Antiarrhythmic drugs
Reading File
Finding Sources
Searching PubMed
"antiarrhythmic drugs"[MeSH Terms] AND "classification"
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Reading File
Reading File
I now have comprehensive, well-sourced material to write a thorough answer. Let me compose it.
Antiarrhythmic Drugs
Cardiac Action Potential - Basis of Drug Action
Before classifying these drugs, it helps to know what they target:
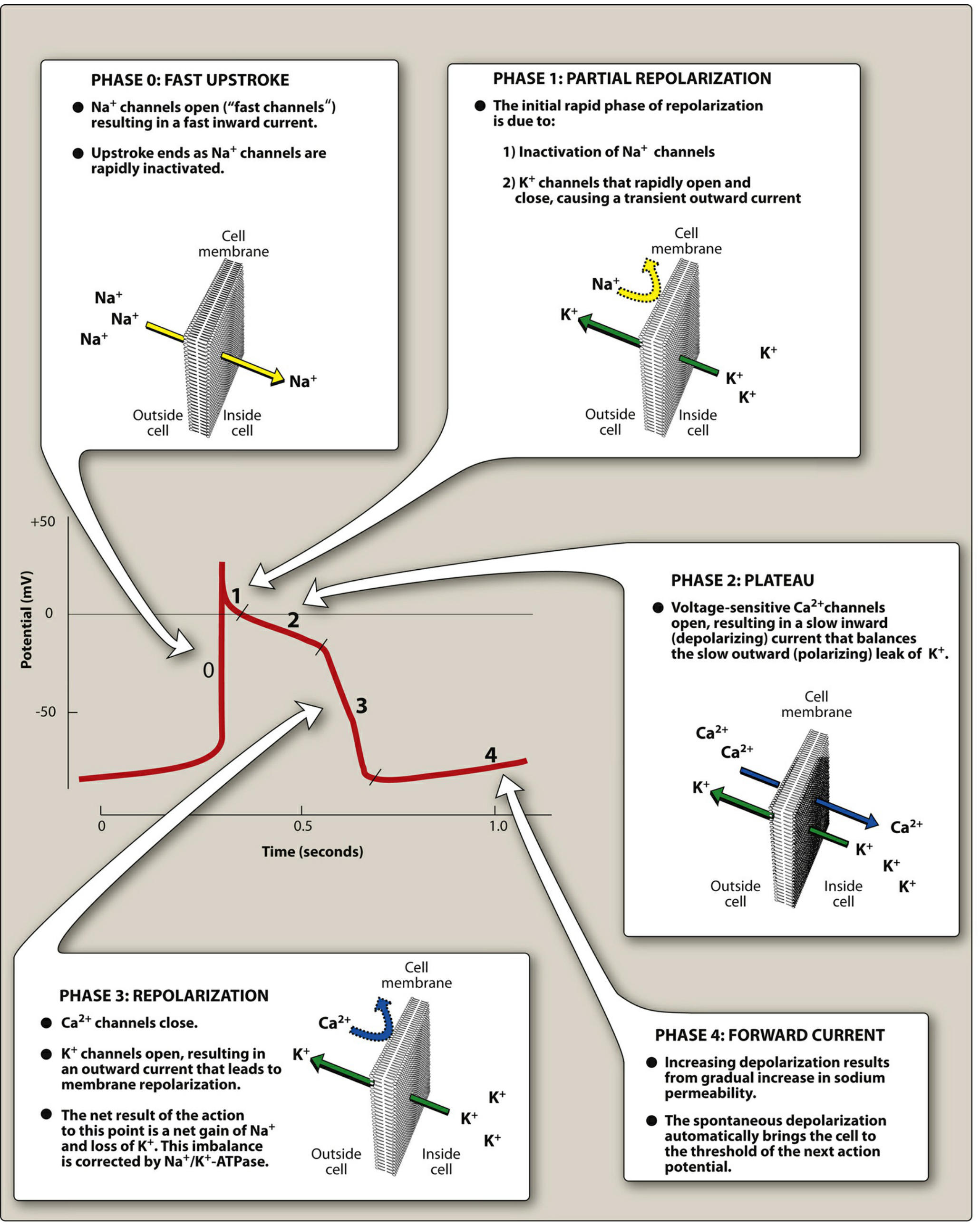
- Phase 0 - Fast upstroke: Na+ channels open (fast inward current)
- Phase 1 - Partial repolarization: Na+ channels inactivate; transient K+ outward current
- Phase 2 - Plateau: Voltage-sensitive Ca2+ channels open, balancing slow K+ leak
- Phase 3 - Repolarization: Ca2+ channels close; K+ channels open (outward current)
- Phase 4 - Spontaneous depolarization in pacemaker cells: gradual increase in Na+ permeability drives cell toward threshold
Lippincott Illustrated Reviews: Pharmacology
Mechanisms of Arrhythmias
Two principal mechanisms:
- Abnormal automaticity - Ectopic pacemaker sites fire faster than the SA node. Most antiarrhythmics suppress this by blocking Na+ or Ca2+ channels, reducing the slope of Phase 4 depolarization and/or raising the discharge threshold.
