Hand functions
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Here is a comprehensive overview of hand functions — the muscles, tendons, nerves, and movements that enable the hand's remarkable capabilities.
Hand Functions
Overview
The hand performs two broad categories of function:
- Prehensile (grasping) — power grip, precision pinch, lateral pinch, opposition
- Non-prehensile — pushing, tapping, pressing
These are executed through a coordinated interplay of extrinsic muscles (originating in the forearm) and intrinsic muscles (wholly within the hand).
1. Intrinsic Muscles of the Hand
Intrinsic muscles have both their origin and insertion within the hand. They are organized into three groups:
A. Thenar Muscles (thumb eminence)
All act on the thumb at the carpometacarpal (CMC) and metacarpophalangeal (MCP) joints.
| Muscle | Action | Nerve |
|---|---|---|
| Abductor pollicis brevis | Thumb abduction | Median (C8, T1) |
| Opponens pollicis | Thumb opposition (CMC) | Median (C8, T1) |
| Flexor pollicis brevis (superficial head) | Thumb flexion (MCP) | Median (C8, T1) |
| Flexor pollicis brevis (deep head) | Thumb flexion | Ulnar (C8, T1) |
| Adductor pollicis | Thumb adduction, MCP flexion | Ulnar (C8, T1) |
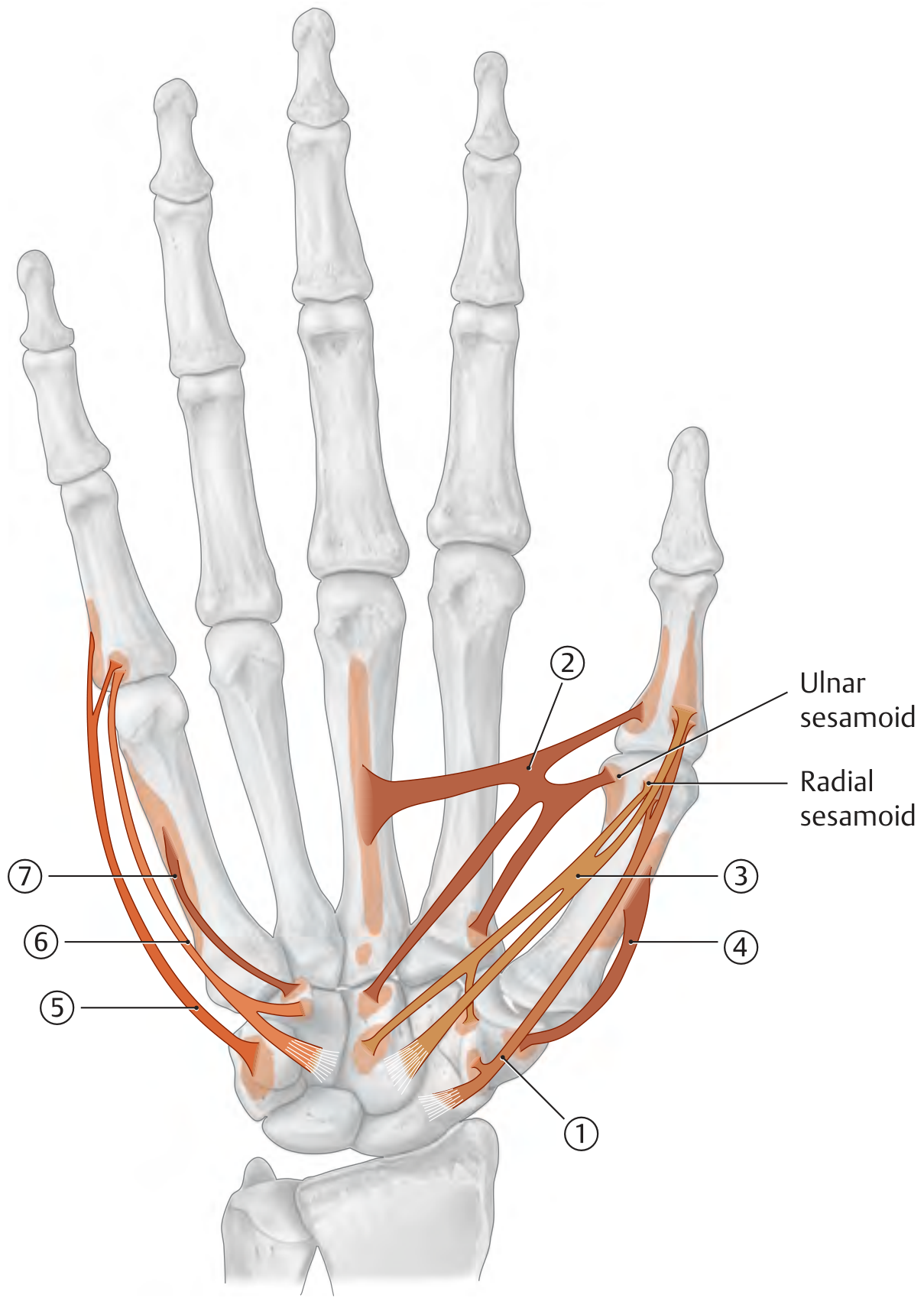
The ability to grasp an object between the pad of the thumb and a finger depends entirely on the thenar muscles (recurrent branch of the median nerve, C8–T1). — Gray's Anatomy for Students
B. Hypothenar Muscles (little-finger eminence)
All innervated by the ulnar nerve (C8, T1).
