Chemical and neural regulation of respiration
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
I now have all the information needed for a thorough, well-illustrated answer. Let me compose it.
Chemical and Neural Regulation of Respiration
1. Overview
Respiration is controlled by two interacting systems: a neural (central) system that generates the basic rhythm and coordinates muscle activity, and a chemical system that continuously adjusts ventilation to keep arterial PO2, PCO2, and pH within narrow limits.
"The ultimate goal of respiration is to maintain proper concentrations of O2, CO2, and H+ in the tissues." - Guyton & Hall Textbook of Medical Physiology, p. 533
2. Neural Regulation - The Respiratory Center
The respiratory center is a collection of neurons distributed bilaterally in the medulla oblongata and pons. It is divided into three major areas:
2.1 The Respiratory Centers
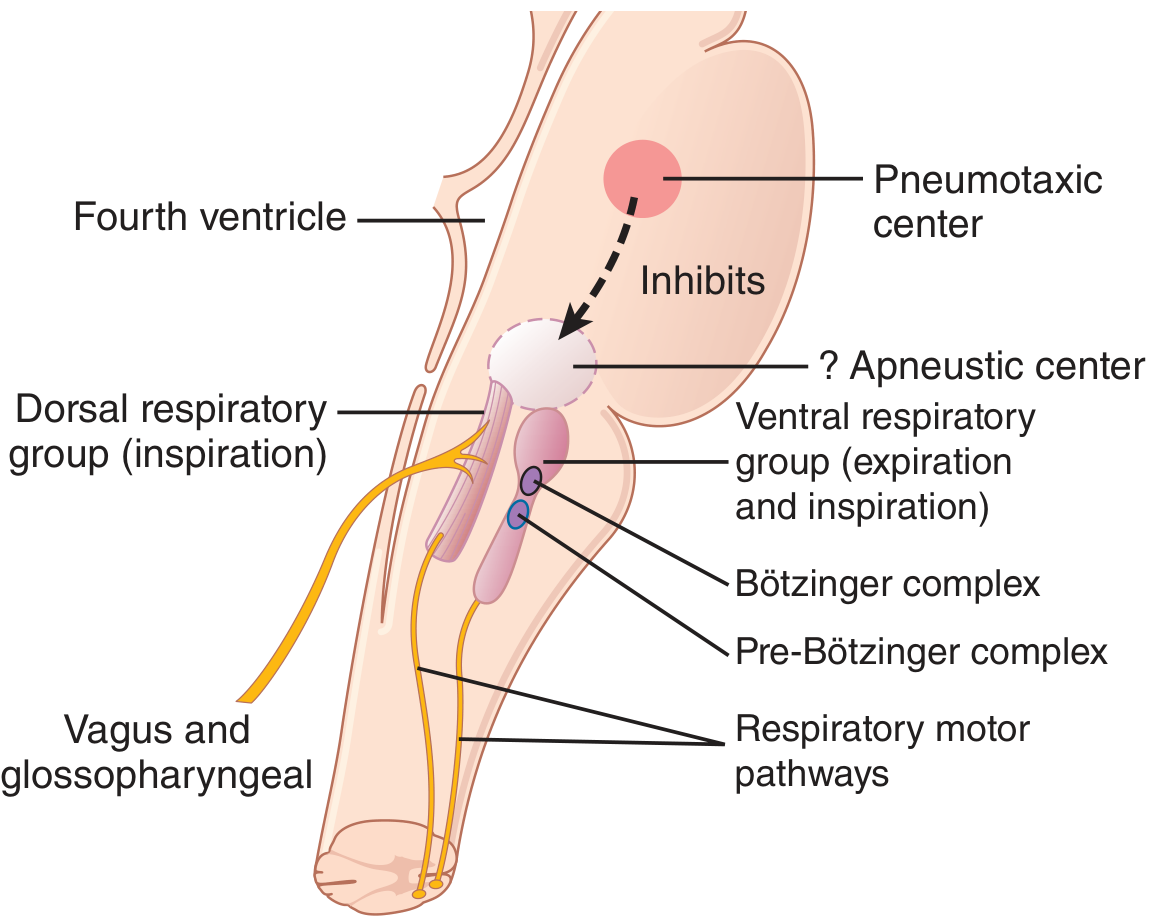
A. Dorsal Respiratory Group (DRG)
- Located in the nucleus tractus solitarius (NTS) in the medulla
- Primarily drives inspiration
- Receives sensory input via vagus (CN X) and glossopharyngeal (CN IX) nerves from peripheral chemoreceptors, baroreceptors, and lung receptors
- Generates rhythmic inspiratory discharges even after sectioning of all peripheral nerves
B. Ventral Respiratory Group (VRG)
- Located in nucleus ambiguus (rostral) and nucleus retroambiguus (caudal)
- Contains neurons for both inspiration and expiration
- Near-silent during quiet breathing (eupnea)
- The Bötzinger complex (rostral VRG) inhibits inspiration to switch to expiration
- The pre-Bötzinger complex contains pacemaker-like neurons that drive the basic respiratory rhythm and project to both DRG and VRG - considered the key component of the respiratory central pattern generator
