Retrosternal chest pain with nausea and vomiting, ECG changes, ST elevation in V1, V2, V3, V4, V5, V6.
Reading File
Finding Sources
Finding Sources
Searching PubMed
"STEMI" AND "anterior myocardial infarction" AND "management"
Finding Sources
Finding Sources
Searching PubMed
"anterior STEMI" AND "reperfusion"
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Now I have comprehensive information to provide a thorough clinical analysis. Here is the full response:
Anterior STEMI (ST-Elevation Myocardial Infarction)
ECG Interpretation
The ECG pattern shown - ST elevation across V1 through V6 - is the hallmark of a large anterior (anterolateral) STEMI.
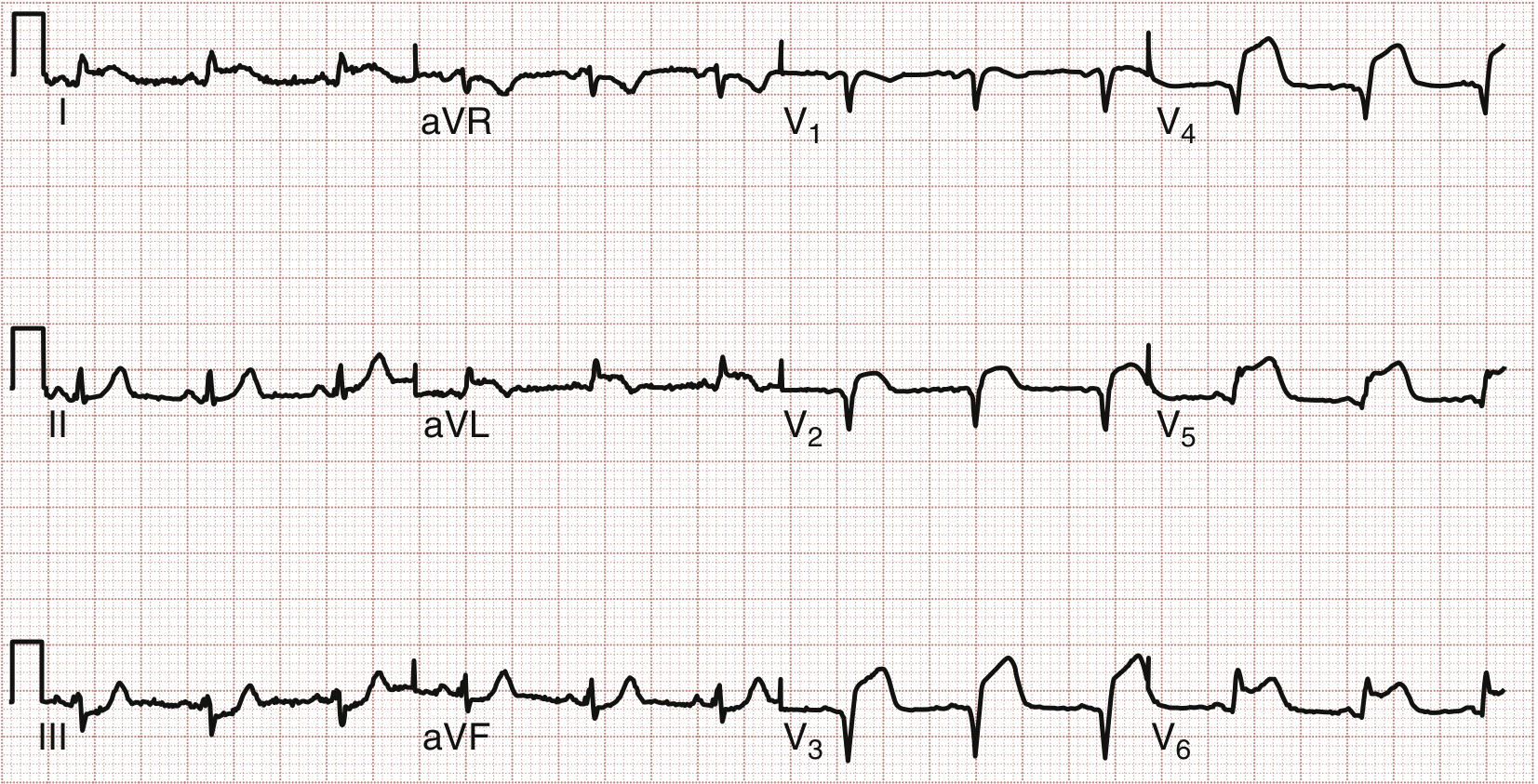
This ECG shows anterolateral ST segment elevation - the pattern matching the clinical scenario described.
