meals):
| Binder | Notes |
|---|---|
| Calcium carbonate | 40% elemental Ca (500 mg per 1250 mg tablet); risk of hypercalcemia + vascular calcification |
| Calcium acetate | 25% elemental Ca (169 mg per 667 mg tab); greater binding capacity than CaCO₃ |
| Sevelamer HCl/carbonate | Non-calcium; ion exchange polymer; also ↓ LDL; ↓ arterial calcification vs. Ca-binders; more expensive; GI side effects |
| Lanthanum carbonate | Non-calcium, non-aluminum; highly effective; long-term safety established |
| Ferric citrate | Also treats iron deficiency anemia |
| Sucroferric oxyhydroxide | Iron-based; lower pill burden |
KDIGO cautions against excessive calcium intake from binders. Non-calcium binders preferred in patients with vascular calcification, hypercalcemia, or low PTH.
B. Vitamin D Therapy
- Nutritional vitamin D (cholecalciferol/ergocalciferol): Correct 25(OH)D deficiency first
- Active vitamin D analogues (for secondary HPT):
- Calcitriol [1,25(OH)₂D₃]: Most potent; increases GI calcium + phosphate absorption
- Paricalcitol (19-nor-1,25(OH)₂D₂): Selective VDR activator; less hypercalcemia/hyperphosphatemia risk; PRIMO study: 48 weeks did not alter cardiac mass index in CKD 3/4
- Doxercalciferol, alfacalcidol
- Active vitamin D analogues suppress PTH gene transcription; increase Ca and Pi absorption from gut (worsens hyperphosphatemia - must balance with binders)
C. Calcimimetics
- Cinacalcet (Sensipar): Allosteric activator of CaSR on parathyroid chief cells; increases receptor sensitivity to extracellular calcium → ↓ PTH secretion
- Approved for dialysis patients with secondary HPT
- Not FDA-approved for CKD stages 3-4 (limited evidence)
- Main side effects: nausea, vomiting, hypocalcemia
- EVOLVE trial: Did not significantly reduce major cardiovascular events vs. placebo in dialysis patients (intention-to-treat analysis)
- Etelcalcetide (Parsabiv): IV calcimimetic for hemodialysis patients
D. Dialysis Modifications
- More frequent dialysis (daily/nocturnal) → lower phosphorus
- Hemodiafiltration associated with better mineral control
E. Parathyroidectomy
- Indicated for: Severe, refractory 2°HPT unresponsive to medical therapy; hypercalcemia; severe symptoms
- Indications: PTH persistently >800-1000 pg/mL (varies by guideline), hypercalcemia, symptomatic bone disease
- Types: Subtotal parathyroidectomy or total parathyroidectomy + autotransplantation
- Risk of post-op "hungry bone syndrome" (severe hypocalcemia as bone rapidly reabsorbs calcium)
F. Special Considerations
Bisphosphonates in CKD:
- Generally NOT recommended for CKD stages 4-5 (eGFR <30 mL/min)
- Inhibit bone turnover → can worsen or induce adynamic bone disease
- Accumulate in bones and may cause osteonecrosis of the jaw
Post-Kidney Transplant:
- Bone loss common in first year (largely reversed with steroid minimization)
- DXA recommended at transplant and yearly
- Avascular necrosis (femoral head) is a complication, especially with corticosteroids
9. KDIGO Targets (Summary)
| Parameter | CKD Stage G3-G5D |
|---|---|
| Phosphorus | Trend toward normal range; avoid hyperphosphatemia |
| Calcium | Maintain in normal range; avoid hypercalcemia |
| PTH (Stage G5D) | 2-9× upper limit of normal for the assay used |
| Vitamin D | Correct if 25(OH)D deficient |
No clinical trial data exist demonstrating that any current CKD-MBD treatment reduces mortality. Current guidelines are based largely on observational data linking elevated phosphorus/calcium to increased mortality.