- Reentry - The most common cause. A unidirectional block (from ischemia, scarring, or prolonged refractory period) allows an impulse to travel in a circuit, re-exciting myocardium. Drugs can terminate reentry by converting the unidirectional block into a bidirectional block or by prolonging the refractory period of the circuit.
Vaughan Williams Classification
The standard classification (Vaughan Williams, 1970) groups drugs by their predominant action on the cardiac action potential. Most antiarrhythmic drugs affect more than one ion current and many exert ancillary effects on contractility or the autonomic nervous system, so this classification has real limitations in clinical practice.
Goodman & Gilman's Pharmacological Basis of Therapeutics
CLASS I - Sodium Channel Blockers
Block the fast inward Na+ current (I_Na), reducing conduction velocity in fast-response tissue and increasing QRS duration. Effect is rate-dependent (use-dependent block): more block at faster heart rates.
Sub-classified by the kinetics of Na+ channel binding/unbinding (τ_recovery):
Class IA - Intermediate kinetics, also block K+ channels
These drugs slow Phase 0 AND prolong the action potential duration (APD) by also blocking K+ channels (I_Kr), extending the refractory period. They prolong the QT interval.
| Drug | Key Features | Clinical Use | Notable Toxicities |
|---|---|---|---|
| Quinidine | Oldest; also antimuscarinic | AF, VT | Cinchonism (tinnitus, headache, visual disturbances), hemolytic anemia, esophagitis, torsades de pointes |
| Procainamide | IV/IM available | VT, pre-excited AF | Drug-induced lupus (SLE-like syndrome), hypotension, torsades via NAPA metabolite in renal failure |
| Disopyramide | Strong antimuscarinic effects | AF, VT | May precipitate heart failure; anticholinergic side effects (urinary retention, dry mouth) |
Class IB - Fast kinetics, shorten APD
Block Na+ channels in inactivated state with rapid recovery. They do not prolong (and may actually shorten) the APD. Preferentially affect ischemic or depolarized tissue.
| Drug | Route | Key Features | Toxicities |
|---|---|---|---|
| Lidocaine | IV only (high first-pass) | Drug of choice for acute ventricular arrhythmias; CNS toxicity (tremor, seizures, confusion) | Neurological symptoms (dose-related) |
| Mexiletine | Oral analog of lidocaine | Chronic VT, used in channelopathies (LQT3, NaV1.5 mutations) | Nausea/vomiting, dyspepsia, neurological |
Class IC - Slow kinetics, minimal effect on APD
Markedly slow Phase 0 and markedly widen QRS; slow dissociation from Na+ channel means the channel does not fully recover between beats - very rate-dependent effect.
| Drug | Key Features | Clinical Use | Toxicities |
|---|---|---|---|
| Flecainide | Most potent Na+ blocker in class | Supraventricular arrhythmias (AF/flutter/SVT) in structurally normal hearts | Strongly proarrhythmic in ischemic heart disease (CAST trial) |
| Propafenone | Also has weak beta-blocking activity | Paroxysmal AF, SVT | Bronchospasm, liver failure, agranulocytosis |
CAST Trial Warning: Class IC drugs (encainide, flecainide) significantly increased mortality in post-MI patients despite suppressing PVCs. These drugs are contraindicated in structural or ischemic heart disease.
CLASS II - Beta-Adrenergic Blockers
Antagonize catecholamine effects on the heart. Primarily act on SA and AV nodes - reduce automaticity (slow Phase 4) and slow AV nodal conduction. Also have direct membrane Na+ channel blocking effects.
Drugs: Metoprolol, Atenolol, Esmolol (IV, ultra-short-acting), Propranolol, Carvedilol
Clinical uses:
- Rate control in AF and atrial flutter
- AV nodal reentry tachycardia (AVNRT)
- Post-MI arrhythmia prevention
- Hypertrophic obstructive cardiomyopathy
- CPVT (catecholaminergic polymorphic VT) - first-line
Toxicities: Bradycardia, heart block, hypotension, worsening HF, bronchospasm, fatigue, exercise intolerance, sexual dysfunction, hyperlipidemia.