| Muscle | Action |
|---|---|
| Abductor digiti minimi | Abduction + MCP flexion of little finger; PIP/DIP extension |
| Flexor digiti minimi brevis | MCP flexion of little finger |
| Opponens digiti minimi | Opposition of little finger |
C. Metacarpal Muscles (Lumbricals and Interossei)
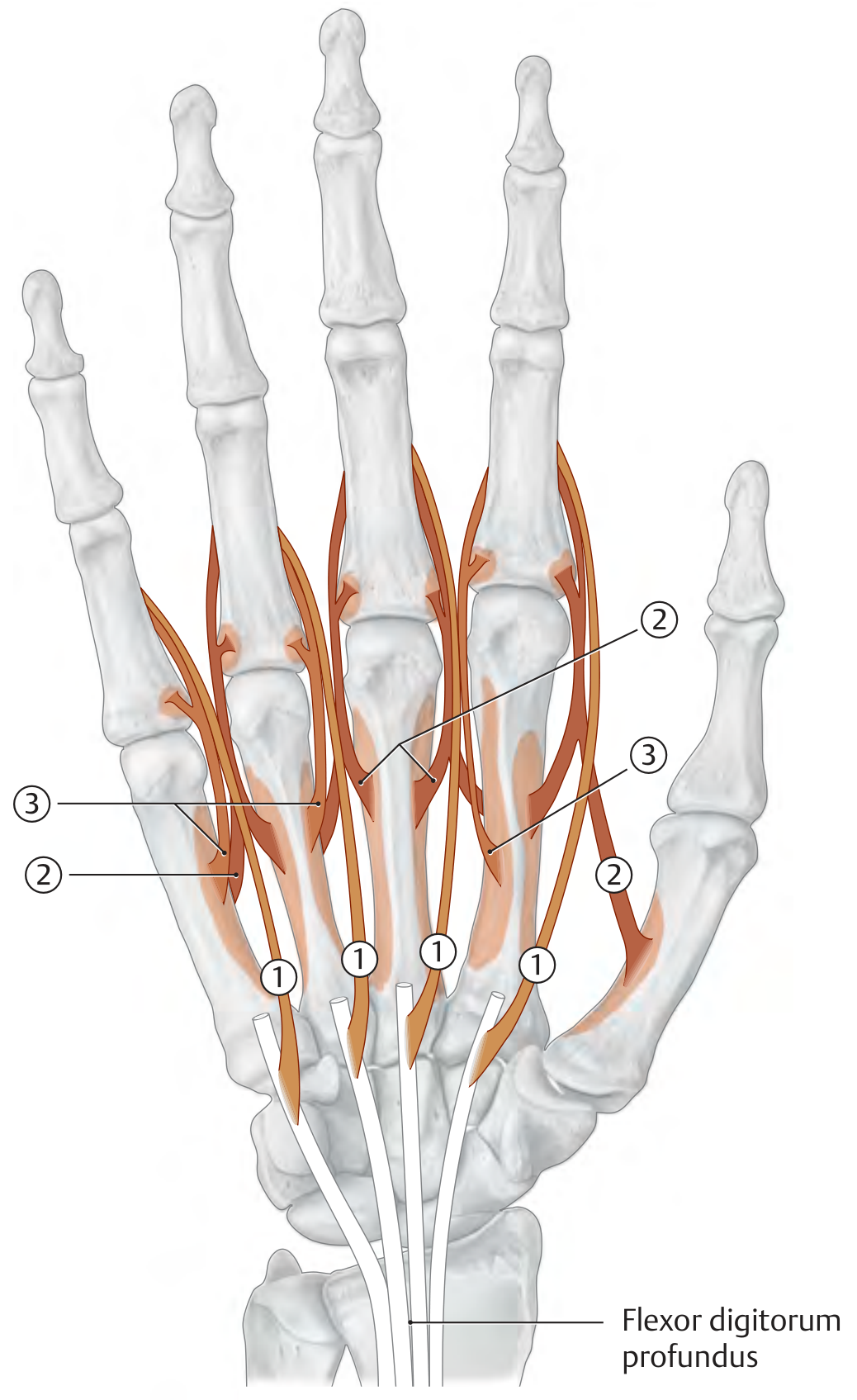
Lumbricals (×4)
- Origin: radial sides of the flexor digitorum profundus (FDP) tendons
- Insertion: dorsal digital expansion (extensor hood) of digits 2–5
- Action: Flex MCP joints + extend PIP and DIP joints simultaneously — the key "intrinsic-plus" position
- Innervation: 1st & 2nd → Median nerve; 3rd & 4th → Ulnar nerve (both C8, T1)
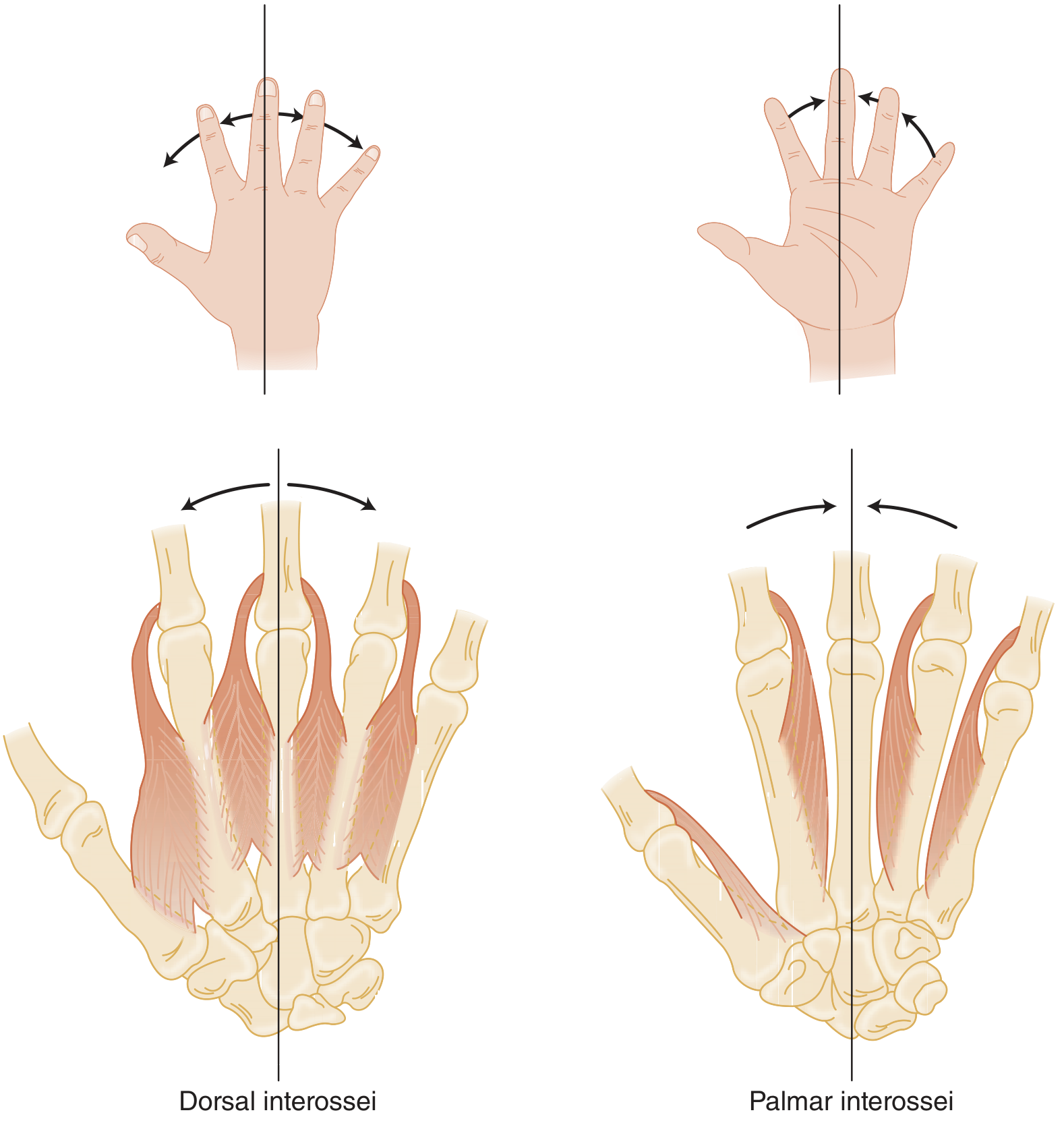
Dorsal Interossei (×4)
- Origin: adjacent sides of metacarpals 1–5 (bipennate)
- Action: MCP flexion + abduction of fingers away from the middle finger axis; PIP/DIP extension
- Innervation: Ulnar nerve (C8, T1)
Palmar Interossei (×3)
- Origin: ulnar side of MC2; radial sides of MC4 and MC5
- Action: MCP flexion + adduction of fingers toward the middle finger; PIP/DIP extension
- Innervation: Ulnar nerve (C8, T1)
Flexing the MCP joints while simultaneously extending the PIP and DIP joints is entirely dependent on the intrinsic muscles, mainly innervated by the deep branch of the ulnar nerve (C8–T1). — Gray's Anatomy for Students
2. Extrinsic Tendons
Flexor Tendons
Nine tendons pass through the carpal tunnel:
- Flexor digitorum superficialis (FDS) ×4 — inserts on the volar proximal middle phalanx → flexes PIP and MCP joints
- Flexor digitorum profundus (FDP) ×4 — inserts at the volar base of the distal phalanx → primarily flexes DIP joint, also PIP and MCP
- Flexor pollicis longus (FPL) ×1 — inserts at the base of the thumb distal phalanx → flexes thumb IP joint
The FDS and FDP run together in synovial sheaths within fibro-osseous tunnels (flexor pulleys), making them susceptible to infectious tenosynovitis.
