pelvic floor anatomy and hip flexors anatomy and how psoas major and related muscles are responsible for back pain. Showcase everything with relevant images.
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching the Web
psoas major anatomy back pain mechanism hip flexors pelvic floor relationship
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
I have all the core content and images needed. Let me also fetch the posterior abdominal wall image from the Thieme atlas (iliopsoas with full labeling) to complete the visual coverage.
Now I have everything needed for a comprehensive response. Let me compile it all.
Pelvic Floor Anatomy, Hip Flexors, and the Psoas Major in Back Pain
Part 1 - Pelvic Floor Anatomy
The pelvic floor separates the pelvic cavity from the perineum. It is a muscular and fascial structure, sometimes called the pelvic diaphragm, formed primarily by two levator ani muscles that meet in the midline via a connective tissue raphe.
(Gray's Anatomy for Students, p. 503)
Key Components
| Structure | Description |
|---|---|
| Levator ani | Large paired muscle; largest component of the pelvic diaphragm |
| Puborectalis | Arises from back of pubic symphysis; forms a U-shaped sling around anorectal junction |
| Pubococcygeus | Originates from posterior pubis and arcus tendineus; forms sling around vagina/urethra (pubovaginal muscles) |
| Iliococcygeus | Arises from ischial spine and obturator fossa; inserts on sacrum, coccyx, and anococcygeal raphe |
