Holter monitoring - Loop recorders, Ambulatory blood pressure recording, Newer technologies for monitoring the patients with heart diseases. Make a explanation of this topics with images
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching the Web
Holter monitoring loop recorder ambulatory BP newer cardiac monitoring technologies 2024 overview
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Loading Image
Loading Image
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Searching the Web
Holter monitor ECG leads setup diagram patient
Loading Image
Loading Image
Searching the Web
ambulatory blood pressure monitor ABPM device 24 hour wrist
Loading Image
Loading Image
I now have all the material needed for a comprehensive, image-rich explanation. Let me compose the full response.
Cardiac Monitoring in Heart Disease: A Complete Guide
1. Holter Monitoring
What is Holter Monitoring?
Holter monitoring is continuous ambulatory electrocardiographic recording over 24-48 hours (and in newer devices, up to 2 weeks). Named after Dr. Norman J. Holter who developed it in the 1960s, it remains the cornerstone of outpatient rhythm assessment.
The patient wears skin electrodes connected by wires to a small digital recorder worn on a belt or shoulder strap. The device records 3 or more ECG channels continuously, while a computer with human oversight scans the data to generate a report capturing symptomatic events, asymptomatic arrhythmias, and ST-segment changes.
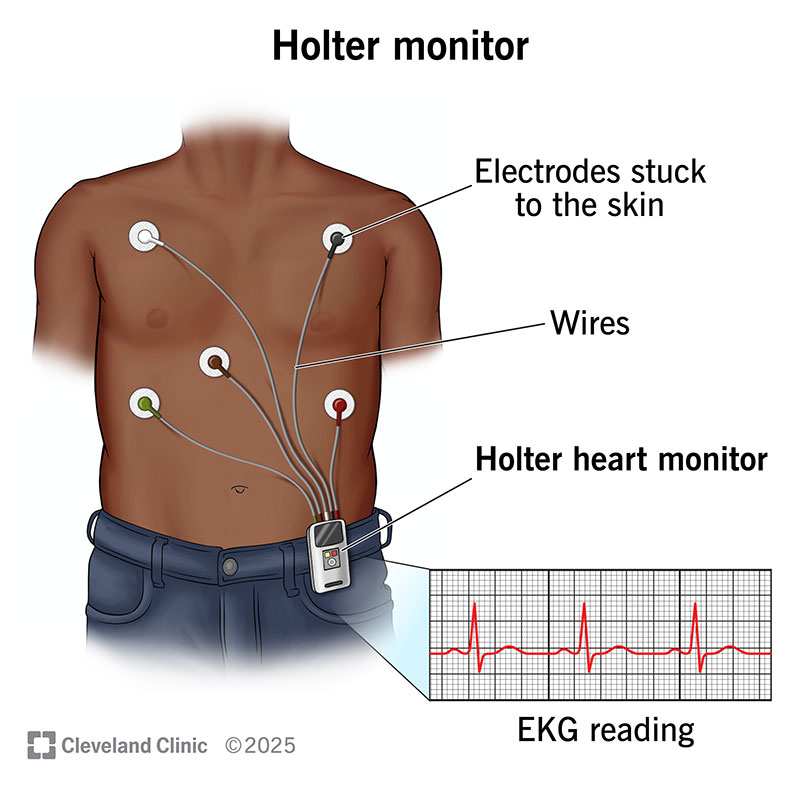
(Holter monitor setup: electrodes stuck to chest skin, connected via wires to the portable recording unit - Cleveland Clinic)
How it Works
- Electrodes placed on the chest capture the heart's electrical signals
- A recorder (about the size of a small smartphone) clips to a belt or hangs from a strap
- The patient keeps a symptom diary - logging the exact time of any palpitations, dizziness, or chest pain so these can be correlated with the ECG trace
- After 24-48 hours, the data is analysed
Clinical Uses
According to Braunwald's Heart Disease:
"Continuous electrocardiographic recorders include the traditional Holter monitor and digitally record three or more electrocardiographic channels for 24 to 48 hours. From 25% to 50% of patients experience a symptom during a 24-hour recording; in 2% to 15% the complaint is caused by an arrhythmia."
Key indications:
| Indication | Details |
|---|---|
| Arrhythmia diagnosis | Palpitations, syncope, presyncope with daily/frequent symptoms |
| Ischemia detection | Silent (asymptomatic) ischemic episodes - common in CAD |
| Drug therapy assessment | Monitoring efficacy and pro-arrhythmic effects of antiarrhythmic drugs |
| Post-MI surveillance | Risk stratification for ventricular arrhythmias |
| Pacemaker/ICD assessment | Evaluating device function |
| Pre-operative evaluation | Frequent ischemic episodes predict intraoperative/postoperative ischemia |
Key point from Morgan & Mikhail's Clinical Anesthesiology: "Holter monitoring showing no ischemic episodes has an excellent negative predictive value for postoperative cardiac complications."
