Screening and diagnosis of OSA from AASM guidelines
Reading File
Finding Sources
Finding Sources
Searching PubMed
"obstructive sleep apnea" AND "AASM" AND diagnosis
Searching the Web
AASM 2023 2024 OSA obstructive sleep apnea screening diagnosis guidelines criteria
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC5337595
Finding Sources
Reading Article
PMID: 40838698
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a thorough, well-organized answer. Here is the complete response:
Screening and Diagnosis of OSA - AASM Guidelines
1. Overview
The core AASM clinical practice guideline on this topic is the 2017 Clinical Practice Guideline for Diagnostic Testing for Adult Obstructive Sleep Apnea (Kapur et al., JCSM 2017), which updated previous 2005/2007 parameters and was endorsed by the World Sleep Society in 2021. The AASM Scoring Manual (Version 3, 2023) provides the technical scoring rules underlying all diagnostic criteria. A focused update to the diagnostic testing guideline is currently in development (Task Force Chair: Indu Ayappa, PhD).
2. Diagnostic Criteria for OSA
The AASM defines OSA as meeting one of the following two criteria on polysomnography (PSG) or home sleep apnea testing (HSAT):
| Criterion | Requirement |
|---|---|
| A (Symptomatic) | AHI ≥ 5 events/hour PLUS symptoms: snoring, witnessed apneas, gasping/choking, or excessive daytime sleepiness (EDS) not explained by other causes |
| B (Asymptomatic) | AHI ≥ 15 events/hour (regardless of symptoms) |
Event definitions (AASM Scoring Manual):
- Apnea: Complete cessation of airflow for ≥ 10 seconds despite continued respiratory effort (obstructive) or without effort (central)
- Hypopnea (AASM recommended): ≥ 30% reduction in airflow for ≥ 10 seconds, accompanied by either ≥ 3% oxygen desaturation (SpO2) OR a cortical arousal
- Hypopnea (CMS criteria): ≥ 30% reduction in airflow, accompanied by ≥ 4% oxygen desaturation - this is slightly more restrictive than AASM
- RERA (Respiratory Effort-Related Arousal): Flow limitation associated with cortical arousal; included in the Respiratory Disturbance Index (RDI) but not the AHI
OSA vs. CSA distinction: OSA is characterized by obstructive events (>50% of events are obstructive, i.e., airflow absent/reduced with continued respiratory effort). CSA has >50% central apneas/hypopneas with central AHI >5. - Braunwald's Heart Disease, Table 89.1
3. Severity Classification
| Severity | AHI (events/hour) |
|---|---|
| Mild | 5 - 14 |
| Moderate | 15 - 30 |
| Severe | > 30 |
Additional severity markers include degree of nocturnal hypoxemia (oxygen nadir, % time SpO2 <90%), sleep fragmentation, and symptom burden. Treatment is generally recommended for moderate-to-severe disease or mild disease with symptoms. - Miller's Anesthesia, 10e, p. 8338
4. Screening: Who to Test
AASM "Increased Risk" Criteria for Diagnostic Testing
The AASM defines increased risk of moderate-to-severe OSA as:
Excessive daytime sleepiness PLUS at least 2 of the following 3:
- Habitual loud snoring
- Witnessed apnea, gasping, or choking
- Diagnosed hypertension
Patients meeting these criteria should proceed to formal sleep testing.
Clinical Screening Tools
Questionnaires and prediction algorithms cannot be used to diagnose OSA on their own - they are adjuncts to clinical assessment only (AASM Strong Recommendation).
STOP-BANG Questionnaire (most widely validated perioperative screening tool):
| Letter | Question |
|---|---|
| S - Snoring | Do you snore loudly (audible through closed doors)? |
| T - Tired | Do you often feel tired, fatigued, or sleepy during the day? |
| O - Observed | Has anyone observed you stop breathing during sleep? |
| P - Pressure | Do you have or are you being treated for high blood pressure? |
| B - BMI | BMI > 35 kg/m²? |
| A - Age | Age > 50 years? |
| N - Neck | Neck circumference > 40 cm? |
| G - Gender | Male? |
- Score ≥ 3: High risk (screened positive - proceed to testing)
- Score 5-8: Suggests moderate-to-severe OSA specifically
- Score 0-2: Low risk
- Miller's Anesthesia, 10e, Box 54.2
Other validated tools include the Epworth Sleepiness Scale (ESS) (score >10 = excessive daytime sleepiness) and the Berlin Questionnaire. The AASM emphasizes that these tools are for risk stratification, not diagnosis.