| Coccygeus | Posterior muscle, overlies sacrospinous ligament; completes the diaphragm posteriorly |
| Perineal membrane | Thick triangular fascial sheet spanning the pubic arch; provides anterior support |
| Deep perineal pouch | Narrow region superior to perineal membrane |
(Campbell-Walsh-Wein Urology, p. 3214-3215)
Pelvic Floor - Funnel-Shaped Anatomy
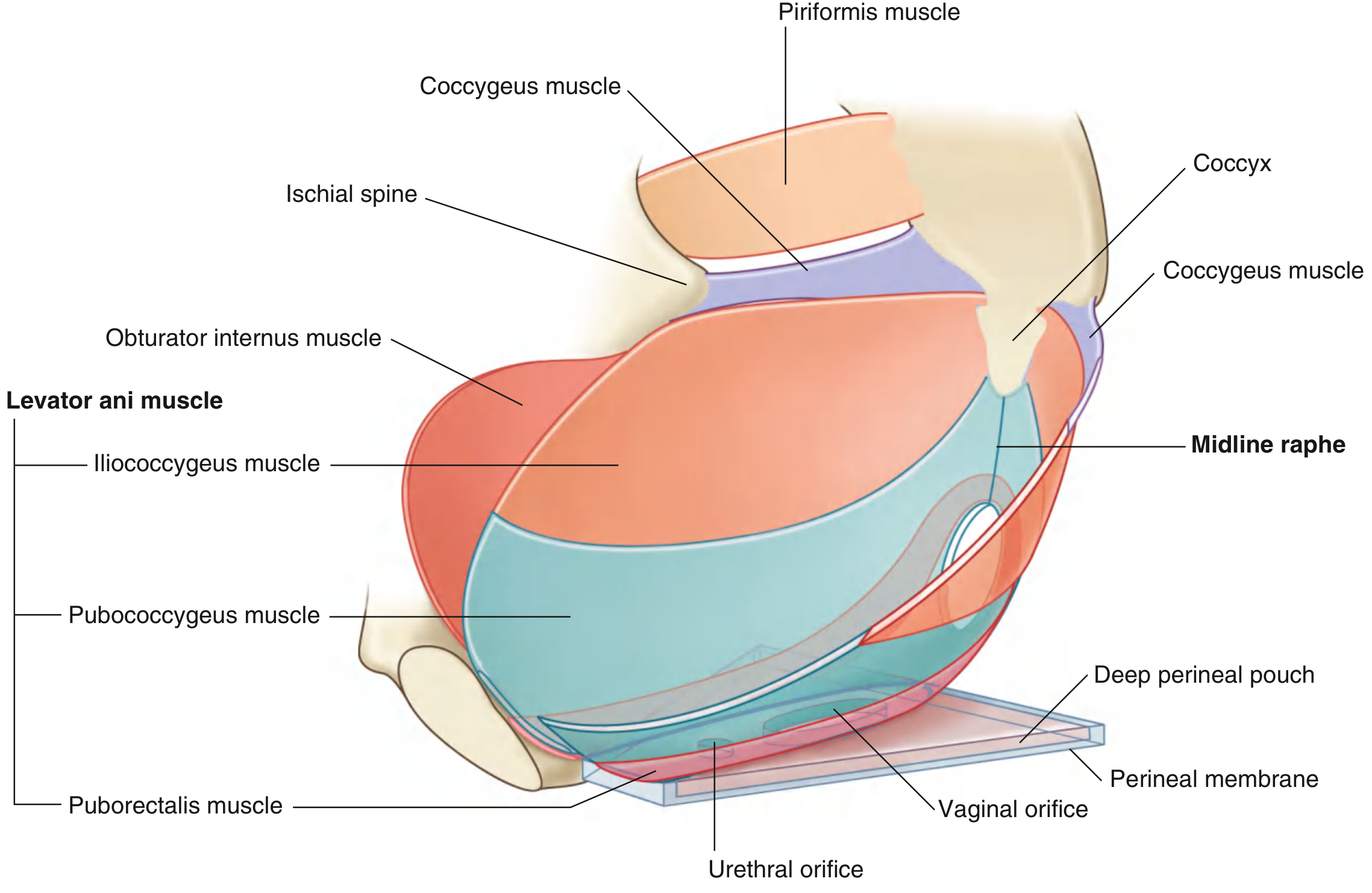
Fig. 5.7 - Pelvic Floor (Gray's Anatomy for Students). The bowl-shaped pelvic diaphragm with the three components of levator ani visible - note the U-shaped levator hiatus anteriorly for passage of the urethra and vagina.
Levator Hiatus and Functional Role
The opening of the levator ani group is the levator hiatus, which allows passage of the urethra, vagina, and rectum. The levator plate - formed by fusion of levator ani muscles in the midline - acts as a shelf on which the viscera rests. Weakening of these muscles causes this plate to sag, opening the hiatus and predisposing to pelvic organ prolapse.
The sustained resting tone of the pelvic floor:
- Supports pelvic viscera
- Resists increases in intra-abdominal pressure
- Provides passive control of urinary and fecal continence
(Campbell-Walsh-Wein Urology, p. 3215)
Innervation
The levator ani receives innervation from the levator ani nerve originating from S3, S4, and S5, traveling medial to the ischial spine and the arcus tendineus levator ani (ATLA). Earlier teaching attributed innervation to branches of the pudendal nerve, but recent studies confirm the levator ani nerve as the primary source.