Extensor Tendons
Nine extensor tendons course under the extensor retinaculum through 6 compartments. In the finger, the extensor mechanism divides into:
- Central slip → attaches to the middle phalanx → extends PIP
- Two lateral bands (joined by lumbrical and interosseous contributions) → attach to the dorsal base of the distal phalanx as the terminal tendon → extend DIP
Adjacent extensor digitorum communis (EDC) tendons are connected by juncturae tendinum — so a complete EDC laceration proximal to a juncture may still allow some finger extension via the neighboring tendon.
3. Functional Movements of the Hand
| Movement | Primary Muscles | Nerve |
|---|---|---|
| Finger flexion (DIP) | FDP | Anterior interosseous (median) to digits 2–3; ulnar to digits 4–5 |
| Finger flexion (PIP) | FDS | Median nerve |
| Finger flexion (MCP) | Interossei, lumbricals | Ulnar (± median for 1st/2nd lumbricals) |
| Finger extension | EDC + EIP + EDM | Radial/posterior interosseous nerve |
| Finger abduction | Dorsal interossei + abductor digiti minimi | Ulnar nerve |
| Finger adduction | Palmar interossei | Ulnar nerve |
| Thumb opposition | Opponens pollicis, abductor pollicis brevis, FPB | Median nerve (recurrent branch) |
| Thumb adduction | Adductor pollicis | Ulnar nerve |
| Thumb IP flexion | FPL | Anterior interosseous nerve (median) |
4. Nerve Contributions — Summary
| Nerve | Key Hand Functions |
|---|---|
| Median | Thenar opposition/abduction; 1st & 2nd lumbrical; FDS & FDP (digits 2–3); FPL |
| Ulnar | All interossei; 3rd & 4th lumbricals; hypothenar muscles; adductor pollicis; FDP (digits 4–5) |
| Radial (PIN) | All finger and wrist extensors; no intrinsic function |
5. Clinical Correlates
- Ulnar nerve palsy → loss of interossei and most intrinsics → "claw hand" (MCP hyperextension, PIP/DIP flexion) most pronounced in ring and little fingers; loss of finger abduction/adduction
- Median nerve palsy → loss of thenar muscles → "ape hand" (inability to oppose thumb); loss of FDS, FDP digits 2–3
- Radial nerve palsy → wrist drop; no intrinsic motor loss
- Boutonnière deformity — central slip rupture → PIP flexion + DIP hyperextension
- Mallet finger — terminal tendon avulsion → isolated DIP flexion deformity
Sources: Gray's Anatomy for Students; THIEME Atlas of General Anatomy and Musculoskeletal System; Tintinalli's Emergency Medicine
refer Pedretti book of occupational therapy for same topic and give me ppt
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Running Command
ls /home/daytona/workspace/ 2>/dev/null || mkdir -p /home/daytona/workspace/hand-functions-ppt
Running Command
mkdir -p /home/daytona/workspace/hand-functions-ppt && ls /home/daytona/workspace/hand-functions-ppt
Writing File
~/hand-functions-ppt/build.js
const pptxgen = require("pptxgenjs");
const pres = new pptxgen();
pres.layout = "LAYOUT_16x9";
pres.title = "Hand Functions – Occupational Therapy Perspective";
pres.author = "Pedretti's Occupational Therapy";
// ─── COLOR PALETTE ───────────────────────────────────────────────
const C = {
navy: "1A3A5C", // dominant dark bg
teal: "1B7FA3", // accent headers
amber: "E8A020", // highlight / accent
white: "FFFFFF",
offWhite:"F0F4F8",
lightBlue:"D6EAF5",
darkText: "1A2B3C",
midText: "2C4A6E",
grey: "6B7C93",
};
// ─── HELPER FUNCTIONS ────────────────────────────────────────────
function titleSlide(pres, title, subtitle) {
const s = pres.addSlide();
// Full navy background
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.navy }, line: { color: C.navy } });
// Teal accent bar left
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 0.4, h: 5.625, fill: { color: C.teal }, line: { color: C.teal } });
// Amber bottom stripe
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 5.1, w: 10, h: 0.525, fill: { color: C.amber }, line: { color: C.amber } });
s.addText(title, {
x: 0.7, y: 1.4, w: 8.6, h: 1.4,
fontSize: 38, bold: true, color: C.white, align: "left",
fontFace: "Calibri", wrap: true
});
s.addText(subtitle, {
x: 0.7, y: 2.95, w: 8.6, h: 0.8,
fontSize: 22, color: C.lightBlue, align: "left",
fontFace: "Calibri"
});
s.addText("Based on Pedretti's Occupational Therapy – Practice Skills for Physical Dysfunction", {
x: 0.7, y: 3.8, w: 8.6, h: 0.5,
fontSize: 13, color: C.grey, align: "left", italic: true, fontFace: "Calibri"
});
return s;
}
function sectionHeader(pres, sectionNum, title, subtitle) {
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.navy }, line: { color: C.navy } });