- The retrotrapezoid nucleus is a major nodal point for CO2/H+ control and active expiration
- Provides powerful expiratory drive to abdominal muscles during heavy breathing
C. Pneumotaxic Center
- Located in the nucleus parabrachialis of the upper pons
- Transmits signals to the inspiratory area to "switch off" inspiration
- Controls duration of the inspiratory ramp signal
- Strong pneumotaxic signal → short inspiration → rate 30-40 breaths/min
- Weak pneumotaxic signal → prolonged inspiration → rate 3-5 breaths/min
The Apneustic Center (lower pons, functionally controversial) - if the pneumotaxic center is removed, prolonged inspiratory gasps (apneusis) occur, suggesting the apneustic center promotes inspiration.
2.2 The Inspiratory "Ramp" Signal
The signal to the diaphragm is not an instantaneous burst but a steadily increasing ramp that:
- Builds up over ~2 seconds of normal inspiration
- Cuts off abruptly for ~3 seconds (allowing passive elastic recoil for expiration)
- Can increase rapidly to fill lungs faster during exercise
Two aspects of the ramp are controlled:
- The rate of increase (determines inspiratory depth)
- The switch-off point (determines respiratory rate)
2.3 Lung Receptors and the Hering-Breuer Reflex
Pulmonary stretch receptors in bronchial/bronchiolar smooth muscle send signals via the vagus to the DRG. When stretched, they inhibit inspiration - the Hering-Breuer inflation reflex. In humans, this reflex activates mainly when tidal volume exceeds ~1.5 L, making it primarily a protective mechanism against over-inflation, not a normal cycle controller.
| Receptor Type | Fiber | Location | Stimulus | Response |
|---|---|---|---|---|
| Slowly adapting stretch | Myelinated | Airway smooth muscle | Lung inflation | Hering-Breuer reflex, bronchodilation |
| Rapidly adapting (irritant) | Myelinated | Airway epithelium | Irritants, histamine | Cough, hyperpnea, bronchoconstriction |