Pelvic Fascia and Ligamentous Support
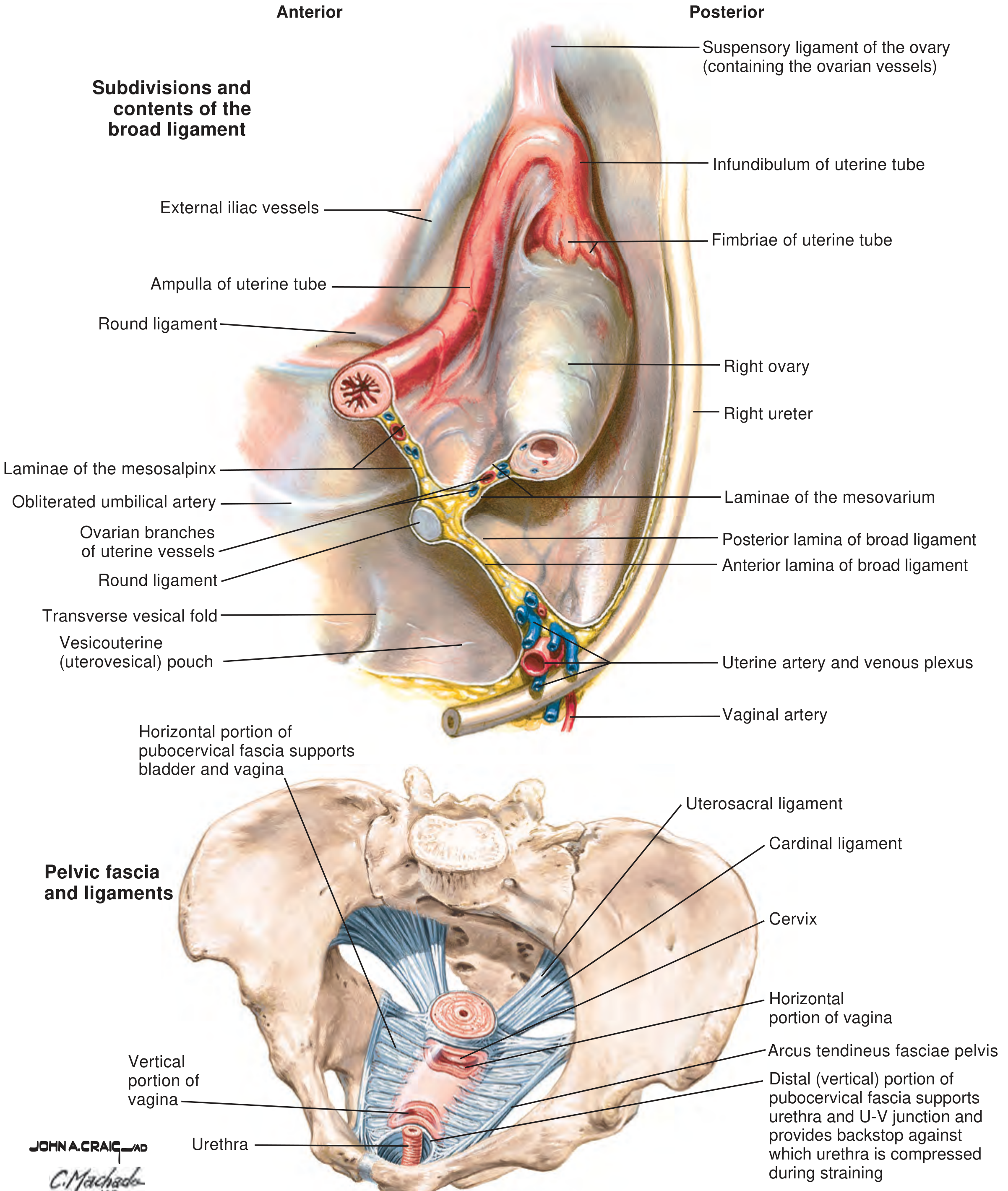
From Campbell-Walsh-Wein Urology - Pelvic fascia and ligaments showing the pubocervical fascia supporting the bladder and vagina, the arcus tendineus fasciae pelvis, and key ligamentous supports (uterosacral, cardinal). Note how the distal (vertical) portion of pubocervical fascia provides a backstop against which the urethra is compressed during straining - a critical continence mechanism.
Part 2 - Hip Flexor Anatomy
The hip flexors are a group of muscles crossing the anterior hip joint. The primary ones are:
| Muscle | Origin | Insertion | Nerve |
|---|---|---|---|
| Psoas major | T12-L5 vertebral bodies & intervertebral disks (superficial); L1-L5 costal processes (deep) | Lesser trochanter (via iliopsoas) | Lumbar plexus L1-L4 |
| Iliacus | Iliac fossa | Lesser trochanter (via iliopsoas) | Femoral nerve L2-L4 |
| Rectus femoris | Anterior inferior iliac spine (AIIS) | Tibial tuberosity via patella | Femoral nerve L2-L4 |
| Sartorius | Anterior superior iliac spine (ASIS) | Pes anserine (medial tibia) | Femoral nerve L2-L3 |
| Tensor fasciae latae | Iliac crest / ASIS | Iliotibial band | Superior gluteal nerve L4-L5 |
(General Anatomy and Musculoskeletal System - THIEME Atlas, p. 476-501)
The iliopsoas is the most powerful hip flexor - psoas major and iliacus join and share a common insertion on the lesser trochanter of the femur.
