Mri report of my mother having back pain from past 2 years which is radiating to left leg. This pain increases on walking and she is unable to continue further walk
Reading File
Reading File
Running Command
cd /home/daytona/workspace/attachments/5f737868-3574-42b1-a7c5-2b8d9d6acb95 && p…
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Searching PubMed
lumbar spinal stenosis treatment conservative surgery
Loading Image
I now have everything needed for a complete, plain-language explanation. Here is the full breakdown:
MRI Report of Mrs. Dilshada - Plain Language Explanation
Date of scan: 16 June 2026 | Age: 45 years, Female | Radiologist: Dr. Obaid Ashraf, MD Radiodiagnosis
What the MRI Found - Finding by Finding
1. Reduced Lumbar Lordosis
The spine normally has a gentle inward curve (lordosis) in the lower back. Your mother's curve is flattened. This is usually a result of chronic muscle spasm and pain - the back muscles tighten and straighten the spine as a protective reflex. It is a secondary sign, not a separate disease.
2. Disc Desiccation at L1-L2, L4-L5, and L5-S1
Think of spinal discs as jelly-filled cushions between each vertebra. They are mostly water when healthy. "Desiccation" means they have dried out and lost their water content - a normal part of ageing, but accelerated by wear and tear. Dried-out discs are thinner, less springy, and more prone to bulging. The three levels affected are:
- L1-L2 - upper lumbar spine
- L4-L5 and L5-S1 - the lower two levels, which bear the most body weight and are the most commonly affected in the general population
3. Schmorl's Nodes (Multiple Levels)
These are small pockets where the disc material has pushed up or down into the vertebral bone above or below it - like a small dent in the end of the bone. They are usually a sign of past mechanical stress. Most Schmorl's nodes cause no symptoms by themselves.
4. Modic Type II Endplate Changes at L5-S1
The "endplate" is the thin layer of cartilage between each disc and the vertebral bone. Modic Type II changes mean the bone marrow directly adjacent to the disc has been replaced with fatty tissue - a sign of chronic disc degeneration and stress at that level. It is associated with chronic low back pain.
5. Diffuse Disc Bulges at L4-L5 and L5-S1 - THE MAIN PROBLEM
This is the most important finding and the direct cause of your mother's leg pain.
A disc bulge means the outer wall of the disc has expanded outward in all directions (like a burger bun being squeezed). At these two levels, the bulging disc is pressing on:
- The spinal canal (central stenosis) - the tunnel that the nerve bundle travels through
- The lateral recess and foramina (side openings) - the exits through which individual nerve roots leave the spine
The report says this causes:
- Bilateral lateral recess stenosis - narrowing of the nerve root canals on both sides
- Foraminal stenosis - narrowing of the exit holes for individual nerves
- Mild acquired canal stenosis - mild narrowing of the central spinal canal
- Abutment of bilateral traversing nerve roots - the bulging disc is actually touching/pressing on the nerve roots on both sides
The thecal sac (the fluid-filled tube containing all the spinal nerves) diameter at L4-L5 is only 7 mm - significantly narrowed. Normal is typically >12 mm.
This pressing on the nerves at L4-L5 and L5-S1 is what causes pain radiating down to the left leg, and the inability to walk far.
6. Central Disc Protrusion at L1-L2
At the upper lumbar level, the disc has not just bulged uniformly but has pushed out focally (protrusion). This is compressing the thecal sac (the main nerve sac). Importantly, the report says there is no significant lateral recess narrowing here - meaning the individual nerve exits are not pinched at this level. This may be contributing to some back pain but is less responsible for the leg symptoms than L4-L5/L5-S1.