| C fibers (J receptors) | Unmyelinated | Near pulmonary capillaries | Hyperinflation, chemicals | Apnea then rapid breathing, bradycardia |
Source: Ganong's Review of Medical Physiology, 26th ed., p. 664
2.4 Other Neural Inputs
- Proprioceptors in muscles, tendons, and joints stimulate inspiratory neurons during movement - important in exercise hyperpnea
- Pons, hypothalamus, and limbic system influence breathing patterns (emotion, pain, sleep states)
- Baroreceptors (arterial, atrial, ventricular, pulmonary) can modulate respiratory rate
- Coughing, sneezing, swallowing, and vomiting all involve reflex respiratory coordination
3. Chemical Regulation
3.1 Central Chemoreceptors - CO2 and H+
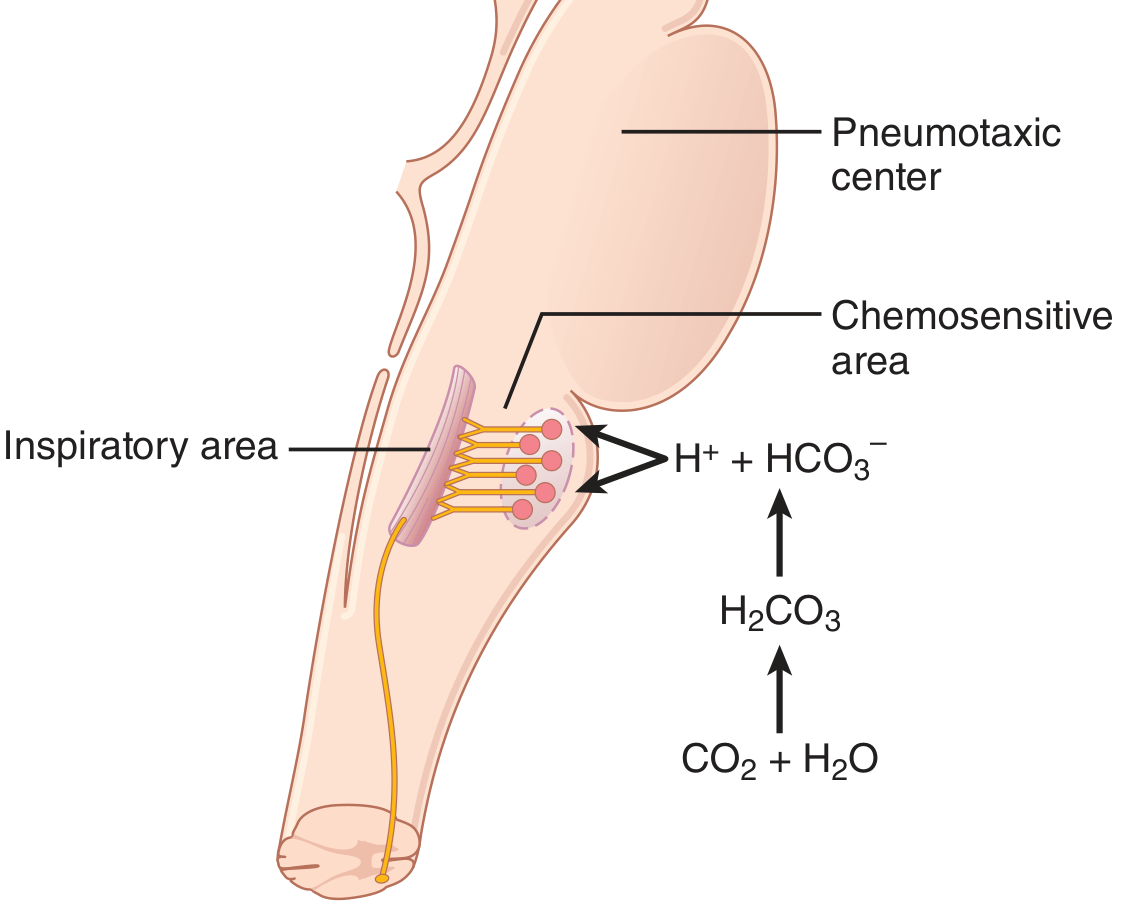
The retrotrapezoid nucleus and adjacent chemosensitive neurons on the ventral surface of the medulla are the primary central chemoreceptors. They are exquisitely sensitive to H+ in CSF and brain interstitial fluid.
Mechanism - why CO2 is more potent than blood H+:
- CO2 crosses the blood-brain barrier freely; blood H+ does not
- CO2 enters the CSF and brain interstitial fluid and reacts: CO2 + H2O → H2CO3 → H+ + HCO3-
- This local H+ directly stimulates the chemosensitive neurons
- Result: blood CO2 changes are ~7x more potent (centrally) than equivalent blood H+ changes
Quantitative effects:
- Arterial PCO2 of 35-75 mmHg range: marked increase in ventilation
- Blood pH 7.3-7.5 range: less than 10% change in ventilation via central receptors alone
- The CO2 drive is the dominant controller of minute-to-minute ventilation
Adaptation over time: After 1-2 days of sustained hypercapnia, the central drive decreases to ~1/5 of its initial level because kidneys increase blood HCO3-, and HCO3- slowly diffuses into CSF, buffering the local H+ stimulus.