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 0.08, fill: { color: C.amber }, line: { color: C.amber } });
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 5.545, w: 10, h: 0.08, fill: { color: C.teal }, line: { color: C.teal } });
s.addText(`0${sectionNum}`, {
x: 0.5, y: 1.0, w: 2, h: 1.8,
fontSize: 90, bold: true, color: C.amber, fontFace: "Calibri", opacity: 0.25
});
s.addText(title, {
x: 0.6, y: 1.8, w: 8.8, h: 1.1,
fontSize: 32, bold: true, color: C.white, fontFace: "Calibri"
});
s.addText(subtitle, {
x: 0.6, y: 3.0, w: 8.8, h: 0.7,
fontSize: 18, color: C.lightBlue, fontFace: "Calibri"
});
return s;
}
function contentSlide(pres, title, bullets, opts = {}) {
const s = pres.addSlide();
// Light background
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.offWhite }, line: { color: C.offWhite } });
// Top header bar
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 0.9, fill: { color: C.navy }, line: { color: C.navy } });
// Amber accent left of title
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 0.18, h: 0.9, fill: { color: C.amber }, line: { color: C.amber } });
s.addText(title, {
x: 0.35, y: 0.0, w: 9.4, h: 0.9,
fontSize: 20, bold: true, color: C.white, valign: "middle",
fontFace: "Calibri", margin: 0
});
const startY = opts.startY || 1.05;
const contentW = opts.contentW || 9.2;
const contentH = opts.contentH || 4.2;
const bulletItems = bullets.map((b, i) => {
const isSubBullet = b.startsWith(" ");
const text = b.replace(/^ /, "");
const isLast = i === bullets.length - 1;
return {
text: text,
options: {
bullet: isSubBullet ? { indent: 25 } : { indent: 10 },
fontSize: isSubBullet ? 14 : 16,
color: isSubBullet ? C.midText : C.darkText,
bold: false,
breakLine: !isLast
}
};
});
s.addText(bulletItems, {
x: 0.4, y: startY, w: contentW, h: contentH,
fontFace: "Calibri", valign: "top", paraSpaceBefore: 4, paraSpaceAfter: 2
});
// Footer
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 5.45, w: 10, h: 0.175, fill: { color: C.teal }, line: { color: C.teal } });
s.addText("Pedretti's Occupational Therapy – Hand Functions", {
x: 0.3, y: 5.45, w: 9.4, h: 0.175,
fontSize: 9, color: C.white, valign: "middle", fontFace: "Calibri"
});
return s;
}
function twoColSlide(pres, title, leftTitle, leftBullets, rightTitle, rightBullets) {
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.offWhite }, line: { color: C.offWhite } });
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 0.9, fill: { color: C.navy }, line: { color: C.navy } });
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 0.18, h: 0.9, fill: { color: C.amber }, line: { color: C.amber } });
s.addText(title, {
x: 0.35, y: 0, w: 9.4, h: 0.9, fontSize: 20, bold: true, color: C.white,
valign: "middle", fontFace: "Calibri", margin: 0
});
// Left column
s.addShape(pres.shapes.RECTANGLE, { x: 0.3, y: 1.0, w: 4.4, h: 4.3, fill: { color: C.white }, line: { color: C.lightBlue, pt: 1 }, shadow: { type: "outer", color: "000000", blur: 4, offset: 2, angle: 135, opacity: 0.08 } });
s.addText(leftTitle, { x: 0.4, y: 1.05, w: 4.2, h: 0.45, fontSize: 15, bold: true, color: C.teal, fontFace: "Calibri" });
const leftItems = leftBullets.map((b, i) => ({ text: b, options: { bullet: { indent: 10 }, fontSize: 14, color: C.darkText, breakLine: i !== leftBullets.length - 1 } }));
s.addText(leftItems, { x: 0.4, y: 1.55, w: 4.2, h: 3.6, fontFace: "Calibri", valign: "top", paraSpaceBefore: 3 });
// Right column
s.addShape(pres.shapes.RECTANGLE, { x: 5.3, y: 1.0, w: 4.4, h: 4.3, fill: { color: C.white }, line: { color: C.lightBlue, pt: 1 }, shadow: { type: "outer", color: "000000", blur: 4, offset: 2, angle: 135, opacity: 0.08 } });
s.addText(rightTitle, { x: 5.4, y: 1.05, w: 4.2, h: 0.45, fontSize: 15, bold: true, color: C.amber, fontFace: "Calibri" });
const rightItems = rightBullets.map((b, i) => ({ text: b, options: { bullet: { indent: 10 }, fontSize: 14, color: C.darkText, breakLine: i !== rightBullets.length - 1 } }));
s.addText(rightItems, { x: 5.4, y: 1.55, w: 4.2, h: 3.6, fontFace: "Calibri", valign: "top", paraSpaceBefore: 3 });
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 5.45, w: 10, h: 0.175, fill: { color: C.teal }, line: { color: C.teal } });
s.addText("Pedretti's Occupational Therapy – Hand Functions", { x: 0.3, y: 5.45, w: 9.4, h: 0.175, fontSize: 9, color: C.white, valign: "middle", fontFace: "Calibri" });
return s;
}
function tableSlide(pres, title, headers, rows) {
