mmse motor system examination sensory system examination name of reflexes (where is closed refelexes of bicep , pateller) multiple sclerosis symptoms gullian barre syndrome symptoms (any 3-4 disorders ) Explain everything detail about the practical activities
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have rich, authoritative content from the textbooks. Let me compile the full detailed answer.
Neurological Practical Examination - Complete Study Guide
1. MMSE - Mini-Mental State Examination
The MMSE is the most widely used bedside screening tool to document gross changes in cognitive/mental status. It assesses multiple cognitive domains in a structured format.
Domains Tested & Maximum Scores (Total = 30 points)
| Domain | Task | Max Score |
|---|---|---|
| Orientation to Time | Year, Season, Month, Date, Day | 5 |
| Orientation to Place | Country, State, City, Hospital, Floor | 5 |
| Registration | Name 3 objects; ask patient to repeat | 3 |
| Attention & Calculation | Serial 7s (subtract 7 from 100, five times) OR spell "WORLD" backwards | 5 |
| Recall | Recall the 3 objects named earlier | 3 |
| Language - Naming | Name a pencil and watch | 2 |
| Language - Repetition | Repeat: "No ifs, ands, or buts" | 1 |
| Language - 3-step command | Take paper, fold it, put it on floor | 3 |
| Reading | Read and obey: "Close your eyes" | 1 |
| Writing | Write a complete sentence | 1 |
| Visuospatial/Construction | Copy intersecting pentagons | 1 |
Interpretation of Scores
- 27-30: Normal cognition
- 21-26: Mild cognitive impairment
- 11-20: Moderate impairment
- 0-10: Severe impairment
Important Limitations (from Kaplan & Sadock's Synopsis of Psychiatry)
- Does NOT assess executive functions (frontal lobe) - a major gap
- Underestimates deficits in highly educated individuals with early Alzheimer disease
- Overestimates deficits in individuals with little education
- Cutoff scores must be adjusted for age and education
- Cannot differentiate the specific etiology of cognitive impairment - not a substitute for neuropsychological testing
Practical Tips for MMSE Administration
- Ensure the patient can hear you and understands the language
- No time pressure, but note if responses are slow
- Do not prompt or help with answers
- Score strictly - partial credit is not given for most items
- Document the total score AND note which domains were impaired
2. Motor System Examination
A complete motor examination involves these sequential steps:
Step 1 - Inspection
- Look for muscle wasting/atrophy (UMN vs LMN distinction)
- Look for fasciculations (fine muscle twitching - LMN sign)
- Note posture and involuntary movements (tremor, chorea, dystonia)
Step 2 - Tone Assessment
Ask the patient to relax. Passively move each joint:
- Normal tone: smooth resistance throughout range
- Hypotonia (flaccidity): decreased resistance - LMN lesion, cerebellar disease
- Hypertonia - Spasticity: velocity-dependent resistance, "clasp-knife" quality - UMN (corticospinal) lesion
- Hypertonia - Rigidity: uniform resistance throughout range ("lead-pipe" or "cogwheel" in Parkinson's) - basal ganglia lesion
Step 3 - Power/Strength Testing (MRC Scale)
| Grade | Description |
|---|---|
| 0 | No movement at all |
| 1 | Flicker/trace of contraction, no movement |
| 2 | Active movement with gravity eliminated |
| 3 | Active movement against gravity, not against resistance |
| 4 | Active movement against gravity and some resistance |
| 5 | Normal power against full resistance |
Test in a root-by-root, muscle-by-muscle pattern:
- Upper limb: shoulder abduction (C5), elbow flexion (C5/C6), wrist extension (C6/C7), finger extension (C7), finger abduction (T1)