- National Kidney Foundation Primer, 8th Ed, p. 562
Key Summary Diagram
Pathophysiologic cascade:
↓ GFR → ↓ Phosphate excretion → Phosphate retention
→ ↓ 1α-hydroxylase → ↓ Calcitriol
→ ↓ Calcium absorption → Hypocalcemia
↓
↑ PTH (2° Hyperparathyroidism)
↓
High-turnover bone disease (Osteitis Fibrosa)
+ FGF-23 ↑↑ (earliest marker)
+ Vascular/Extraskeletal Calcification
+ Cardiovascular Disease & ↑ Mortality
Sources:
- Brenner & Rector's The Kidney, 2-Volume Set - Chapter 53, pp. 2388-2410
- National Kidney Foundation Primer on Kidney Diseases, 8th Ed - Chapter 53, pp. 553-565
- Comprehensive Clinical Nephrology, 7th Ed - Chapter 88
- Tietz Textbook of Laboratory Medicine, 7th Ed - Chapter on CKD-MBD
- Goodman & Gilman's Pharmacological Basis of Therapeutics - Chapter 15
Significant lymph nodes all criteria
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive data from multiple standard textbooks. Let me compile the complete, detailed answer:
Significant (Pathological) Lymph Nodes: All Criteria
References: Harrison's Principles of Internal Medicine 22E, Sabiston Textbook of Surgery, Grainger & Allison's Diagnostic Radiology, Fishman's Pulmonary Diseases, Washington Manual
Overview
A lymph node is considered significant/pathological when it deviates from normal characteristics across several parameters. No single criterion is absolute - assessment is always multiparametric. The key domains are:
- Clinical (palpation) criteria
- Size criteria (general + site-specific)
- Imaging criteria (US, CT, MRI, PET)
- Architectural/morphologic criteria
- Site-specific significance
- Extranodal extension
- RECIST criteria (oncologic follow-up)
1. Clinical Examination Criteria
Size (on palpation)
| Size | Significance |
|---|---|
| ≤1.0 cm² (1 cm × 1 cm) | Almost always benign/reactive |
| >2 cm (diameter) | High suspicion for malignant or granulomatous disease (biopsy discriminant in one study) |
| >2.25 cm² (1.5 cm × 1.5 cm) | Best size limit for distinguishing malignant/granulomatous from benign causes |
- Harrison's Principles of Internal Medicine 22E, p. 2085
Consistency / Texture
| Texture | Implication |
|---|---|
| Soft | Usually benign/reactive |
| Firm, rubbery | Lymphoma (large, discrete, symmetric, rubbery, firm, mobile, nontender) |
| Hard | Metastatic carcinoma |
| Fluctuant | Suppurative adenitis (abscess formation) |
| Matted | Multiple nodes fused together (TB, lymphoma, metastatic cancer) |
Tenderness
- Tender nodes - usually inflammatory/reactive (capsule stretched by rapid enlargement)
- Can also occur in aggressive malignancies (rapid enlargement → hemorrhage/necrosis - e.g., acute leukemia)
- Nontender nodes - more suspicious for malignancy (metastatic cancer, lymphoma)
"A mass that is tender is more likely inflammatory, whereas a mass that is fixed and nontender is more likely malignant." - Cummings Otolaryngology
Mobility / Fixation
- Mobile - benign or lymphoma
- Fixed/non-movable - metastatic cancer (fixation to surrounding tissues); also TB (periadenitis)
Warmth
-
Warm, erythematous overlying skin - acute inflammatory/infective adenitis
-
Sabiston Textbook of Surgery, p. 1593
2. Size Criteria by Imaging (CT/MRI)
General Rule
A normal lymph node measures <1 cm in its smallest (short-axis) diameter on CT/MRI. Shape is ovoid/reniform ("kidney-shaped") with a visible fatty hilum.