Anatomic Localization (Table 4-14)
| ST Elevation Leads | Myocardial Territory | Culprit Artery |
|---|---|---|
| V1-V6 (as here) | Anterior + septal + lateral walls | Proximal LAD or Left Main |
| V1-V2 | Septum | Proximal LAD / septal branch |
| V2-V4 | Anterior wall | LAD |
| V5-V6 | Lateral wall | LCX |
| II, III, aVF | Inferior wall | RCA or LCX |
ST elevation spanning V1-V6 indicates occlusion of the proximal LAD or possibly the left main coronary artery - this is the highest-risk STEMI pattern, involving a large myocardial territory.
- Washington Manual of Medical Therapeutics, p. 147
ECG Diagnostic Thresholds for STEMI
- Men >40 years: ST elevation ≥2 mm at J-point in V2-V3, >1 mm in all other leads
- Men <40 years: >2.5 mm in V2-V3
- Women: >1.5 mm in V1-V3, >1 mm in other leads
Two or more anatomically contiguous leads must meet threshold for diagnosis. - Washington Manual of Medical Therapeutics, p. 147
Diagnosis
STEMI - Large Anterior/Anterolateral MI
Triad present here:
- Symptoms: Retrosternal chest pain + nausea/vomiting (vagal response to ischemia, common in anterior MI)
- ECG: ST elevation in V1-V6 (2+ contiguous leads)
- Mechanism: Thrombotic occlusion of proximal LAD causing transmural ischemia of the anterior + septal + lateral walls
Differential Diagnosis of ST Elevation
Before committing to STEMI, consider (especially important if presentation is atypical):
| Cardiac | Other |
|---|---|
| Prior MI with aneurysm | Pulmonary embolism |
| Aortic dissection with coronary involvement | Hyperkalemia |
| Pericarditis / Myocarditis | |
| LV hypertrophy / strain | |
| Brugada syndrome | |
| Coronary vasospasm (Prinzmetal, cocaine) | |
| Early repolarization (normal variant) |
Get prior ECGs to compare. Aortic dissection must be excluded before fibrinolysis. - Washington Manual of Medical Therapeutics, p. 148
Immediate Management - Time is Myocardium
Step 1: Activate the STEMI Protocol NOW
- ECG must be obtained within 10 minutes of presentation
- Activate the catheterization lab immediately
- Target: door-to-balloon (D2B) time <90 minutes
Step 2: Immediate Medications (Before/During Transport to Cath Lab)
| Drug | Dose | Notes |
|---|---|---|
| Aspirin | 325 mg PO (loading) | Give immediately, continue 81 mg/d indefinitely |
| P2Y12 inhibitor | Ticagrelor 180 mg OR Prasugrel 60 mg OR Clopidogrel 600 mg | Give if PCI planned; use only clopidogrel if fibrinolysis planned |
| Anticoagulation | UFH (weight-based) or Bivalirudin | UFH is preferred if PCI or fibrinolysis; start immediately |
| Nitroglycerin | 0.4 mg SL q5min x3, then IV | Avoid if hypotension, RV infarct suspected, or PDE5i use |
| Oxygen | Supplement if SpO2 <90% | Do not give routinely if SpO2 normal |
| Morphine / Fentanyl | IV for refractory pain | Note: morphine may mask ongoing symptoms; use cautiously |
- Rosen's Emergency Medicine, p. 1033
- Washington Manual of Medical Therapeutics, p. 155
Step 3: Reperfusion Strategy
Primary PCI available within 90 min of first medical contact?