- Lower limb: hip flexion (L1/L2), knee extension (L3/L4), ankle dorsiflexion (L4/L5), big toe extension (L5), ankle plantarflexion (S1/S2)
Step 4 - Coordination
- Finger-nose test: finger to own nose, to examiner's finger - tests cerebellar function
- Heel-shin test: heel along opposite shin
- Rapid alternating movements (dysdiadochokinesia): pat hand rapidly
- Romberg's test: stand feet together, eyes open then closed (positive = sways/falls with eyes closed = dorsal column/proprioceptive loss)
Step 5 - Gait
- Observe: stride length, arm swing, base width, turning
- Hemiplegic gait: circumduction of leg (UMN lesion)
- Cerebellar/ataxic gait: wide-based, staggering
- Parkinsonian gait: shuffling, festinating, reduced arm swing
- Steppage gait: foot drop, high stepping (LMN/peroneal nerve)
- Scissor gait: legs cross each other (bilateral spastic paresis)
3. Sensory System Examination
Systematic testing of all sensory modalities:
Primary Sensory Modalities
| Modality | Tool Used | Pathway Tested |
|---|---|---|
| Pain (Pinprick) | Disposable pin/Neurotip | Spinothalamic tract (contralateral) |
| Temperature | Warm & cold tuning fork/tubes | Spinothalamic tract (contralateral) |
| Light Touch | Cotton wisp | Both spinothalamic & dorsal column |
| Vibration | 128 Hz tuning fork (on bony prominences) | Dorsal columns (ipsilateral) |
| Joint Position Sense (Proprioception) | Move distal phalanx up/down | Dorsal columns (ipsilateral) |
Cortical/Higher Sensory Modalities (if primary intact)
- Two-point discrimination: Distinguish two simultaneous points (tests parietal cortex)
- Stereognosis: Identify object by touch with eyes closed (coin, key)
- Graphesthesia: Identify number/letter written on palm
- Point localization: Identify where you were touched
Practical Method
- Always explain the test to the patient first with eyes open, then test with eyes closed
- Work from areas of reduced sensation outward to normal
- Compare left vs. right, proximal vs. distal, upper vs. lower limbs
- Map the deficit - is it dermatomal (nerve root), peripheral nerve territory, or hemisensory (central)?
Patterns of Sensory Loss
- Glove and stocking: Peripheral polyneuropathy (e.g., diabetic neuropathy)
- Dermatomal: Nerve root compression
- Hemisensory loss: Contralateral thalamus or cortex lesion
- Dissociated (pain/temp lost, vibration intact): Syringomyelia, Brown-Sequard syndrome
- Vibration/proprioception lost, pain/temp intact: Dorsal column lesion (subacute combined degeneration, tabes dorsalis)
4. Reflexes - Names and Reflex Arc Levels
Deep Tendon Reflexes (DTRs) - Complete List
| Reflex | Stimulus | Response | Spinal Level |
|---|---|---|---|
| Biceps | Tap biceps tendon at elbow crease | Elbow flexion | C5, C6 |
| Brachioradialis (Supinator) | Tap radius 5 cm above wrist | Elbow flexion + supination | C5, C6 |
| Triceps | Tap triceps tendon above olecranon | Elbow extension | C7 |
| Finger Flexors (Trömner) | Flick middle finger | Finger flexion | C8 |
| Patellar (Knee Jerk) | Tap patellar tendon | Knee extension | L2, L3, L4 |
| Achilles (Ankle Jerk) | Tap Achilles tendon | Plantarflexion | S1, S2 |
Reflex Grading Scale
- 0: Absent (abnormal)
- 1+: Hypoactive / diminished
- 2+: Normal (brisk)
- 3+: Hyperactive without clonus
- 4+: Hyperactive with transient clonus
- 5+: Hyperactive with sustained clonus
Biceps Reflex Arc - Closed Loop (C5, C6)
- Tap biceps tendon → stretches biceps brachii
- Muscle spindle (Ia fiber) activated → afferent signal up C5/C6 dorsal root
- Synapse in spinal cord at C5-C6 level
- Efferent via C5/C6 ventral root → musculocutaneous nerve → biceps contracts
The arc is "closed" at C5-C6 in the cervical spinal cord.