Site-Specific Size Thresholds (CT)
| Site | Abnormal Short-Axis Size |
|---|---|
| General / most sites | >10 mm (1 cm) short axis |
| Jugulodigastric (level II cervical) | >13 mm short axis (normal upper limit) |
| Gastrohepatic ligament / porta hepatis | >8 mm |
| Retrocrural | >6 mm |
| Pelvic (oval shape) | >10 mm short axis |
| Pelvic (round shape) | >8 mm |
| Splenic hilum, presacral, perirectal | Any visible node is likely abnormal |
| Supraclavicular / scalene | Any enlargement is abnormal |
| Mediastinal (lung cancer staging) | >1 cm short axis = potentially malignant |
Important caveat: Up to 21% of nodes <1 cm are malignant and up to 40% of nodes >1 cm are benign in mediastinal staging - highlighting the limitations of size alone.
- Grainger & Allison's Diagnostic Radiology; Fishman's Pulmonary Diseases
RECIST 1.1 Criteria (Oncologic Response Assessment)
| Parameter | Threshold |
|---|---|
| Pathological lymph node (target lesion) | >15 mm short axis on CT |
| Non-target lymph node | 10-15 mm short axis |
| Normal lymph node | <10 mm short axis |
| Complete response | All target nodes <10 mm short axis |
- Washington Manual of Medical Therapeutics
Lugano Classification (Lymphoma)
- Lymph node with longest diameter >1.5 cm = enlarged
- For FDG-avid lymphomas: a node is positive if there is abnormal FDG uptake regardless of size
3. Ultrasound (US) Criteria
Normal vs. Pathological on Ultrasound
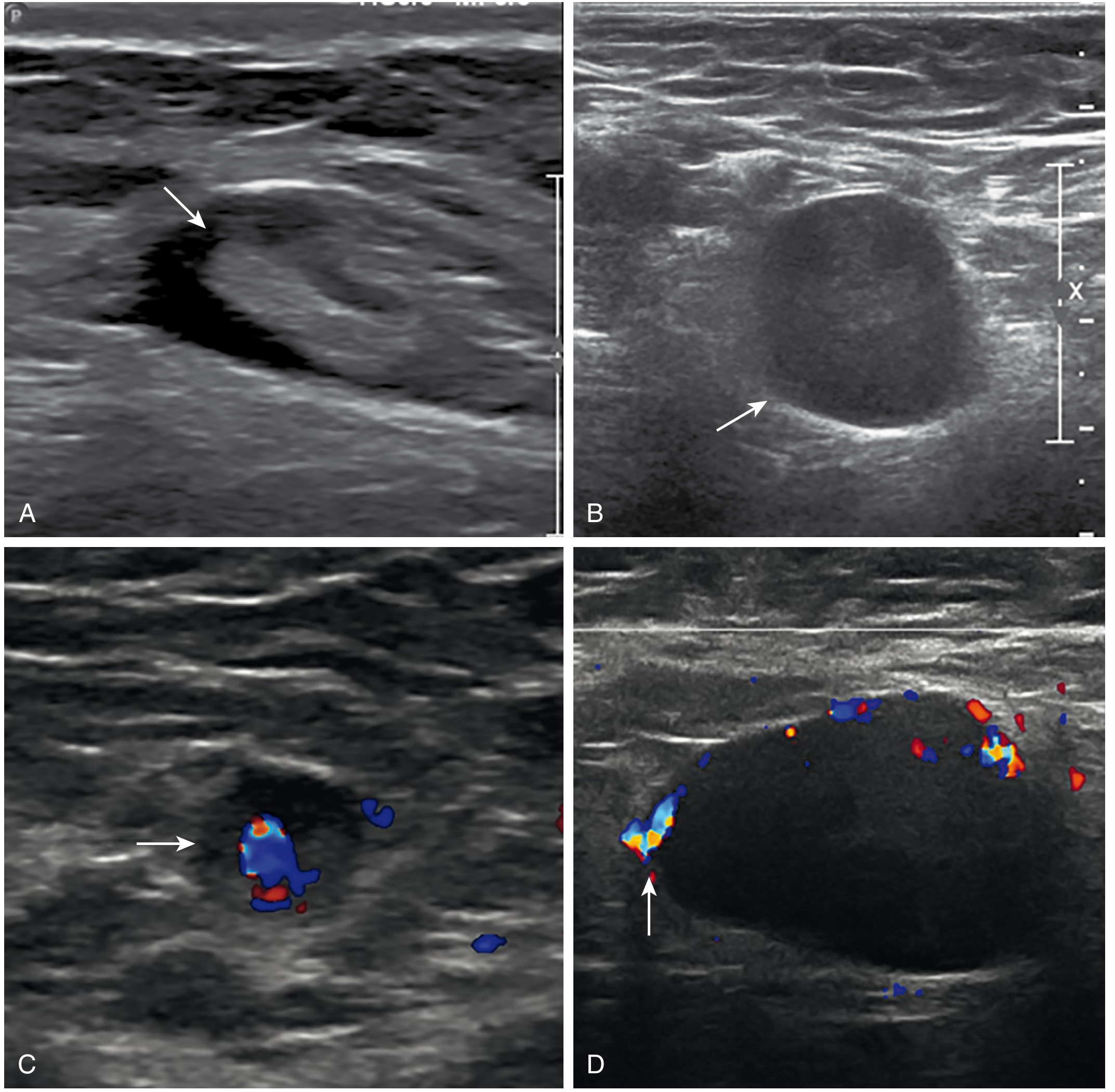
| Feature | Normal (Benign) | Pathological (Malignant) |
|---|---|---|
| Shape | Oval / reniform ("rugby ball") | Rounded ("football") |
| Long:Short axis ratio | >2 (elongated) | <2 (shape index >0.5 = rounded) |
| Short axis | <1 cm | >1 cm |
| Fatty hilum (echogenic hilum) | Present (92% of benign nodes) | Absent / lost (only 4% of malignant nodes retain it) |
| Cortex echogenicity | Hypoechoic cortex | Hypoechoic (non-specific) |
| Internal texture | Homogeneous | Necrosis or calcifications = malignant |
| Vascularity (Doppler) | Hilar flow - radial branching from hilum | Peripheral flow - around edges (tumor displaces hilar vessels) |
| Cystic change | Absent | Present - concerning (especially in HPV+ oropharyngeal SCC) |
- Sabiston Textbook of Surgery; Grainger & Allison's
4. CT / MRI Additional Features