CLASS III - Potassium Channel Blockers
Block outward K+ currents (mainly I_Kr), prolonging Phase 3 repolarization and extending the effective refractory period and QT interval. Increased risk of torsades de pointes if QT prolongation is excessive.
| Drug | Additional Actions | Clinical Use | Important Toxicities |
|---|---|---|---|
| Amiodarone | Blocks Na+, Ca2+, K+ channels AND has alpha/beta-blocking properties; Class I+II+III+IV | AF (rate + rhythm control), VT, VF prevention; "the dirty drug" | Pulmonary toxicity (pneumonitis/fibrosis), hepatotoxicity, hypo/hyperthyroidism, corneal deposits, blue-gray skin discoloration, peripheral neuropathy, bradycardia |
| Dronedarone | Amiodarone analog without iodine | AF (rhythm control) | Increased mortality in severe HF; less thyroid/lung toxicity than amiodarone |
| Sotalol | Also non-selective beta-blocker | VT, AF | Torsades de pointes (dose-dependent QT prolongation); bradycardia |
| Dofetilide | Pure I_Kr blocker | AF cardioversion and maintenance | Torsades de pointes (requires in-hospital initiation) |
| Ibutilide | IV only; also activates inward Na+ current | AF/flutter cardioversion | Torsades de pointes |
Amiodarone is the most widely used antiarrhythmic overall because of its broad effectiveness, but its adverse effect profile is extensive and long-term use requires monitoring of thyroid, liver, lungs, and eyes.
CLASS IV - Calcium Channel Blockers (Non-dihydropyridines)
Block L-type Ca2+ channels in the SA and AV nodes (which are Ca2+-dependent, "slow-response" tissue). They slow AV conduction and reduce automaticity.
| Drug | Route | Key Uses | Toxicities |
|---|---|---|---|
| Verapamil | PO/IV | AVNRT, rate control in AF/flutter | Bradycardia, heart block, negative inotropy (avoid in HFrEF), constipation, gingival hyperplasia |
| Diltiazem | PO/IV | Rate control in AF/flutter, AVNRT | Bradycardia, heart block, peripheral edema, hypotension |
Avoid verapamil/diltiazem in WPW (Wolff-Parkinson-White) with AF - they may accelerate conduction down the accessory pathway, triggering VF.
Other Antiarrhythmic Agents
Adenosine
- Naturally occurring nucleoside; at high doses decreases conduction velocity, prolongs refractory period, and decreases automaticity in the AV node
- Drug of choice for terminating acute SVT (AVNRT, AVRT)
- Extremely short duration (~10-15 seconds) due to rapid uptake by erythrocytes and endothelial cells
- Given as rapid IV bolus (6 mg, then 12 mg)
- Side effects: flushing, chest pain/pressure, transient dyspnea, hypotension (all brief)
- Contraindicated in asthma; can be used safely in WPW
Digoxin
- Inhibits Na+/K+-ATPase; indirect vagotonic effect via increased vagal tone