Posterior Abdominal Wall - Psoas Major and Iliacus
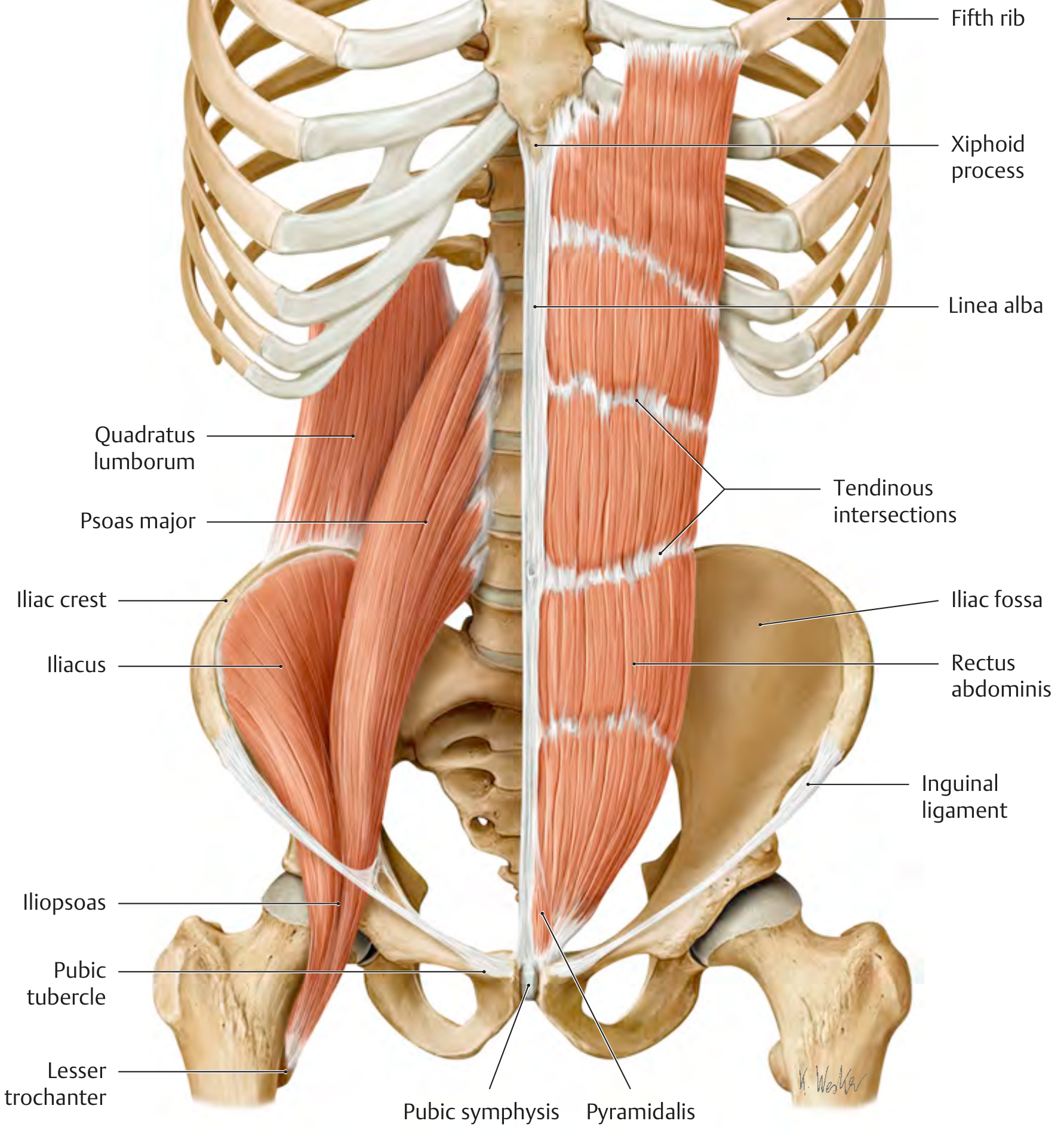
THIEME Atlas - Anterior and posterior abdominal wall muscles. Left side shows psoas major descending from the lumbar spine alongside the iliacus muscle from the iliac fossa, converging as the iliopsoas to insert on the lesser trochanter. This image beautifully demonstrates why a tight psoas pulling on L1-L5 can exert direct traction on the lumbar spine.