│
YES ──► PRIMARY PCI (preferred)
│
NO ──► Transfer for PCI still possible within 120 min?
│
YES ──► Transfer for primary PCI
│
NO ──► FIBRINOLYSIS (if within 12h of onset, no contraindications)
─ Give within 30 min of first contact ("door-to-needle")
─ Transfer to PCI center afterward regardless
Primary PCI is superior to fibrinolysis in all situations where it is available in time:
-
Greater TIMI 3 flow restoration
-
Less reinfarction
-
No intracranial hemorrhage risk
-
Better survival
-
Washington Manual of Medical Therapeutics, p. 156-157
When PCI is ALWAYS Preferred (even if delayed)
- Cardiogenic shock / severe HF (Killip class III/IV)
- Contraindication to fibrinolysis
- Prior CABG or recent PCI
- Symptom onset >12 hours ago
Contraindications to Fibrinolysis
Absolute:
- Prior intracranial hemorrhage (any time)
- Ischemic stroke within 3 months
- Known intracranial neoplasm or AVM
- Closed head injury within 3 months
- Suspected aortic dissection
- Active bleeding / bleeding diathesis
- SBP >180 or DBP >110 mm Hg (severe uncontrolled HTN)
Relative:
- Prior ischemic stroke >3 months
- Major surgery within 3 weeks
- Active peptic ulcer
- Recent internal bleeding (2-4 weeks)
- Pregnancy
Complications to Monitor (Anterior MI Specific)
| Complication | Details |
|---|---|
| Cardiogenic shock | Proximal LAD occlusion = large infarct, high risk |
| AV block / conduction disturbance | Anterior MI AV block is unstable (wide QRS escape, 80% mortality) - often needs pacemaker (unlike inferior MI, which is transient) |
| LV dysfunction / heart failure | Get baseline echo; assess EF |
| LV thrombus | Risk with apical hypokinesis; monitor but routine anticoagulation not indicated without confirmed thrombus |
| VSD / papillary muscle rupture | Mechanical complications - emergency surgery if they occur |
| Ventricular arrhythmias | Continuous telemetry in CCU |
- Washington Manual of Medical Therapeutics, p. 160
Post-STEMI Medical Therapy (Long-Term)
| Drug | Details |
|---|---|
| ASA | 81 mg/d indefinitely |
| P2Y12 inhibitor | Minimum 12 months (clopidogrel/ticagrelor/prasugrel) |
| Beta-blocker | Start within 24h, continue indefinitely; mortality benefit |
| ACE inhibitor / ARB | Start within 24h; especially important in anterior MI with EF <40% |
| High-intensity statin | Start early; target LDL <70 mg/dL or ≥50% reduction |
| Aldosterone antagonist | If EF <40% or diabetes (eplerenone/spironolactone) |
- Washington Manual of Medical Therapeutics, p. 160-161
Key Time Targets (ACC/AHA)
| Target | Goal |
|---|---|
| First ECG | ≤10 minutes from presentation |
| Door-to-balloon (primary PCI) | ≤90 minutes |
| Door-to-needle (fibrinolysis) | ≤30 minutes |
| Transfer + PCI (if transferred) | First medical contact to balloon ≤120 minutes |
Summary
This patient has a large anterolateral STEMI from proximal LAD or left main occlusion. This is a time-critical emergency. The single most important intervention is achieving coronary reperfusion as rapidly as possible via primary PCI. All adjunctive therapies (aspirin, P2Y12 inhibitor, anticoagulation) should be given promptly but must not delay transport to the catheterization laboratory.
Admit to CCU for continuous monitoring post-intervention. Given the extent of territory involved (V1-V6), monitor closely for LV dysfunction, conduction abnormalities, and mechanical complications.
This is a shared conversation. Sign in to Orris to start your own chat.