- Shortens atrial refractory period; prolongs AV nodal conduction and refractoriness
- Rate control in AF/flutter (but sympathetic stimulation easily overcomes it)
- Therapeutic trough: 1.0-2.0 ng/mL for AF; 0.5-0.9 ng/mL for HFrEF
- Toxicity at >2.0 ng/mL: bradycardia, AV block, ectopic ventricular beats, VT/VF; GI symptoms; yellow/blurred vision; confusion
- Risk increased by hypokalemia, hypomagnesemia, renal impairment
Magnesium Sulfate (IV)
- Slows SA node impulse formation; prolongs conduction along myocardial tissue
- Drug of choice for torsades de pointes (regardless of magnesium level)
- Also used for digoxin-induced arrhythmias
Ranolazine
- Primarily antianginal; antiarrhythmic properties similar to amiodarone
- Main effect: shortens repolarization, decreases APD (via late Na+ current block)
- Can suppress arrhythmias associated with the long QT syndrome
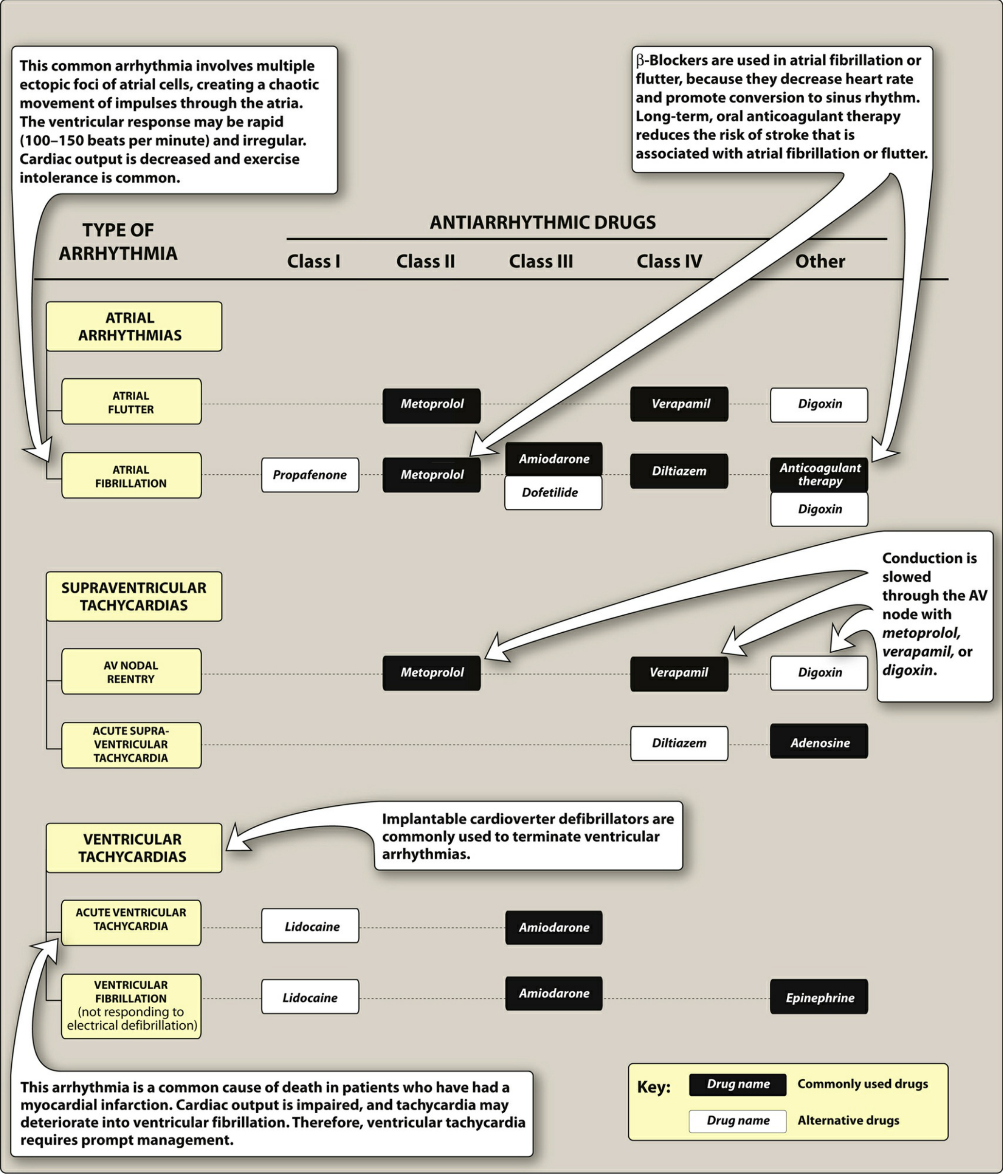
Therapeutic Indications by Arrhythmia
Lippincott Illustrated Reviews: Pharmacology
| Arrhythmia | First-Line / Commonly Used |
|---|---|
| Acute SVT (AVNRT) | Adenosine IV; verapamil/diltiazem; metoprolol |
| Atrial flutter | Rate control: metoprolol, verapamil; Rhythm: amiodarone, dofetilide |
| Atrial fibrillation (rate control) | Metoprolol, diltiazem, verapamil, digoxin |
| Atrial fibrillation (rhythm control) | Amiodarone, flecainide (no structural disease), propafenone, dofetilide, sotalol |
| Acute VT (hemodynamically stable) | Amiodarone IV, lidocaine IV |
| VT post-MI prevention | Amiodarone, beta-blockers, ICD |
| VF (refractory to defibrillation) | Amiodarone IV, lidocaine, epinephrine |
| Torsades de pointes | IV Magnesium sulfate; correct electrolytes; temporary pacing |
| WPW with AF | Procainamide IV; avoid AV nodal blockers |
| CPVT | Beta-blockers (nadolol, propranolol); flecainide |
Key Points on Proarrhythmia
All antiarrhythmic drugs can cause the very arrhythmias they are meant to treat - this is the fundamental paradox of antiarrhythmic therapy:
- QT prolongation (class IA, III) raises risk of torsades de pointes - a polymorphic VT that can degenerate to VF
- Class IC drugs are strongly proarrhythmic in ischemic/structural heart disease (CAST trial)
- Amiodarone is the least proarrhythmic of the QT-prolonging drugs, despite its other toxicities
- Risk is amplified by: hypokalemia, hypomagnesemia, bradycardia, female sex, drug-drug interactions (inhibited metabolism)
Sources:
- Goodman & Gilman's Pharmacological Basis of Therapeutics, Chapter 34
- Katzung's Basic and Clinical Pharmacology, 16th Edition
- Lippincott Illustrated Reviews: Pharmacology, Chapter 11
This is a shared conversation. Sign in to Orris to start your own chat.