Patellar Reflex Arc - Closed Loop (L2-L4)
- Tap patellar tendon → stretches quadriceps femoris
- Muscle spindle (Ia fiber) activated → afferent up L2-L4 dorsal root
- Monosynaptic synapse in spinal cord at L2-L4 level
- Efferent via L2-L4 ventral root → femoral nerve → quadriceps contracts (knee extends)
- Simultaneously, inhibitory interneurons relax the antagonist (hamstrings)
The arc is "closed" at L2-L4 (mainly L4) in the lumbar spinal cord.
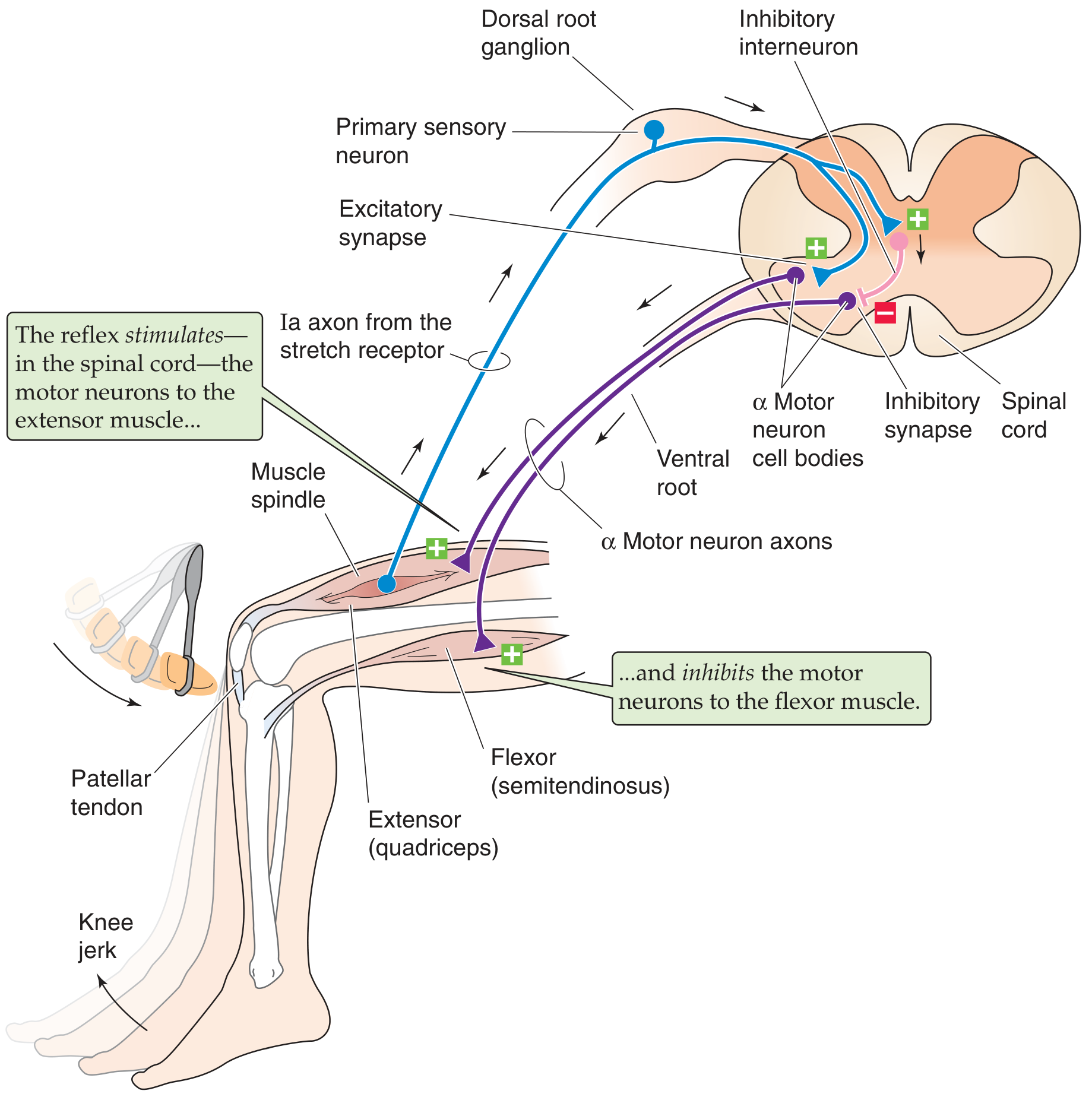
Diagram: Tapping the patellar tendon activates Ia axons from the muscle spindle. These make monosynaptic connections with alpha motor neurons (quadriceps), causing knee extension. Simultaneously, inhibitory interneurons relax the antagonist flexor (semitendinosus).