5. Diagnostic Testing: PSG vs. HSAT
Recommendation 1 (STRONG): No Diagnosis by Questionnaire Alone
Clinical tools, questionnaires, and prediction algorithms should not be used to diagnose OSA without PSG or HSAT.
Recommendation 2 (STRONG): PSG or HSAT for Uncomplicated Patients
For uncomplicated adults at increased risk of moderate-to-severe OSA:
- Either PSG or HSAT with a technically adequate device is acceptable
"Uncomplicated patient" is defined by the absence of:
- Significant cardiorespiratory disease
- Potential respiratory muscle weakness (neuromuscular disease)
- Awake hypoventilation or suspected sleep-related hypoventilation
- Chronic opioid use
- History of stroke
- Severe insomnia
Recommendation 3 (STRONG): Negative/Inconclusive HSAT → Get PSG
If a single HSAT is negative, inconclusive, or technically inadequate, polysomnography must be performed.
Technical adequacy for HSAT requires a minimum of 4 hours of adequate oximetry and flow data encompassing the habitual sleep period.
Recommendation 4 (STRONG): PSG Required for Complex/Comorbid Patients
PSG, rather than HSAT, must be used when any of the following are present:
| Condition | Rationale |
|---|---|
| Significant cardiorespiratory disease (e.g., HF, severe COPD) | HSAT underestimates AHI; needs full monitoring |
| Neuromuscular disease (respiratory muscle weakness) | May have hypoventilation not captured by HSAT |
| Awake hypoventilation / suspected sleep-related hypoventilation | Needs CO2 monitoring (transcutaneous or end-tidal) |
| Chronic opioid use | Atypical breathing patterns including CSA |
| History of stroke | Complex sleep architecture; high CSA risk |
| Severe insomnia | Poor sleep may render HSAT uninterpretable |
Recommendation 5 (WEAK): Split-Night Protocol Acceptable
A split-night PSG (combined diagnostic + CPAP titration in one night) may be used if:
- Moderate-to-severe OSA observed during ≥ 2 hours of diagnostic recording, AND
- ≥ 3 hours remain for CPAP titration
6. Polysomnography - Technical Overview
PSG is the gold standard and monitors:
| Parameter | Signal |
|---|---|
| Sleep staging | EEG (electroencephalography) |
| Eye movements | EOG (electro-oculography) |
| Muscle tone | EMG (chin and tibialis anterior) |
| Airflow | Nasal pressure transducer + thermistor |
| Respiratory effort | Respiratory inductance plethysmography (chest/abdomen) |
| Oxygen saturation | Pulse oximetry (SpO2) |
| Cardiac rhythm | ECG |
| Snoring | Microphone |
| Body position | Actigraphy |
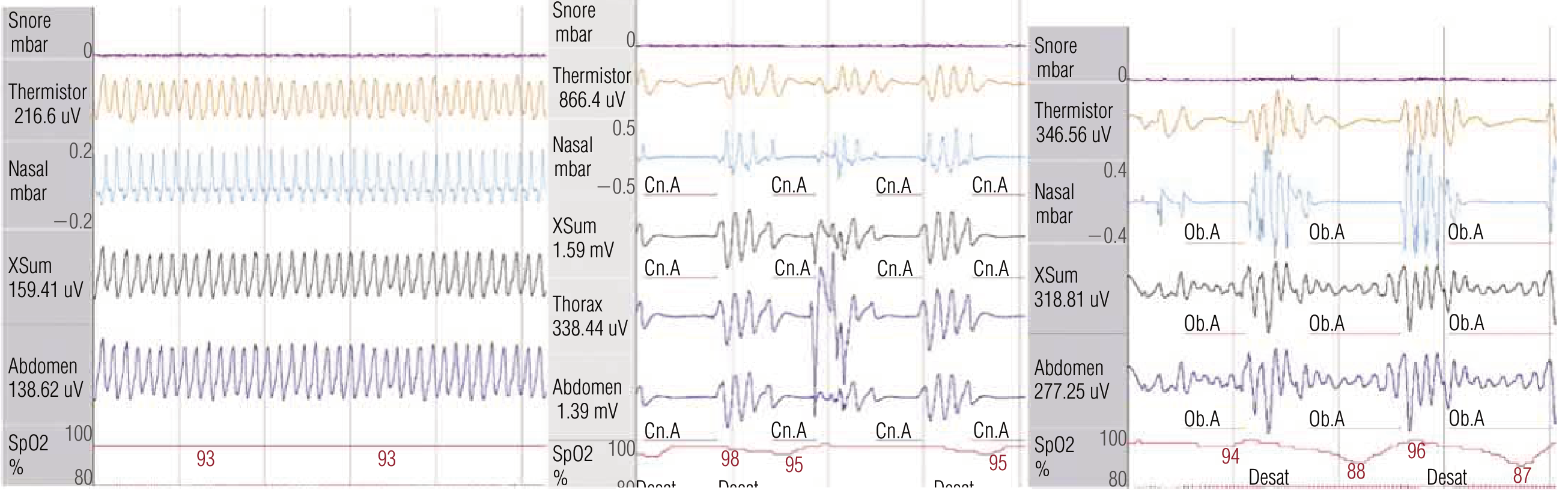
The figure below from a sleep study shows the three key patterns - normal breathing (left), central apneas (Cn.A, middle), and obstructive apneas (Ob.A, right) with the characteristic deep desaturations:
HSAT Devices
HSAT uses fewer channels. Accepted configurations include:
- Peripheral arterial tonometry (PAT) + oximetry + actigraphy (e.g., WatchPAT)
- Cardiorespiratory channels: airflow + respiratory effort + oximetry + HR
- Some newer devices include a single EEG channel
Key limitation: HSAT calculates the respiratory event index (REI) as events per recording time (not per sleep time), which typically underestimates AHI by ~12% - larger discrepancies in poor sleepers, HF patients, and women.
7. Oximetry Alone: Not Sufficient
Overnight pulse oximetry alone is insufficient to diagnose OSA because:
- Single-channel measurement - cannot classify event type
- Cannot distinguish apnea from hypopnea from hypoventilation
- Normal oximetry does not exclude OSA
Its role is limited to: (1) identifying patients who may benefit from formal sleep testing, and (2) monitoring treatment efficacy. - Murray & Nadel's Respiratory Medicine
8. Inpatient Screening (AASM 2025 Guideline - New)
The 2025 AASM guideline (Mehra et al., JCSM 2025 - PMID: 40838698) addresses a previously uncharted area:
- Recommendation 1 (Conditional): For medically hospitalized adults at increased OSA risk, the AASM suggests in-hospital screening as part of a care management pathway incorporating diagnosis and PAP treatment - rather than no screening
- Screening may include validated questionnaires and/or overnight high-resolution pulse oximetry
- Recommendation 4 (Conditional): A discharge management plan should be arranged for at-risk/diagnosed patients to ensure timely outpatient diagnosis and effective OSA management
- Good Practice Statement: For hospitalized patients already on PAP therapy, existing treatment should be continued rather than withheld unless contraindicated
9. Algorithm Summary
Clinical suspicion (snoring, EDS, witnessed apneas, HTN, obesity)
↓
Screening questionnaire (STOP-Bang, Berlin, ESS) + clinical assessment
↓
Increased risk confirmed?
↓ YES
Is patient "uncomplicated"?
↓ YES ↓ NO (complex comorbidities)
HSAT or PSG PSG only
↓
HSAT result:
Positive → Diagnose, treat
Negative/Inconclusive → Proceed to PSG
↓
PSG → AHI interpretation → Severity grading → Treatment
Key References
- AASM 2017 Diagnostic Testing Guideline - Kapur VK et al., J Clin Sleep Med 2017 (primary source for recommendations above)
- Mehra R et al. AASM 2025 inpatient OSA guideline. J Clin Sleep Med 2025 (PMID: 40838698)
- AASM Manual for Scoring Sleep and Associated Events, Version 3, 2023
- Braunwald's Heart Disease, Table 89.1 and Figure 89.1
- Miller's Anesthesia, 10e, Box 54.2 (STOP-Bang)
- Murray & Nadel's Respiratory Medicine - Diagnostic Sleep Testing chapter
This is a shared conversation. Sign in to Orris to start your own chat.