| CT/MRI Feature | Significance |
|---|---|
| Round shape | Malignant until proven otherwise |
| Loss of fatty hilum | Tumor infiltration |
| Central necrosis / cystic center | Metastatic SCC (especially HPV+), TB, suppurative adenitis |
| Ring enhancement (after contrast) | TB lymphadenitis (caseous necrosis) |
| Calcification | Post-treatment; TB; sarcoidosis; treated lymphoma |
| Confluent/conglomerate nodes >2-3 cm | Malignant until proven otherwise (lymphoma, nodal metastasis) |
| Irregular/spiculated margins | Extranodal extension |
| Homogeneous soft-tissue density | Lymphoma |
| Heterogeneous signal (T2-MRI) | Associated with worse outcome in lymphoma |
"Abnormal lymph nodes on CT or MRI are virtually never normal from a pathologic standpoint, even if the diagnosis is not clinically significant." - Fishman's Pulmonary Diseases, p. 1887
5. PET/CT Criteria
| Parameter | Threshold / Finding |
|---|---|
| SUVmax | >2.5 = suspicious for malignancy |
| FDG-avid lymphomas | Any abnormal uptake = positive regardless of size |
| Calcified nodes | More likely benign even if FDG-avid |
| Performance | Sensitivity 79%, Specificity 91% for mediastinal nodes (vs. CT: 61%/79%) |
- Fishman's Pulmonary Diseases
6. Extranodal Extension (ENE) / Extracapsular Spread (ECS)
- Defined as extension of nodal metastases beyond the lymph node capsule
- Can be diagnosed pathologically (histology) or clinically (imaging/palpation showing clear extension)
- AJCC 8th edition: ENE automatically classifies as N3b in head and neck cancers
- Each factor (ipsilateral node, contralateral node, extracapsular spread) decreases 5-year survival by 50%
- Imaging features: irregular/infiltrative margins, loss of fat planes, matting of adjacent nodes
7. Site-Specific Significance
Supraclavicular / Scalene Nodes
- Enlargement is ALWAYS abnormal (Harrison's Principles)
- Drain: lung, retroperitoneal space, mediastinum
- Virchow's node: enlarged left supraclavicular node = metastatic GI malignancy (Troisier's sign)
- Also: lung, breast, testis, ovarian cancers; TB, sarcoidosis, toxoplasmosis
Cervical Nodes
- Most common site of lymphadenopathy; usually benign (URTI, dental, EBV)
- 7 levels (Levels I-VII) in head and neck cancer