7. Facet Joint Arthropathy + Ligamentum Flavum Hypertrophy at L4-L5 and L5-S1
This is a "triple hit" at these two levels:
| Structure | What's happening | Effect |
|---|---|---|
| Disc | Bulging forward | Pinches nerve from the front |
| Facet joints (small joints at the back of spine) | Arthritic, enlarged | Pinches nerve from the side/back |
| Ligamentum flavum (yellow ligament inside spine) | Thickened/hypertrophied | Pinches nerve from behind |
This is exactly the picture shown in the textbook image below, which is a real MRI of degenerative spinal stenosis at L4-L5 - very similar to your mother's condition:
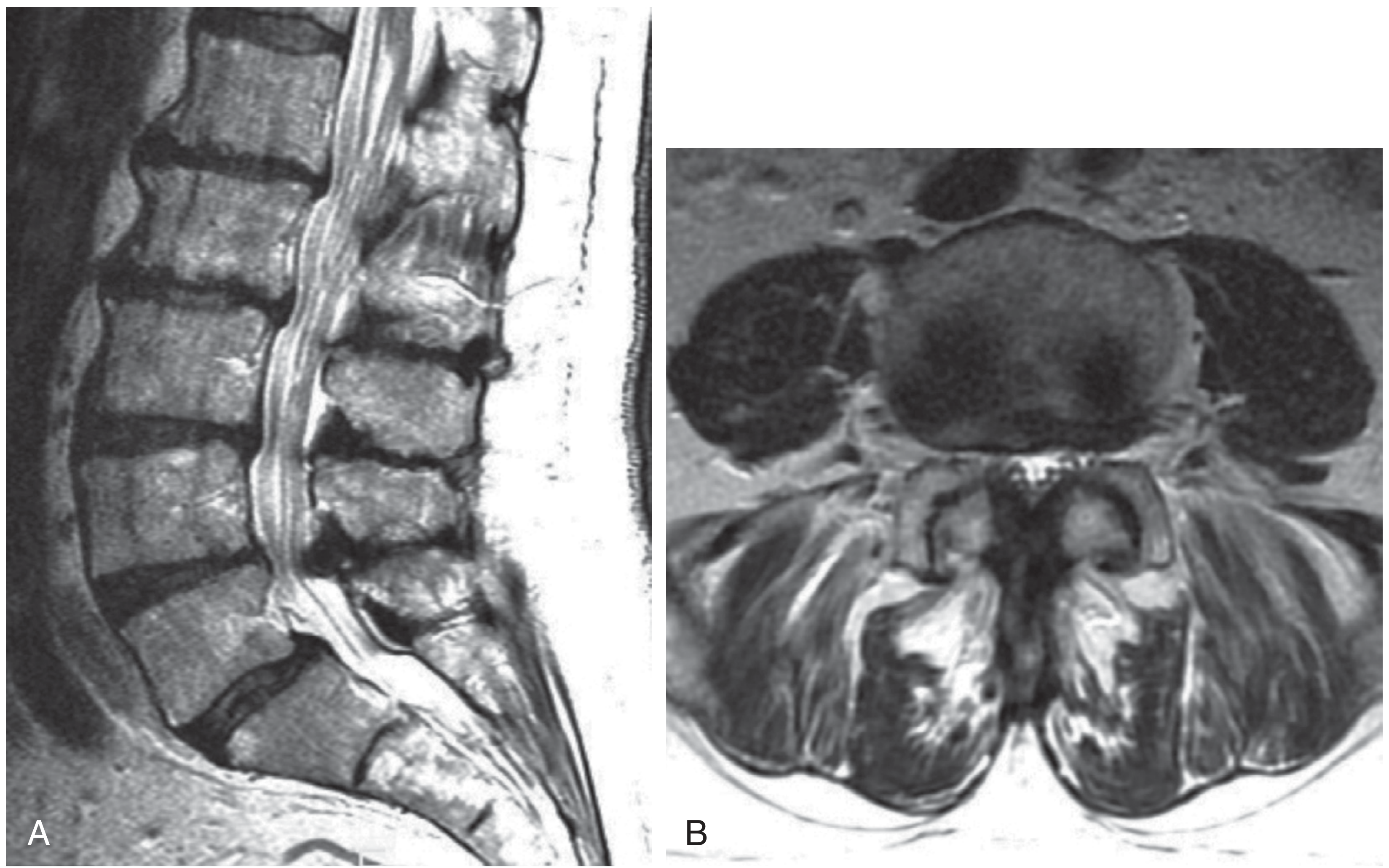
Left: Side view showing narrowing at L4-L5. Right: Cross-sectional view showing how the thecal sac (nerve bundle) is being squeezed by disc bulge and facet hypertrophy.