Superficial Reflexes
- Abdominal reflex: Stroke abdomen toward umbilicus - T8-T12
- Cremasteric reflex: Stroke inner thigh - L1, L2
- Plantar reflex (Babinski): Stroke lateral sole of foot
- Normal: plantarflexion (toes curl down)
- Abnormal (Babinski sign): dorsiflexion of big toe + fanning of other toes = UMN lesion
5. Multiple Sclerosis (MS) - Symptoms
MS is an autoimmune demyelinating disease of the central nervous system (brain, optic nerves, spinal cord). It is characterized by lesions disseminated in time and space.
(Source: Bradley and Daroff's Neurology in Clinical Practice)
Cardinal Features by System
Optic Nerve (Optic Neuritis - most common first presentation)
- Acute/subacute unilateral visual loss with pain on eye movement
- Decreased color vision
- Relative afferent pupillary defect (Marcus Gunn pupil)
- Central scotoma on visual field testing
- 90% recover vision over 2-6 months
Brainstem / Cranial Nerves
- Internuclear ophthalmoplegia (INO) - hallmark of MS in a young adult
- Impaired adduction of one eye with nystagmus in the abducting eye
- Caused by lesion in medial longitudinal fasciculus (MLF)
- Nystagmus (acquired pendular nystagmus is characteristic)
- Diplopia (double vision)
- Dysarthria (slurred speech)
- Vertigo (in 30-50% of patients)
- Facial numbness or trigeminal neuralgia in young adults
- Facial myokymia (undulating facial twitching)
Spinal Cord Symptoms
- Lhermitte's sign: Electric shock sensation down spine/limbs on neck flexion - pathognomonic of posterior column involvement
- Motor: spastic weakness of limbs (UMN pattern - hyperreflexia, spasticity, Babinski sign)
- Sensory: numbness, tingling, pins and needles, "MS hug" (band-like chest tightness)
- Impaired vibration and joint position sense (posterior column)
- Bladder dysfunction: urgency, frequency, retention, incontinence (neurogenic bladder)
- Bowel dysfunction: constipation, urgency
- Sexual dysfunction
Cerebellar Symptoms (Charcot's Triad)
- Intention tremor
- Nystagmus
- Scanning/staccato dysarthria
- Ataxic gait
- Dysmetria (past-pointing)
- Dysdiadochokinesia (inability to perform rapid alternating movements)
Cognitive & Psychiatric
- Cognitive slowing, memory problems
- Depression (very common)
- Euphoria (less common)
- Fatigue (most disabling complaint in >90% of patients)
Heat Sensitivity (Uhthoff's Phenomenon)
- Temporary worsening of symptoms with heat (hot shower, exercise, fever)
- Classic and characteristic of MS
6. Guillain-Barré Syndrome (GBS) - Symptoms
GBS is an acute immune-mediated inflammatory polyneuropathy affecting peripheral nerves and spinal roots. It is the leading cause of acute flaccid paralysis in the developed world.