Hip Muscles - Iliopsoas with Bony Landmarks
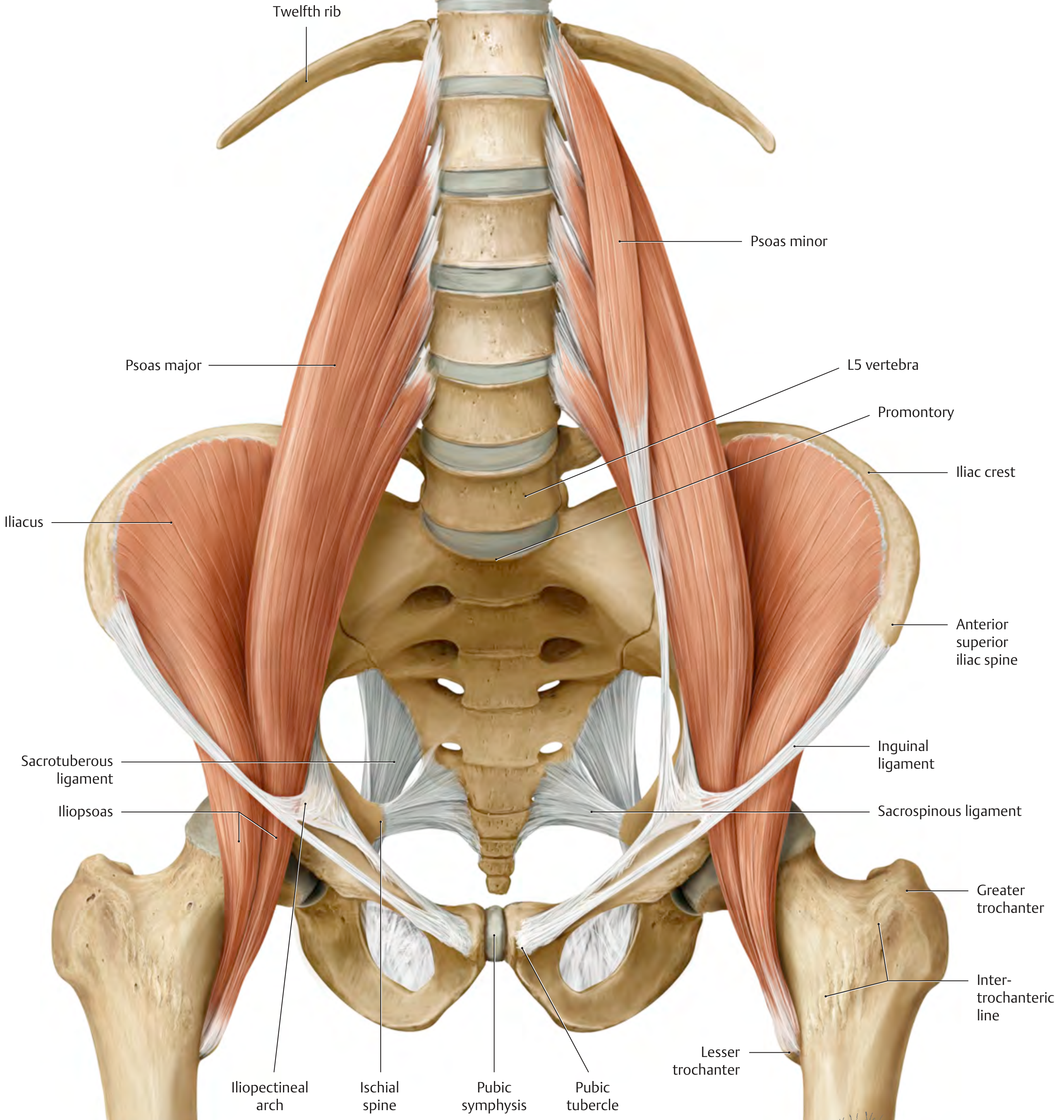
THIEME Atlas - Inner hip muscles, anterior view. This is the definitive view of the iliopsoas apparatus. The psoas major originates from T12-L5 and the iliacus from the iliac fossa; they converge as the iliopsoas and pass under the inguinal ligament via the iliopectineal arch to insert on the lesser trochanter.
Iliopsoas as a Postural Muscle
The iliopsoas is classified as a postural muscle with predominantly slow-twitch (type I) fibers, making it inherently susceptible to pathological shortening - particularly in older patients or those with sedentary lifestyles. Regular stretching is required to maintain normal tone.
Shortening (contracture) of the hip flexors causes a cascade:
- Increased anterior pelvic tilt
- Increased lumbar lordosis
- Limitation of hip extension
(THIEME Atlas, p. 501)
Part 3 - Psoas Major and Back Pain
Anatomy That Creates the Problem
The psoas major is unique because it has dual attachment to the spine AND the femur. Its superficial layer attaches to the lateral surfaces of T12 through L4 vertebral bodies and the intervertebral disks between them. Its deep layer attaches to the costal (transverse) processes of L1-L5.
"Can you imagine how it feels for a tight psoas to be yanking on your L4 disc?" - this is not an exaggeration. A chronically shortened psoas muscle directly loads the intervertebral disks at T12-L5.
Mechanisms of Back Pain
1. Lumbar Spine Compression and Hyperlordosis
A psoas spasm causes direct compression of the lumbar spine through excessive compressive forces. This leads to hyperlordosis (exaggerated lumbar curve) and shearing stress at the lumbosacral junction (L5-S1). The biomechanical model described by McGill compares lumbar stability to a fishing rod with guy wires - reducing tension in any one muscle (wire) allows the spinal segment (rod) to buckle and predispose to injury.