3.2 Peripheral Chemoreceptors - O2, CO2, and H+
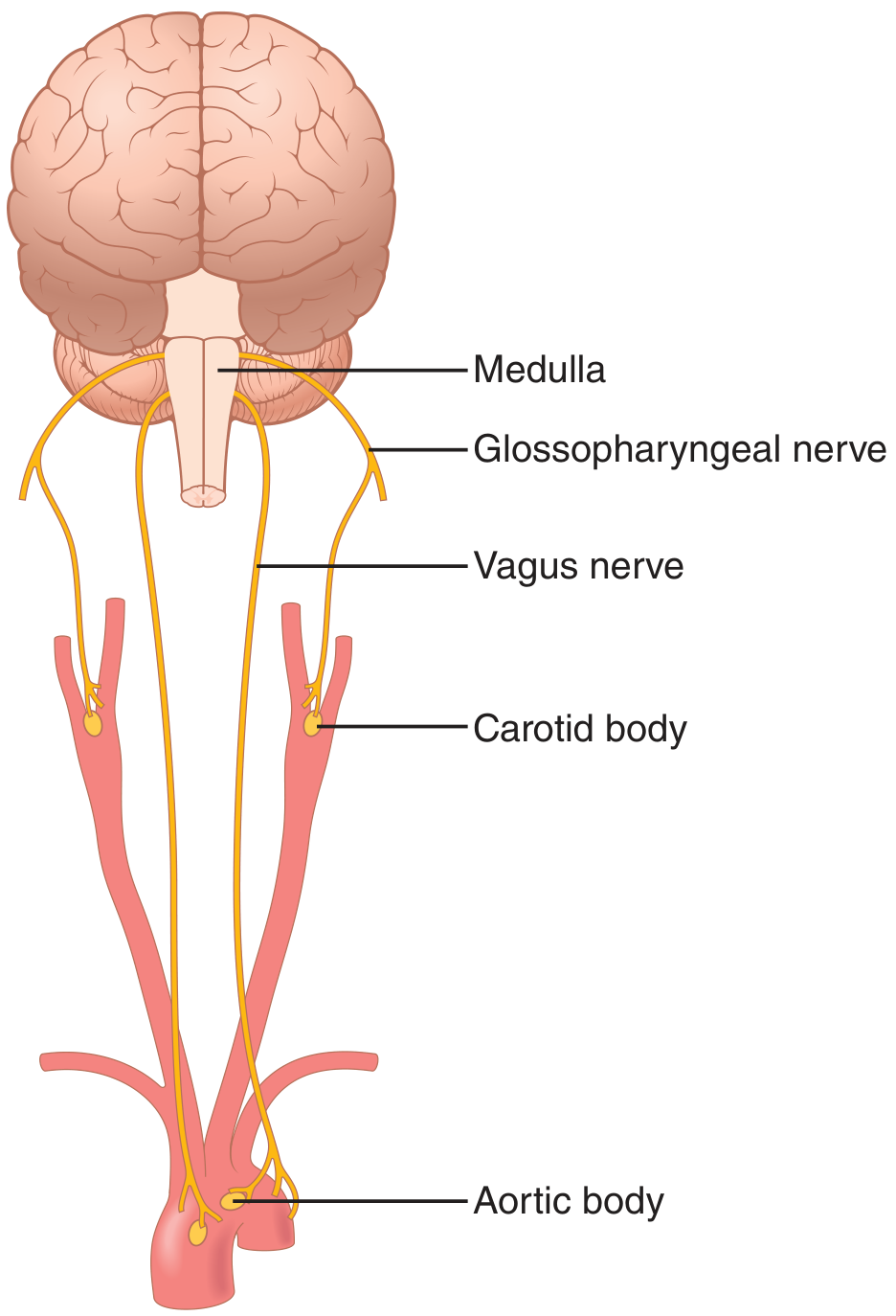
Located at the carotid bifurcations (carotid bodies) and aortic arch (aortic bodies). Afferents travel in Hering's nerve → glossopharyngeal (CN IX) for carotid bodies, and vagus (CN X) for aortic bodies - both terminating in the DRG.