(Source: Bradley and Daroff's Neurology in Clinical Practice)
Classic Presentation
- Onset: Often 2-4 weeks after respiratory or GI infection (esp. Campylobacter jejuni, CMV, EBV)
- Weakness: Begins in legs, ascends proximally ("ascending paralysis")
- Symmetric weakness of lower limbs first, then arms
- Can progress to quadriplegia
- In severe cases: respiratory muscle failure (requires ventilation in 9-30% of cases)
- Areflexia/Hyporeflexia: Invariable feature - absent deep tendon reflexes
- Sensory symptoms: Paresthesias (tingling, pins and needles) worse in hands and feet, but sensory loss is often mild compared to motor loss
- Pain: Moderate-severe pain in extremities, back, interscapular area in ~70% during acute phase
Autonomic Dysfunction (65% of hospitalized patients)
- Orthostatic hypotension
- Hypertension (episodic or sustained)
- Sinus tachycardia or bradycardia
- Cardiac arrhythmias
- Urinary retention
- Gastrointestinal atony (ileus)
- Sweating abnormalities
Cranial Nerve Involvement (45-75%)
- Bilateral facial palsy (most common cranial nerve involvement)
- Dysphagia, dysarthria (bulbar involvement)
- Ophthalmoplegia (in Miller-Fisher variant)
Diagnostic Criteria (Required)
- Progressive weakness of both legs and arms
- Areflexia or hyporeflexia
CSF Finding (Hallmark)
- Albuminocytological dissociation: Elevated protein (>45 mg/dL) with < 10 cells/μL (no pleocytosis)
GBS Subtypes
| Subtype | Key Features |
|---|---|
| AIDP (most common in West) | Demyelinating, good recovery |
| AMAN (Asia) | Pure motor axonal, summer epidemics |
| AMSAN | Motor + sensory axonal, severe, poor recovery |
| Miller-Fisher Syndrome | Triad: ophthalmoplegia + ataxia + areflexia |
7. Other Neurological Disorders - Symptoms
7a. Parkinson's Disease
Classic motor triad:
- Resting tremor - "pill-rolling" 4-6 Hz, disappears with movement
- Rigidity - cogwheel or lead-pipe resistance to passive movement
- Bradykinesia - slowness of voluntary movement (most disabling)
Additional features:
- Postural instability (later feature) - retropulsion, festinating gait
- Hypomimia (mask-like face, reduced blinking)
- Micrographia (progressively smaller handwriting)
- Hypophonia (soft, monotone speech)
- Shuffling gait with reduced arm swing
- Non-motor: depression, constipation, REM sleep disorder, anosmia (often precedes motor symptoms by years), dementia (Parkinson's dementia, 30-40% of patients)
7b. Myasthenia Gravis
Autoimmune disease: antibodies against acetylcholine receptors at the neuromuscular junction.
Key features:
- Fatigable weakness - gets worse with activity, improves with rest
- Ptosis and diplopia - most common first presentation (ocular myasthenia)
- Bulbar weakness: dysarthria, dysphagia, nasal regurgitation
- Limb weakness (proximal > distal)
- Respiratory failure in myasthenic crisis
- Normal reflexes and sensation (pure motor, NMJ disease)
- Positive Tensilon (edrophonium) test
- Ice pack test: ptosis improves when ice applied to eye (cold improves NMJ function)
- Thymoma association (10-15%)
7c. Stroke (CVA)
Ischemic stroke (80%) vs. hemorrhagic stroke (20%)
Classical cortical symptoms by territory:
- MCA territory (most common): contralateral hemiplegia (face + arm > leg), hemisensory loss, homonymous hemianopia, aphasia (dominant hemisphere), neglect (non-dominant)
- ACA territory: contralateral leg weakness > arm, urinary incontinence, behavioral changes
- PCA territory: homonymous hemianopia, memory deficits, cortical blindness
- Lacunar infarcts: pure motor hemiplegia, pure sensory stroke, ataxic hemiparesis, dysarthria-clumsy hand syndrome
FAST signs for public awareness: Face drooping, Arm weakness, Speech difficulty, Time to call emergency services
7d. Meningitis