2. Pelvic Torsion
Unilateral shortening of the iliopsoas tilts the ilium on the affected side forward, causing pelvic torsion - the pelvis becomes twisted upon itself. This directly alters sacroiliac joint function, the intervertebral joints, and the lumbosacral junction, with degenerative changes in vertebral bodies over time.
(THIEME Atlas, p. 500-501)
3. Lumbar Disk Herniation
In most patients with lumbar disk herniation, significant atrophy of the psoas major on the affected side occurs. The muscle loses its stabilizing role, allowing abnormal segmental motion and worsening disk pathology. Whether atrophy causes the herniation or follows it is debated, but the association is strong.
(Imaging Anatomy Atlas Vol. 3, p. 259)
4. Restriction of Thoracic Diaphragm Movement
The psoas major is continuous via fascia with the medial arcuate ligament and the thoracic diaphragm's crura. A psoas spasm can restrict diaphragm movement, causing a cascade that potentially causes more disability in the back muscles than many other conditions. The psoas fascia blends with the anterior longitudinal ligament superiorly and becomes continuous with the deep fascia of the pelvic floor inferiorly - linking the diaphragm, psoas, and pelvic floor into one functional unit.
(StatPearls - Anatomy, Bony Pelvis and Lower Limb: Psoas Major; PMC2796950)
5. Psoas Myofascial Pain Syndrome
Clinical presentation includes:
- Low back pain (often unilateral)
- Groin and pelvic pain
- Radiating pain toward the knee
- Difficulty walking and maintaining fully erect posture
- Pain with prolonged sitting (which shortens/cramps the muscle)
6. Snapping Hip Syndrome
The iliopsoas tendon can snap over the iliopectineal eminence as the hip moves from flexion to extension. This can be associated with labral pathology and bursitis, adding groin and anterior hip pain to the picture.
The Psoas-Pelvic Floor-Diaphragm Link
The psoas is not simply an isolated hip flexor. Its fascial connections form a vertical chain:
Thoracic Diaphragm (breathing)
↕ [medial arcuate ligament / crura fascia]
Psoas Major (T12 → lesser trochanter)
↕ [inferomedial fascia → pelvic floor fascia]
Pelvic Floor (levator ani, coccygeus)
A dysfunctional psoas can therefore:
- Alter respiratory mechanics by restricting diaphragm descent
- Affect intra-abdominal pressure regulation
- Transmit dysfunction into the pelvic floor - clinically relevant in patients with pelvic floor disorders, incontinence, and pelvic pain
Clinical Assessment
| Test | Findings in Psoas Dysfunction |
|---|---|
| Thomas Test | Hip flexion contracture on the affected side (ilium tilts forward) |
| Postural analysis | Increased lumbar lordosis, posterior pelvic tilt |
| Gait analysis | Shortened stride on the affected side |
| Functional squat | Pain or hip flexor weakness |
| Palpation | Deep anterior hip / retroperitoneal tenderness |
| Hip range of motion | Reduced active flexion and passive extension |
Related Hip Flexors Contributing to Back Pain
Beyond the psoas, other hip flexors contribute when shortened:
- Rectus femoris: Crosses both hip and knee; shortening pulls the AIIS forward, contributing to anterior pelvic tilt
- Tensor fasciae latae + IT band: Lateral hip tightness can cause lateral pelvic imbalance
- Quadratus lumborum: Not a hip flexor but directly attaches to L1-L4 transverse processes and the iliac crest; unilateral spasm is a classic cause of lateral low back pain and is often co-contracted with a tight psoas
Summary
The pelvic floor (levator ani complex) forms the base of the pelvis and provides sphincteric control and visceral support. The hip flexors - led by the iliopsoas - are the most powerful movers of the hip joint and are functionally inseparable from lumbar spine mechanics. The psoas major sits at the anatomical intersection of the thoracic spine, lumbar spine, pelvis, and hip, attaching to every lumbar vertebral body and disk. When it becomes tight or dysfunctional through prolonged sitting, weakness, or spasm, it directly compresses the lumbar spine, creates hyperlordosis, twists the pelvis, weakens disk integrity, and can even restrict breathing. It is one of the most clinically significant muscles in chronic low back pain, yet is one of the most overlooked.
Sources: Gray's Anatomy for Students - THIEME General Anatomy and Musculoskeletal System Atlas - Imaging Anatomy Atlas Vol. 3 - Campbell-Walsh-Wein Urology - StatPearls (Psoas Major) - PMC review of psoas biomechanics
This is a shared conversation. Sign in to Orris to start your own chat.