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.offWhite }, line: { color: C.offWhite } });
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 0.9, fill: { color: C.navy }, line: { color: C.navy } });
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 0.18, h: 0.9, fill: { color: C.amber }, line: { color: C.amber } });
s.addText(title, { x: 0.35, y: 0, w: 9.4, h: 0.9, fontSize: 20, bold: true, color: C.white, valign: "middle", fontFace: "Calibri", margin: 0 });
const colW = 9.4 / headers.length;
const tableRows = [
headers.map(h => ({
text: h,
options: { bold: true, color: C.white, fill: { color: C.teal }, fontSize: 13, align: "center", fontFace: "Calibri" }
})),
...rows.map((row, ri) =>
row.map(cell => ({
text: cell,
options: { color: C.darkText, fill: { color: ri % 2 === 0 ? C.white : C.lightBlue }, fontSize: 12, fontFace: "Calibri" }
}))
)
];
s.addTable(tableRows, {
x: 0.3, y: 1.0, w: 9.4, colW: headers.map(() => colW),
border: { pt: 0.5, color: "CBD5E0" },
rowH: 0.42
});
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 5.45, w: 10, h: 0.175, fill: { color: C.teal }, line: { color: C.teal } });
s.addText("Pedretti's Occupational Therapy – Hand Functions", { x: 0.3, y: 5.45, w: 9.4, h: 0.175, fontSize: 9, color: C.white, valign: "middle", fontFace: "Calibri" });
return s;
}
// ─── SLIDE 1: TITLE ──────────────────────────────────────────────
titleSlide(pres, "Hand Functions", "Anatomy, Kinesiology & Occupational Performance");
// ─── SLIDE 2: OUTLINE ────────────────────────────────────────────
contentSlide(pres, "Outline", [
"01 Overview of Hand Function",
"02 Bones & Joints of the Hand",
"03 Extrinsic Muscles – Flexors",
"04 Extrinsic Muscles – Extensors",
"05 Intrinsic Muscles – Thenar & Hypothenar",
"06 Intrinsic Muscles – Lumbricals & Interossei",
"07 Nerve Supply of the Hand",
"08 Functional Movements & Prehension Patterns",
"09 Grip & Pinch Types (Pedretti's Classification)",
"10 Clinical Correlates & OT Assessment",
]);
// ─── SLIDE 3: SECTION 1 ──────────────────────────────────────────
sectionHeader(pres, 1, "Overview of Hand Function", "The hand as a tool of occupational performance");
// ─── SLIDE 4: OVERVIEW ───────────────────────────────────────────
contentSlide(pres, "Overview of Hand Function", [
"The hand is the primary end-organ for manipulation and occupational performance",
"Two categories of hand use:",
" Prehensile – grasping, holding, pinching (power or precision)",
" Non-prehensile – pushing, pressing, tapping",
"Hand function depends on:",
" Intact musculoskeletal framework (bones, joints, tendons)",
" Normal neuromuscular control (peripheral nerve integrity)",
" Sensory feedback (touch, proprioception, pain, temperature)",
" Coordinated interplay of extrinsic and intrinsic muscles",
"OT perspective (Pedretti): hand function assessed within context of ADL, productivity, and leisure",
]);
// ─── SLIDE 5: BONES & JOINTS ─────────────────────────────────────
sectionHeader(pres, 2, "Bones & Joints of the Hand", "Structural framework enabling mobility and stability");
contentSlide(pres, "Bones & Joints of the Hand", [
"27 bones in the hand and wrist:",
" 8 carpal bones (proximal & distal rows)",
" 5 metacarpal bones (MC1–MC5)",
" 14 phalanges: 3 per finger (proximal, middle, distal), 2 for thumb",
"Key joints:",
" Radiocarpal (wrist) joint – flexion, extension, radial/ulnar deviation",
" Carpometacarpal (CMC) joints – saddle joint of thumb allows opposition",
" Metacarpophalangeal (MCP) joints – flexion, extension, abduction, adduction",
" Proximal interphalangeal (PIP) joints – hinge, flexion/extension only",
" Distal interphalangeal (DIP) joints – hinge, flexion/extension only",
]);
// ─── SLIDE 6: EXTRINSIC FLEXORS ──────────────────────────────────
sectionHeader(pres, 3, "Extrinsic Muscles – Flexors", "Origin in forearm, insertion in hand");
contentSlide(pres, "Extrinsic Flexor Tendons", [
"9 flexor tendons pass through the carpal tunnel:",
"Flexor Digitorum Superficialis (FDS) ×4:",
" Inserts: volar surface of middle phalanx (digits 2–5)",
" Action: Flexes PIP and MCP joints",
" Nerve: Median nerve (C7, C8, T1)",
"Flexor Digitorum Profundus (FDP) ×4:",
" Inserts: volar base of distal phalanx (digits 2–5)",
" Action: Primarily flexes DIP; also PIP and MCP",
" Nerve: Median (digits 2–3) / Ulnar (digits 4–5)",
"Flexor Pollicis Longus (FPL) ×1:",
" Inserts: distal phalanx of thumb",
" Action: Flexes thumb IP joint",
" Nerve: Anterior interosseous branch of median nerve",