Inflammation of meninges (bacterial, viral, fungal, TB):
Classic triad:
- Fever
- Severe headache ("worst headache of life" if subarachnoid hemorrhage/meningeal irritation)
- Neck stiffness (nuchal rigidity)
Additional signs:
- Photophobia and phonophobia
- Kernig's sign: Flex hip 90°, then attempt to extend knee - pain/resistance = positive
- Brudzinski's sign: Passive neck flexion causes involuntary flexion of hips and knees
- Jolt accentuation of headache: Horizontal head rotation at 2-3 Hz worsens headache
- Non-blanching petechial/purpuric rash (meningococcal septicaemia - emergency)
- Altered consciousness (bacterial meningitis more severe)
- Seizures
Summary - UMN vs LMN Differentiation (Practical Examination Key)
| Feature | UMN Lesion (above cord) | LMN Lesion (cord/nerve) |
|---|---|---|
| Tone | Increased (spasticity) | Decreased (flaccidity) |
| Power | Reduced | Reduced |
| Reflexes | Increased (hyperreflexia) | Decreased/absent |
| Plantar | Extensor (Babinski +ve) | Flexor (normal) |
| Clonus | Present | Absent |
| Wasting | Late, mild | Early, severe |
| Fasciculations | Absent | Present |
Sources:
- Kaplan & Sadock's Synopsis of Psychiatry - MMSE and neuropsychological assessment
- Bradley and Daroff's Neurology in Clinical Practice - MS, GBS clinical features
- Ganong's Review of Medical Physiology, 26e - Reflex arcs and DTR grading
- Medical Physiology (Boron & Boulpaep) - Motor system, stretch reflex arc
Summarize with important tests
Neurological Examination - Quick Summary with Important Tests
1. MMSE (30 Points Total)
| Domain | Test | Score |
|---|---|---|
| Orientation | Date/day/month/year/season + Country/state/city/hospital/floor | 5+5 |
| Registration | Repeat 3 objects (apple, table, penny) | 3 |
| Attention | Serial 7s OR spell WORLD backwards | 5 |
| Recall | Remember the 3 objects | 3 |
| Language | Name pencil + watch / Repeat phrase / 3-step command / Read & obey / Write sentence | 2+1+3+1+1 |
| Visuospatial | Copy intersecting pentagons | 1 |
Score interpretation: 27-30 = Normal | 21-26 = Mild | 11-20 = Moderate | 0-10 = Severe
2. Motor System - Key Tests
| Test | What You Do | What It Tells You |
|---|---|---|
| Inspection | Look for wasting, fasciculations | LMN lesion |
| Tone | Passively move limb - feel resistance | Spasticity (UMN) vs Rigidity (Basal ganglia) vs Flaccidity (LMN) |
| Power (MRC 0-5) | Resist active movement at each joint | Weakness distribution |
| Finger-Nose Test | Touch nose then examiner's finger repeatedly | Cerebellar intention tremor |
| Heel-Shin Test | Heel slides down opposite shin | Cerebellar lower limb |
| Dysdiadochokinesia | Rapid alternating hand movements | Cerebellar dysfunction |
| Romberg's Test | Stand feet together - eyes open then closed | Positive = dorsal column/proprioception loss |
| Gait | Walk, turn, heel-toe walk | Hemiplegic / Ataxic / Parkinsonian / Steppage |
3. Sensory System - Key Tests
| Test | Tool | Pathway |
|---|---|---|
| Pinprick | Disposable pin | Spinothalamic (contralateral) |
| Temperature | Cold/warm tubing | Spinothalamic (contralateral) |
| Light Touch | Cotton wisp | Both pathways |
| Vibration | 128 Hz tuning fork on bony points | Dorsal column (ipsilateral) |
| Proprioception | Move distal joint up/down | Dorsal column (ipsilateral) |
| Stereognosis | Identify object by touch (eyes closed) | Parietal cortex |
| Graphesthesia | Number written on palm | Parietal cortex |
| Two-point discrimination | Two pins simultaneously | Parietal cortex |
4. Important Reflexes
| Reflex | How to Elicit | Response | Arc Closed At |
|---|---|---|---|
| Biceps | Tap biceps tendon at elbow | Elbow flexion | C5, C6 |
| Triceps | Tap above olecranon | Elbow extension | C7 |