Limitations
- Only 24-48 hours of recording - misses infrequent arrhythmias
- The ability to diagnose depends on a symptom occurring during the recording window
- Artifact can simulate dangerous arrhythmias (VT, VF, asystole)
2. Loop Recorders
Loop recorders extend monitoring well beyond the Holter's 48-hour window. There are two types: external and implantable.
2a. External Loop Recorders (Event Recorders)
These devices continuously record and store the ECG in a "loop" buffer - typically the last few minutes of activity. When the patient activates the device (or when pre-programmed rate thresholds are met), the preceding and following ECG is saved to memory for later analysis.
- Worn externally for days to weeks
- Can transmit data wirelessly to a cardiac monitoring centre (mobile cardiac outpatient telemetry - MCOT)
- Best when symptoms are intermittent but occur at least once every few weeks
- Limitation: Patient must be conscious to trigger the device - not ideal for syncope
Harrison's Principles (22e) notes: "A patient-activated event recorder is inappropriate in a patient with syncope, as the arrhythmic event will likely have passed once the patient reawakens."
2b. Implantable Loop Recorder (ILR)
The ILR is the most powerful tool for detecting infrequent, unexplained arrhythmias.

(ILR placement: the tiny device - about 1¾ inches long - is inserted subcutaneously in the left parasternal or left anterior axillary position)
How it works (from Goldman-Cecil Medicine):
"Implantable loop recorders are small devices with integrated leads that are placed in a small subcutaneous pocket during a simple surgery, usually performed in the electrophysiology laboratory. They function similarly to event recorders in terms of recording ECGs. Patients can activate the device with a small transmitter, or the device can be autotriggered on the basis of preprogrammed heart rates. Newer devices can wirelessly communicate with a telephone-connected base station in the home to upload data after an event."
| Feature | Details |
|---|---|
| Size | ~1¾ inches (~4.5 cm) - about the size of a USB stick |
| Insertion | Minimally invasive, local anaesthesia, no general surgery |
| Battery life | Up to 3 years of continuous monitoring |
| Triggering | Auto-triggered by pre-set rate limits OR patient-activated handheld transmitter |
| Remote monitoring | Wireless upload to home base station - transmits to cardiologist |
| Interrogation | Like a pacemaker - external programmer reads stored data |
Indications for ILR
- Unexplained syncope - ILR outperforms the combination of tilt testing, external loop recorders, and electrophysiologic testing for establishing an arrhythmic cause
- Cryptogenic stroke - to detect paroxysmal atrial fibrillation (ILR detects AF significantly more often than prolonged external monitoring in patients aged 70-79 or with prior ischemic stroke)
- Palpitations - when symptoms are too infrequent for shorter-term monitors
- Suspected paroxysmal AV block
3. Ambulatory Blood Pressure Recording (ABPM)
Principle
ABPM uses an oscillometric cuff (upper arm) that automatically inflates at programmed intervals throughout a 24-hour period (typically every 15-20 minutes during the day and every 30 minutes at night), giving a complete picture of blood pressure behaviour across the full sleep-wake cycle.