Why Pain Gets Worse on Walking - Neurogenic Claudication
Your mother's symptom - back and leg pain that comes on or worsens after walking a certain distance, forcing her to stop - has a specific medical name: neurogenic claudication (also called pseudoclaudication).
As per Firestein & Kelley's Textbook of Rheumatology:
"Neurogenic claudication is induced by standing erect or walking and relieved by sitting or flexing forward. This forward flexion increases the spinal canal dimensions."
Here is why this happens:
- When standing/walking upright: the lumbar spine slightly extends (arches backward). This makes the spinal canal even narrower, squeezing the already-compressed nerves more. Blood flow to the nerve roots is also temporarily reduced.
- When sitting or leaning forward: the canal opens up slightly, pressure on nerves is relieved, and pain subsides.
This is why many patients find they can walk much longer if they push a shopping cart (slightly bent forward) than if they walk upright - this is actually called the "shopping cart sign" in medical literature. If your mother finds relief by sitting down or leaning forward, this confirms the diagnosis.
Summary - What Does Your Mother Have?
Degenerative Lumbar Spinal Stenosis - primarily at L4-L5 and L5-S1, caused by a combination of:
- Dried-out, bulging discs
- Arthritic facet joints
- Thickened ligaments
All three are squeezing the spinal canal and nerve roots at the most critical levels. This is causing:
- Chronic low back pain (2 years)
- Left leg pain/sciatica (nerve root compression)
- Neurogenic claudication (worsening pain with walking)
What Happens Next - What Can Be Done
The good news from Firestein & Kelley's Rheumatology textbook is that this condition has a mostly benign natural history - in a long-term follow-up study, 70% of patients remained stable, 15% improved, and only 15% worsened without surgery.
Conservative (Non-surgical) Treatment First
Most patients are managed without surgery initially:
- Physiotherapy - core strengthening, lumbar flexion exercises (these open up the canal)
- NSAIDs / pain medications - as prescribed by her doctor
- Epidural steroid injections - can provide temporary relief by reducing nerve inflammation
- Activity modification - walking with a slightly forward lean, using a walker or stick
- Weight management - reduces load on the lower spine
When Surgery is Considered
Surgery becomes an option if:
- Conservative treatment fails after a fair trial (usually 3-6 months)
- Symptoms are severely affecting quality of life
- There is progressive weakness in the legs
- Bladder/bowel symptoms develop (this would be urgent)
The standard surgery is decompressive laminectomy - removing the bone and thickened ligament pressing on the nerves. Per Miller's Review of Orthopaedics, the SPORT trial (a major clinical trial) showed significant improvement in pain and function for surgical vs. non-surgical groups at 4-year follow-up.
A recent 2025 network meta-analysis (PMID 39577647) reviewing different interventions for lumbar spinal stenosis is the most current evidence on treatment options.
Important Note
This explanation is to help you understand the MRI report. The radiologist has correctly noted this is not a final diagnosis and must be correlated with clinical findings. Please show this report to a spine specialist (orthopedic surgeon or neurosurgeon) or a neurologist who will examine your mother, assess her nerve function, and decide the best treatment plan.
Red flag symptoms - if your mother develops any of the following, seek emergency care immediately:
- Inability to control bladder or bowel
- Sudden severe weakness or numbness in both legs
- Numbness in the groin/inner thigh area (saddle anesthesia)
These could indicate cauda equina syndrome, which requires urgent surgical decompression.
Where should we do surgery in neurosurgeon superspeciality or orthopedic surgery
Searching PubMed
lumbar spinal stenosis outcomes neurosurgery orthopedic spine surgery comparison
Searching the Web
neurosurgeon vs orthopedic surgeon lumbar spine surgery who is better for spinal stenosis
This is a very common and important question. Here is a clear, honest answer:
Neurosurgeon vs. Orthopedic Spine Surgeon - Which One for Your Mother?
The Short Answer
For your mother's condition - lumbar spinal stenosis with disc bulge and nerve compression - both a neurosurgeon and an orthopedic spine surgeon are equally qualified to perform the surgery. The outcomes are comparable between the two specialties when the surgeon has dedicated spine training.
The more important question is not which specialty but which surgeon - specifically, one who focuses primarily on spine surgery.