- Level II (jugulodigastric): largest normal cervical node - upper limit 13 mm short axis
Axillary Nodes
- Benign: upper limb infections, cat-scratch disease
- Malignant: breast cancer (primary drainage), melanoma, lymphoma
Epitrochlear Nodes
- Normal: not usually palpable
- Any enlargement: sarcoidosis, secondary syphilis, lymphoma, infections of forearm/hand
- Bilateral epitrochlear adenopathy = strong indicator of systemic disease (sarcoidosis, EBV)
Inguinal Nodes
- Normal: can be palpable up to 1-2 cm (inguinal region has naturally larger normal nodes)
- Pathological: STIs (LGV, primary syphilis, genital herpes, chancroid), lymphoma, melanoma, GU/GI/GYN malignancy
Mediastinal Nodes
- Any mass-like conglomerate adenopathy is malignant until proven otherwise
- Distribution pattern aids diagnosis (lung → ipsilateral hilar/subcarinal; H&N SCC → supraclavicular; breast → axillary/internal thoracic; HCC → anterior cardiophrenic)
Intra-abdominal / Retroperitoneal Nodes
- Not normally visible on imaging
- If visible and >10 mm = pathological
- Porta hepatis/gastrohepatic: >8 mm
- Retrocrural: >6 mm
8. Summary Table: Normal vs. Significant
| Parameter | Normal | Significant/Pathological |
|---|---|---|
| Size (short axis, CT) | <10 mm | >10 mm (site-specific exceptions) |
| Shape | Oval/reniform | Rounded |
| Long:Short ratio | >2 | <2 (shape index >0.5) |
| Fatty hilum | Present | Absent |
| Consistency | Soft-firm | Hard (metastasis), rubbery (lymphoma), fluctuant (abscess) |
| Tenderness | Variable | Tender = reactive; Non-tender = malignant |
| Mobility | Mobile | Fixed = malignant/TB |
| Borders | Smooth | Irregular = ENE |
| Internal architecture | Homogeneous | Necrosis, calcification, cystic |
| Vascularity (Doppler) | Hilar flow | Peripheral flow |
| FDG uptake (PET) | Background | SUVmax >2.5 |
| Extranodal extension | Absent | Present = worsened staging |
Key Clinical Pearl
Nodes <1.0 cm² should be observed (excluding EBV/toxoplasma). Nodes >2 cm or >2.25 cm² (1.5×1.5 cm) warrant biopsy. Supraclavicular/scalene adenopathy is ALWAYS abnormal. Hard, fixed, nontender nodes suggest metastatic carcinoma; large, rubbery, discrete, bilateral nodes suggest lymphoma.
- Harrison's Principles of Internal Medicine 22E
This is a shared conversation. Sign in to Orris to start your own chat.