(Classic 24-hour ABPM: upper arm oscillometric cuff connected to portable recorder worn on a shoulder strap)

(Modern compact wearable ABPM device - records day and night blood pressure seamlessly)
Why ABPM is Superior to Office BP
From Brenner and Rector's The Kidney and Comprehensive Clinical Nephrology:
ABPM:
- Diagnoses white coat hypertension (elevated clinic BP, normal ambulatory BP)
- Diagnoses masked hypertension (normal clinic BP, elevated ambulatory BP - missed by office readings alone)
- Identifies nocturnal hypertension - the absence of the normal nocturnal dip ("non-dipping") is an independent risk factor for cardiovascular events
- Correlates better with target-organ damage (LVH, renal damage, retinopathy) and future CV events than either office or home BP
- Identifies true resistant hypertension (vs. white coat resistance)
Indications for ABPM
| Clinical Situation | ABPM Priority |
|---|---|
| White coat hypertension suspected | +++ (gold standard) |
| Masked hypertension | +++ |
| True resistant hypertension | +++ |
| Nocturnal hypertension / non-dipping | +++ (home monitoring cannot do this) |
| Borderline office BP, no organ damage | +++ |
| Labile / episodic hypertension | ++ |
| Autonomic dysfunction | ++ |
| Hypotensive symptoms | ++ |
| Carotid sinus syncope / pacemaker syndrome | ++ |
| Evaluating 24-hour drug effect | +++ |
Diagnosis Algorithm
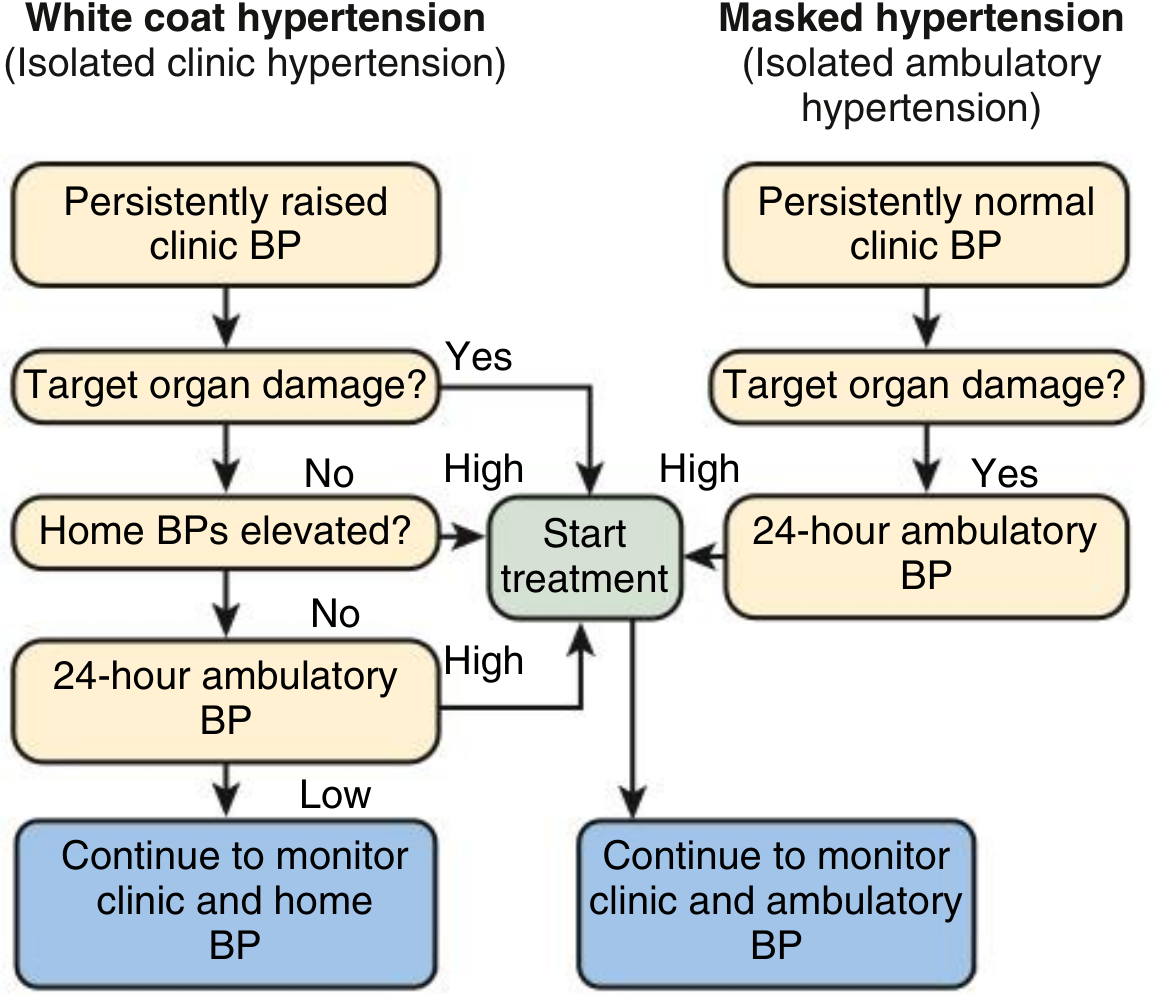
(Algorithm for using clinic, home, and ambulatory BP to diagnose white coat and masked hypertension - from Comprehensive Clinical Nephrology)
Normal ABPM Thresholds (as per guidelines)
| Period | Normal BP Target |
|---|---|
| 24-hour average | < 130/80 mmHg |
| Daytime (awake) | < 135/85 mmHg |
| Night-time (asleep) | < 120/70 mmHg |
| Normal nocturnal dip | 10-20% fall from daytime values |
Practical Points
- Patient keeps an activity diary noting wake/sleep times and medication timing
- Most patients tolerate the procedure well; <10% have compromised sleep
- Occasional bruising or discomfort from frequent cuff inflations
- Use an independently validated monitor (see dableducational.org)
- Clinicians should use actual diary-derived sleep/wake times rather than fixed windows
4. Newer Technologies for Cardiac Monitoring
The monitoring landscape has expanded dramatically with digital health, miniaturisation, and AI.