What Each Specialty Brings
| Neurosurgeon | Orthopedic Spine Surgeon | |
|---|---|---|
| Training focus | Brain, spinal cord, nerves, microsurgical technique | Bones, joints, structural spine mechanics |
| Spine procedures | Decompression, discectomy, nerve surgery | Decompression, fusion, structural correction |
| Strength for your mother's case | Nerve decompression, microsurgery around nerve roots | Mechanical stability, spinal reconstruction if fusion needed |
| For lumbar stenosis specifically | Excellent | Excellent |
As Spine-health.com summarizes - for procedures like lumbar decompression (laminectomy), discectomy, and single-level fusion, both specialties are equally well qualified, and outcomes data from large national databases shows no significant difference.
For Your Mother's Specific Condition
Her MRI shows:
- Disc bulge pressing on nerves at L4-L5 and L5-S1
- Thickened ligamentum flavum and facet arthropathy squeezing the canal
- No spinal cord tumor, no complex deformity, no scoliosis
This is a standard degenerative lumbar stenosis case - the bread-and-butter surgery for both specialties. The operation she would most likely need is a laminectomy (decompression) - removing the overgrown bone/ligament to give nerves more space.
A real-world database study found that orthopedic surgeons actually perform more lumbar fusions and decompression surgeries than neurosurgeons, while neurosurgeons perform more cervical (neck) spine and intradural (inside the nerve covering) surgeries. Neither group had meaningfully different patient outcomes or hospital stay lengths for standard lumbar procedures.
When a Neurosurgeon Has an Edge
- If the problem is inside the spinal cord itself (tumor, syrinx, tethered cord)
- Complex nerve microsurgery
- Cervical spine with spinal cord involvement (myelopathy)
Your mother does NOT have any of these based on the MRI.
When an Orthopedic Spine Surgeon Has an Edge
- Complex spinal deformity or scoliosis
- Multi-level fusion with instrumentation (rods and screws)
- Structural reconstruction
Your mother's case may or may not need fusion depending on what the surgeon finds clinically.
Practical Advice - What to Actually Do
-
Seek a "spine specialist" specifically - not just any orthopedic surgeon or any neurosurgeon. Ask: "Do you specialize in spine surgery? How many lumbar decompressions do you do per year?"
-
A surgeon who does 100+ spine surgeries a year at a well-equipped hospital is far more important than the specialty label.
-
Ideally visit both - get a consultation from one of each and compare their assessment and surgical plan. If both recommend the same approach, that gives confidence.
-
Look for a hospital with a dedicated spine unit or spine center - these often have both specialties working together in a multidisciplinary setup, which gives the best outcomes.
-
Do not rush into surgery - your mother should first complete a proper trial of conservative treatment (physiotherapy, pain medications, possibly an epidural steroid injection). Surgery is considered only if that fails after a few months, unless she develops weakness or bladder/bowel issues.
Bottom Line
For your mother's lumbar disc bulge and spinal stenosis: either specialty is fine as long as the surgeon is an experienced, fellowship-trained spine surgeon who performs these operations regularly. In India, both Orthopedic Spine Surgeons and Neurosurgeons at tertiary hospitals and superspeciality centers routinely handle cases exactly like hers with good results. Trust the surgeon's experience and volume over the specialty name on the door.
She is taking pregabalin, NSAIDS for past 1 yrs
Finding Sources
Finding Sources
Searching PubMed
pregabalin lumbar radiculopathy spinal stenosis long term
Searching the Web
long term NSAID use side effects risks kidney stomach 1 year chronic back pain
This is very important information. Here is what 1 year of these medications means for your mother:
One Year on Pregabalin + NSAIDs - What This Means
The Critical Point: Conservative Treatment Has Already Failed
Standard medical guidelines consider a 3-6 month trial of conservative treatment (medications + physiotherapy) as the minimum before considering surgery. Your mother has been on medications for 1 full year - that is double the typical trial period.
If she is still having back pain, leg pain, and inability to walk despite 1 year of treatment, this is a strong signal that medications alone are not solving her problem.
This is a legitimate reason to now seriously discuss surgery with a spine specialist.
What Pregabalin Does (and Its Limitations)
Pregabalin (brand name Lyrica) works by calming overactive nerve signals. It is used for neuropathic (nerve) pain - the burning, shooting, electric pain that radiates down the leg. It does NOT treat the underlying cause. It does not shrink the disc, open the spinal canal, or reverse the nerve compression.