]);
// ─── SLIDE 7: EXTRINSIC EXTENSORS ────────────────────────────────
sectionHeader(pres, 4, "Extrinsic Muscles – Extensors", "Nine extensors in 6 compartments under extensor retinaculum");
contentSlide(pres, "Extrinsic Extensor Tendons", [
"9 extensor tendons divide under extensor retinaculum into 6 compartments",
"Extensor Digitorum Communis (EDC): extends fingers at MCP, PIP, DIP",
" Adjacent tendons connected by juncturae tendinum",
" Laceration proximal to juncture may still allow extension via neighbor",
"Extensor mechanism in the finger divides into:",
" Central slip → inserts on middle phalanx → extends PIP joint",
" Two lateral bands → join lumbrical/interosseous tendons",
" Terminal tendon (lateral bands) → inserts on distal phalanx → extends DIP",
"Other extensors: EIP (index), EDM (little finger), EPL/EPB/APL (thumb)",
"Nerve supply: Radial nerve / Posterior interosseous nerve (PIN)",
]);
// ─── SLIDE 8: THENAR & HYPOTHENAR ────────────────────────────────
sectionHeader(pres, 5, "Intrinsic Muscles – Thenar & Hypothenar", "Both origin and insertion within the hand");
twoColSlide(pres,
"Thenar Muscles (Median Nerve C8, T1)",
"Thenar Muscles",
[
"Abductor pollicis brevis",
" → Thumb abduction",
" → Median nerve (C8, T1)",
"Opponens pollicis",
" → CMC opposition (thumb)",
" → Median nerve (C8, T1)",
"Flexor pollicis brevis",
" → Superficial head: Median nerve",
" → Deep head: Ulnar nerve",
"Adductor pollicis",
" → Thumb adduction & MCP flexion",
" → Ulnar nerve (C8, T1)",
],
"Hypothenar Muscles (Ulnar Nerve C8, T1)",
[
"Abductor digiti minimi",
" → Little finger abduction",
" → MCP flexion; PIP/DIP extension",
"Flexor digiti minimi brevis",
" → Little finger MCP flexion",
"Opponens digiti minimi",
" → Little finger opposition",
"All three innervated by Ulnar nerve",
"Origin: flexor retinaculum & carpal bones",
"Lesion → loss of little finger opposition",
]
);
// ─── SLIDE 9: LUMBRICALS & INTEROSSEI ────────────────────────────
sectionHeader(pres, 6, "Intrinsic Muscles – Lumbricals & Interossei", "The key to combined MCP flexion + IP extension");
twoColSlide(pres,
"Lumbricals & Interossei",
"Lumbrical Muscles (×4)",
[
"Origin: FDP tendons (radial side)",
"Insertion: Dorsal digital expansion",
"Action (intrinsic-plus position):",
" → Flex MCP joints (digits 2–5)",
" → Extend PIP and DIP joints",
"Innervation:",
" 1st & 2nd → Median nerve (C8, T1)",
" 3rd & 4th → Ulnar nerve (C8, T1)",
"OT significance: essential for writing, pinch",
],
"Interossei Muscles",
[
"Dorsal interossei (×4) – Ulnar nerve C8/T1",
" → Abduct fingers from midline (DAB)",
" → Also flex MCP + extend PIP/DIP",
"Palmar interossei (×3) – Ulnar nerve C8/T1",
" → Adduct fingers to midline (PAD)",
" → Also flex MCP + extend PIP/DIP",
"Midline reference = middle (3rd) finger",
"OT significance: precision grip, typing, ADLs",
]
);
// ─── SLIDE 10: NERVE SUPPLY ───────────────────────────────────────
sectionHeader(pres, 7, "Nerve Supply of the Hand", "Median, Ulnar, and Radial nerve territories");
tableSlide(pres, "Nerve Supply – Motor Functions",
["Nerve", "Key Structures Innervated", "Functional Deficit if Lost"],
[
["Median nerve\n(C6–T1)", "Thenar muscles (APB, OP, FPB-superficial)\n1st & 2nd lumbricals\nFDS, FDP (digits 2–3), FPL", "Loss of thumb opposition\n'Ape hand' deformity\nWeak precision pinch"],
["Ulnar nerve\n(C8–T1)", "All interossei (dorsal & palmar)\n3rd & 4th lumbricals, hypothenar\nFDP (digits 4–5), adductor pollicis", "Claw hand (ring & little)\nLoss of finger abduction/adduction\nWeak power grip"],
["Radial nerve\n(C5–C8)", "All wrist & finger extensors\nNo intrinsic hand muscles", "Wrist drop\nInability to extend fingers\nNo intrinsic hand loss"],
]
);
// ─── SLIDE 11: FUNCTIONAL MOVEMENTS ──────────────────────────────
sectionHeader(pres, 8, "Functional Movements & Prehension", "Movement analysis for occupational performance");
contentSlide(pres, "Functional Movements of the Hand", [
"Wrist positioning provides the stable base for all hand function:",
" Wrist extension (30°–35°) = optimal tenodesis position",
" Wrist flexion weakens grip force significantly",
"Key finger movements:",
" DIP flexion – FDP (AIN/median or ulnar nerve)",
" PIP flexion – FDS (median nerve)",
" MCP flexion + IP extension – Intrinsic muscles (combined)",
" Finger abduction – Dorsal interossei (ulnar nerve)",
" Finger adduction – Palmar interossei (ulnar nerve)",
"Thumb movements:",