(Left to right: smartwatch with ECG/PPG, adhesive patch monitor, implantable loop recorder)
4a. ECG Patch Monitors
- Adhesive patch worn continuously for 7-14 days
- Single or multi-lead continuous ECG recording
- No wires or bulky recorder - shower-safe
- Examples: Zio Patch (iRhythm), BioTel Heart patches
- AI-powered analysis significantly reduces physician review time
- Best for detecting paroxysmal AF, PACs, PVCs, conduction disorders
4b. Mobile Cardiac Outpatient Telemetry (MCOT)
From Goldman-Cecil Medicine:
"Mobile cardiac outpatient telemetry units are similar to external event monitors, except that data are transmitted wirelessly in real time to a monitoring center. These devices are useful for patients in whom intermittent symptoms are severe or the differential diagnosis includes potentially dangerous arrhythmias that should be diagnosed expeditiously."
- Real-time wireless transmission to a staffed monitoring centre 24/7
- The centre can alert emergency services if dangerous rhythms are detected
- Duration: typically 30 days
4c. Consumer-Based Wearable Rhythm Monitors
Smartwatches with ECG capability (Apple Watch, Samsung Galaxy Watch, Withings ScanWatch):
- Use photoplethysmography (PPG) via optical sensors on the wrist to detect pulse rate and rhythm
- Single-lead ECG recorded by touching the crown (Apple Watch) or bezel
- FDA/CE approved for atrial fibrillation screening only
- Automated classification: "Normal", "Possible AFib", or "Undetermined"
Goldman-Cecil Medicine cautions:
"These devices should not generally substitute for other, more established types of ambulatory monitoring to diagnose patients with suspected arrhythmias, with the possible exception of screening for atrial fibrillation."
4d. AI-Enabled Analysis
Modern ambulatory ECG platforms now incorporate machine learning algorithms to:
- Auto-detect and classify AF, SVT, VT, heart blocks
- Flag clinically significant findings for urgent physician review
- Reduce false positive rates that previously burdened Holter interpretation
4e. Cuffless Blood Pressure Monitoring
An emerging frontier for ABPM: cuffless wrist-worn sensors using PPG + pulse transit time estimate BP without an inflating cuff. Currently under validation - not yet a replacement for standard oscillometric ABPM, but Nature Scientific Reports research shows feasibility for 24-hour BP profiling.
4f. Remote Monitoring & Telehealth Integration
- ILRs and cardiac implantable devices now transmit data nightly to cloud servers
- Cardiologists receive automated alerts for predefined events (AF episode >30 minutes, bradycardia <40 bpm, etc.)
- Reduces the need for frequent in-person device checks
Summary Comparison Table
| Technology | Duration | Invasive? | Triggers | Best For |
|---|---|---|---|---|
| Holter Monitor | 24-48 h | No | Continuous | Frequent symptoms (daily) |
| Extended Holter | Up to 2 weeks | No | Continuous | Frequent-intermittent symptoms |
| External Loop Recorder | Weeks | No | Patient + auto | Infrequent symptoms (conscious) |
| ECG Patch (Zio etc.) | 7-14 days | No | Continuous | Paroxysmal AF, PVC burden |
| MCOT | Up to 30 days | No | Auto + real-time | Urgent/dangerous suspected arrhythmia |
| Implantable Loop Recorder | Up to 3 years | Minimally (subcutaneous) | Auto + patient | Syncope, cryptogenic stroke, rare events |
| ABPM | 24-48 h | No | Automated cuff | Hypertension evaluation |
| Smartwatch ECG | Continuous | No | Patient-activated | AF screening only |
Sources consulted:
- Braunwald's Heart Disease, 12e, Ambulatory Electrocardiographic (Holter) Recording
- Goldman-Cecil Medicine, Implantable Loop Recorders & Consumer-Based Rhythm Monitors
- Harrison's Principles of Internal Medicine, 22e, Arrhythmia Evaluation
- Brenner and Rector's The Kidney, Clinical Use of Ambulatory and Home BP Monitoring
- Comprehensive Clinical Nephrology, 7e, Ambulatory Blood Pressure Monitoring
- Morgan & Mikhail's Clinical Anesthesiology, 7e, Holter Monitoring
- AER Journal - Holter and Loop Recorders review
This is a shared conversation. Sign in to Orris to start your own chat.