Cell types:
- Type I (glomus) cells - contain dense-core granules with catecholamines (mainly dopamine); directly sense PO2 and transmit via afferent nerve endings
- Type II cells - glia-like, sustentacular function
Mechanism of O2 sensing:
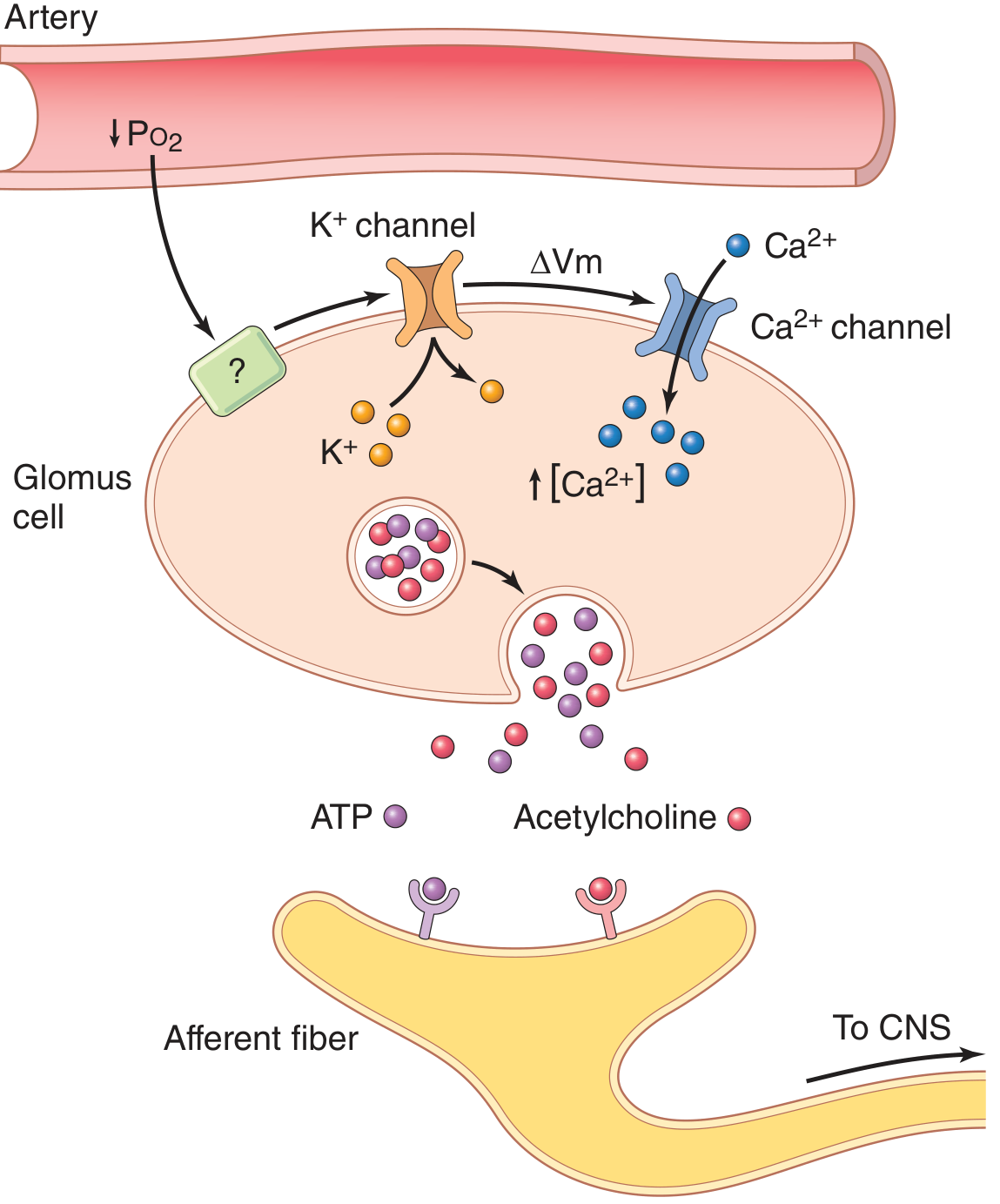
- When arterial PO2 falls below ~60 mmHg, O2-sensitive K+ channels close
- K+ efflux decreases → cell depolarizes
- Voltage-gated L-type Ca2+ channels open → intracellular Ca2+ rises
- Ca2+ triggers release of ATP (primary neurotransmitter), dopamine, and acetylcholine
- Afferent fibers fire → signals travel to CNS → ventilation increases
Blood flow to the carotid bodies is enormous (~2000 mL/100 g/min), so O2 supply is nearly entirely from dissolved O2 in plasma. This is why the chemoreceptors are NOT stimulated in anemia or carbon monoxide poisoning (dissolved PO2 is normal in both), but ARE stimulated in hypoxia with low arterial PO2.