After 1 year, if pregabalin is not giving adequate relief, continuing it further is unlikely to suddenly start working. Long-term pregabalin use can also cause:
- Dizziness and unsteadiness (especially dangerous for someone already struggling to walk)
- Weight gain (which worsens spine load)
- Drowsiness and mental fog
- Dependence - it cannot be stopped suddenly
What NSAIDs for 1 Year Have Done to Her Body
This is the most concerning part and needs immediate attention from her doctor.
NSAIDs (like ibuprofen, diclofenac, naproxen, etoricoxib) are defined as long-term when taken more than 3 times a week for more than 3 months. Your mother has taken them for 12 months. The risks by now are real:
| Organ | Risk after Long-Term NSAID Use |
|---|---|
| Stomach/GI tract | Gastric ulcers, gastritis, GI bleeding - can be silent (no symptoms until bleeding occurs) |
| Kidneys | Reduced blood flow to kidneys, possible chronic kidney damage |
| Heart | Increased risk of high blood pressure, fluid retention, heart attack risk (especially with age) |
| Liver | Mild elevation of liver enzymes with prolonged use |
Per Mayo Clinic, NSAIDs also have a ceiling effect - above a certain dose they do not control pain any better, but the side effect risk keeps rising.
What she should do RIGHT NOW regarding NSAIDs:
- Tell her doctor she has been on NSAIDs for 1 year - a blood test for kidney function (creatinine, urea) and a check for stomach issues should be done
- She should be on a stomach-protecting tablet (like pantoprazole or omeprazole) if she is not already - anyone on NSAIDs for more than a few weeks needs this
- Do not stop NSAIDs suddenly on your own - reduce gradually under doctor's guidance
Where Things Stand Now - A Clear Picture
Duration of back/leg pain: 2 years
Medications tried: Pregabalin + NSAIDs
Duration of medication trial: 1 year ✓ (more than enough)
Pain still present: Yes
Walking still limited: Yes
MRI findings: Significant nerve compression at L4-L5, L5-S1
By standard spine care guidelines, your mother now qualifies for surgical evaluation. One year of failed medical therapy, combined with structural nerve compression visible on MRI and functional limitation (unable to walk), meets the criteria for considering surgical decompression.
What the Next Steps Should Be
Step 1 - Spine Specialist Consultation (This Week)
Book an appointment with a spine surgeon (neurosurgeon or orthopedic spine surgeon as discussed). Bring:
- The MRI report and films (CD/pen drive)
- List of current medications and how long she has been on them
- Description of symptoms: when pain started, what makes it worse, how far she can walk
Step 2 - Tests the Doctor Will Likely Order
- Nerve conduction study / EMG - to check how much nerve damage has already occurred from 2 years of compression
- X-ray of lumbar spine - to assess bone alignment and rule out instability
- Blood tests - kidney function, liver function (given 1 year of NSAIDs)
Step 3 - One More Conservative Option (if surgeon agrees)
Before surgery, if she has NOT yet had an epidural steroid injection (ESI), this can be tried. It involves injecting a steroid directly near the compressed nerve under X-ray guidance. According to the radiology textbook in the medical library, spinal injections are indicated for pain relief in patients with degenerative spinal canal stenosis. Some patients get significant relief for months from a single injection. However, if she has already tried this, or if the surgeon feels the compression is too severe, surgery is the logical next step.
Step 4 - Surgery Discussion
Given 1 year of failed medication, she is a genuine surgical candidate. The surgeon will weigh:
- Her age (45 - relatively young, which actually favors surgery as she has many active years ahead)
- Severity of nerve compression on MRI (significant at L4-L5 with 7mm canal)
- Degree of functional disability (unable to walk)
- Whether she needs just decompression (laminectomy) or decompression + fusion
Bottom Line
1 year on pregabalin + NSAIDs without adequate relief, in the presence of significant MRI findings, is a clear indication to move beyond medications. Please consult a spine surgeon soon. Also ask her treating doctor to check her kidney function and stomach health given the prolonged NSAID use - that health check should not wait.
This is a shared conversation. Sign in to Orris to start your own chat.