| Brachioradialis | Tap radius above wrist | Elbow flexion + supination | C5, C6 |
| Patellar (Knee jerk) | Tap patellar tendon | Knee extension | L2, L3, L4 |
| Achilles (Ankle jerk) | Tap Achilles tendon | Plantarflexion | S1, S2 |
| Plantar (Babinski) | Stroke lateral sole | Normal = toes flex DOWN | Cortical UMN |
Babinski Sign = Big toe goes UP + other toes fan out = UMN lesion (ABNORMAL in adults)
DTR Grade: 0 = Absent | 1+ = Diminished | 2+ = Normal | 3+ = Hyperactive | 4+ = Clonus
5. Multiple Sclerosis - Key Signs & Tests
"Disseminated in time AND space" - hallmark concept
| System | Key Finding | Important Test |
|---|---|---|
| Optic nerve | Painful unilateral visual loss | Swinging flashlight test → Marcus Gunn pupil (RAPD) |
| Brainstem | Internuclear ophthalmoplegia (INO) | Horizontal gaze - impaired adduction + nystagmus in other eye |
| Spinal cord | Lhermitte's sign | Flex neck → electric shock down spine |
| Sensory | Numbness, tingling, "MS hug" | Sensory examination |
| Cerebellum | Ataxia, intention tremor | Finger-nose, gait, dysdiadochokinesia |
| Bladder | Urgency, retention | Post-void residual ultrasound |
| Heat | Uhthoff's phenomenon | Symptoms worsen with hot shower/exercise |
Investigations: MRI brain + spine (white matter plaques) | VEPs (delayed in optic neuritis) | CSF - oligoclonal bands
6. Guillain-Barré Syndrome - Key Signs & Tests
"Ascending flaccid paralysis with areflexia" - hallmark concept
| Feature | Finding | Test |
|---|---|---|
| Weakness | Starts in legs, ascends upward | MRC power grading - bilateral symmetrical |
| Reflexes | Absent (areflexia) - invariable | DTR examination |
| Sensory | Mild paresthesias distally | Sensory exam - glove/stocking pattern |
| Autonomic | BP swings, tachycardia, urinary retention | BP monitoring, ECG |
| Facial | Bilateral facial palsy (45-75%) | CN VII examination |
| Respiratory | Respiratory failure (9-30%) | Forced Vital Capacity (FVC) - bedside spirometry |
| CSF | High protein, <10 cells | Lumbar puncture → albuminocytological dissociation |
| Nerve conduction | Slowed velocity, conduction block | NCS/EMG |
7. Other Disorders - Key Tests Summary
Parkinson's Disease
| Sign | Test |
|---|---|
| Resting tremor | Observe at rest, disappears with movement |
| Rigidity | Passive movement - cogwheel feel at wrist |
| Bradykinesia | Finger tapping, hand opening/closing speed |
| Postural instability | Pull test (retropulsion) |
| Gait | Shuffling, festination, reduced arm swing |
Myasthenia Gravis
| Test | Positive Finding |
|---|---|
| Sustained upward gaze | Ptosis worsens after 30-60 seconds |
| Ice pack test | Ptosis improves with ice on eye |
| Counting aloud to 100 | Voice becomes nasal/weaker |
| Tensilon (edrophonium) test | Rapid improvement in ptosis |
| Anti-AChR antibodies | Positive in 85% |
Meningitis
| Sign | How to Test | Positive Finding |
|---|---|---|
| Nuchal rigidity | Passive neck flexion | Cannot touch chin to chest |
| Kernig's sign | Flex hip 90°, extend knee | Pain/resistance at <135° |
| Brudzinski's sign | Flex neck passively | Hips and knees reflexly flex |
| Jolt accentuation | Rotate head 2-3x/second | Headache worsens |
UMN vs LMN - The Most Important Distinction
| UMN (Brain/Cord) | LMN (Nerve/Root) | |
|---|---|---|
| Tone | ↑ Spasticity | ↓ Flaccidity |
| Reflexes | ↑ Hyperreflexia | ↓ / Absent |
| Babinski | + (extensor) | - (flexor) |
| Wasting | Mild, late | Severe, early |
| Fasciculations | Absent | Present |
| Example | Stroke, MS | GBS, polio, disc prolapse |
Memory aid for reflex levels: "C5-6 pick up sticks (biceps), C7 lay them straight (triceps), L3-4 kick the door (patellar), S1-2 stamp the floor (Achilles)"
This is a shared conversation. Sign in to Orris to start your own chat.