" Palmar abduction, opposition, adduction – critical for pinch",
" Composite opposition (O-ring test) requires median + ulnar nerve integrity",
]);
// ─── SLIDE 12: GRIP & PINCH ───────────────────────────────────────
sectionHeader(pres, 9, "Grip & Pinch Patterns", "Pedretti's classification of prehension patterns");
contentSlide(pres, "Prehension Patterns (Pedretti's Classification)", [
"POWER GRIPS (large force; whole hand; extrinsic + intrinsic):",
" Cylindrical grip – holding a hammer, jar, glass",
" Spherical grip – holding a ball, orange",
" Hook grip – carrying a briefcase (FDP dominant)",
" Lateral (key) pinch – may be classified under power",
"PRECISION GRIPS (fine control; fingertips; intrinsic-dominant):",
" Tip-to-tip pinch (pulp pinch) – threading a needle",
" Lateral (key) pinch – turning a key, holding card",
" Three-jaw chuck (tripod pinch) – holding a pen",
"Tenodesis grip: passive functional grip for C6 spinal cord injury",
" Wrist extension → passive finger flexion (natural tenodesis)",
" Wrist flexion → fingers open",
]);
// ─── SLIDE 13: OT ASSESSMENT ─────────────────────────────────────
sectionHeader(pres, 10, "Clinical Correlates & OT Assessment", "Nerve injuries, deformities, and functional evaluation");
twoColSlide(pres,
"Hand Dysfunction – OT Assessment & Intervention",
"Common Clinical Deformities",
[
"Claw hand (ulnar nerve palsy)",
" → MCP hyperextension, PIP/DIP flexion",
" → Ring & little fingers worst affected",
"Ape hand (median nerve palsy)",
" → Thenar wasting, no opposition",
"Wrist drop (radial nerve palsy)",
" → Loss of wrist & finger extension",
"Boutonnière deformity",
" → Central slip rupture → PIP flexion + DIP extension",
"Mallet finger",
" → Terminal tendon avulsion → DIP drop",
"Swan-neck deformity",
" → PIP hyperextension + DIP flexion",
],
"OT Evaluation & Approach",
[
"Range of motion (goniometry) – MCP, PIP, DIP",
"Grip strength – Jamar dynamometer (5 positions)",
"Pinch strength – Pinch gauge (tip, lateral, tripod)",
"Sensory testing – Semmes-Weinstein monofilaments, 2PD",
"Functional assessments:",
" → DASH, COPM, Jebsen-Taylor Hand Function Test",
" → Box & Block Test, Purdue Pegboard",
"OT intervention strategies:",
" → Splinting for deformity prevention/correction",
" → Tendon gliding exercises (FDS/FDP differentiation)",
" → ADL retraining, adaptive equipment",
" → Sensory re-education, desensitization",
]
);
// ─── SLIDE 14: SUMMARY ───────────────────────────────────────────
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.navy }, line: { color: C.navy } });
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 0.4, h: 5.625, fill: { color: C.teal }, line: { color: C.teal } });
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 5.1, w: 10, h: 0.525, fill: { color: C.amber }, line: { color: C.amber } });
s.addText("Key Takeaways", { x: 0.7, y: 0.5, w: 8.6, h: 0.7, fontSize: 28, bold: true, color: C.amber, fontFace: "Calibri" });
const pts = [
"Hand function = extrinsic muscle power + intrinsic muscle precision + intact sensation",
"Intrinsic muscles (lumbricals & interossei) enable the intrinsic-plus position: MCP flexion + IP extension — key for fine motor tasks",
"Median nerve → opposition and precision pinch; Ulnar nerve → grip strength and finger abduction/adduction; Radial nerve → extension",
"Pedretti classifies prehension into power grips (cylindrical, spherical, hook) and precision grips (tip, lateral, three-jaw chuck)",
"OT assessment must address ROM, strength, sensation, and performance in meaningful occupations",
];
const items = pts.map((p, i) => ({
text: p,
options: { bullet: { indent: 14 }, fontSize: 15, color: C.white, breakLine: i !== pts.length - 1 }
}));
s.addText(items, { x: 0.7, y: 1.35, w: 8.8, h: 3.6, fontFace: "Calibri", valign: "top", paraSpaceBefore: 10 });
s.addText("Reference: Pedretti's Occupational Therapy – Practice Skills for Physical Dysfunction, 7th ed.", {
x: 0.7, y: 5.1, w: 8.6, h: 0.4, fontSize: 11, color: C.navy, fontFace: "Calibri", italic: true
});
}
// ─── WRITE FILE ───────────────────────────────────────────────────
pres.writeFile({ fileName: "/home/daytona/workspace/hand-functions-ppt/Hand_Functions_Pedretti_OT.pptx" })
.then(() => console.log("✅ PPTX created successfully"))
.catch(e => { console.error("❌ Error:", e); process.exit(1); });
You've run out of free credits. Sign up for a free account to continue using Orris.
This is a shared conversation. Sign in to Orris to start your own chat.