Stimuli for peripheral chemoreceptors (in descending order of potency):
- Low arterial PO2 (mainly <60 mmHg, not responsive to mild hypoxia >100 mmHg)
- Elevated arterial PCO2 (response is about 5x faster than central but only 1/7 as strong)
- Elevated H+ concentration (pH changes >7.3-7.5 range)
- Cyanide (blocks tissue O2 utilization, acts like hypoxia)
- Nicotine, lobeline
- Elevated plasma K+ (relevant during exercise)
Aortic bodies: Functionally similar but less well studied; their contribution is minor - after bilateral carotid body removal, the hypoxic ventilatory response is essentially abolished.
3.3 Role of O2 vs CO2 as Respiratory Controllers
| Feature | CO2/H+ | O2 |
|---|---|---|
| Primary site | Central chemoreceptors (medulla) | Peripheral chemoreceptors |
| Threshold | Graded response over normal range (35-75 mmHg) | No response until PO2 <100 mmHg; strong below 60 mmHg |
| Potency | DOMINANT controller of ventilation | Secondary/backup controller |
| Speed | Slower (minutes) | Faster peripheral response (seconds) |
| Adaptation | Yes, over 1-2 days | Less adaptation |
| Rationale | CO2 directly reflects metabolic rate; Hb-O2 buffer maintains O2 delivery despite wide PO2 variation | PO2 must fall dramatically before Hb-O2 curve shifts significantly |
3.4 Acid-Base and Ventilation
- Metabolic acidosis (e.g., diabetic ketoacidosis): excess blood H+ stimulates peripheral chemoreceptors → Kussmaul breathing (deep, rapid) → CO2 blown off → compensatory respiratory alkalosis
- Metabolic alkalosis (e.g., vomiting with HCl loss): depression of ventilation → CO2 retained → compensatory respiratory acidosis
- Respiratory acidosis: hypoventilation raises PCO2 → stimulates central chemoreceptors → corrective increase in drive
- Respiratory alkalosis: hyperventilation lowers PCO2 → reduces central drive → corrective apnea/hypoventilation
Source: Ganong's Review of Medical Physiology, 26th ed., p. 661
4. Regulation During Exercise
During strenuous exercise, O2 consumption and CO2 production can increase up to 20-fold, yet in healthy individuals, arterial PO2, PCO2, and pH remain nearly normal. The mechanism involves both neural and chemical contributions:
Neural (dominant at onset):
- At the start of exercise, ventilation increases almost instantaneously - before any chemical changes in blood
- Collateral neural signals from motor cortex to exercising muscles simultaneously excite the brain stem respiratory center (analogous to how the vasomotor center is activated)
- Proprioceptive signals from joints and muscles also contribute
Chemical (fine-tuning):
- After ~30-40 seconds, CO2 accumulation catches up to the increased ventilation
- Chemical adjustments (CO2, H+, O2) fine-tune the response to keep blood gases normal
- Plasma K+ increases during exercise and may stimulate carotid body afferents, contributing to hyperpnea
The combined effect: neural signals provide the bulk, immediate ventilatory drive; chemical factors make the final quantitative corrections - neither alone is sufficient for the precise matching seen in healthy exercise.
Summary
| Mechanism | Stimulus | Receptor | Effect |
|---|---|---|---|
| Central chemoreception | ↑ PCO2 / ↑ H+ in CSF | Retrotrapezoid nucleus / ventral medullary neurons | ↑ Ventilation (dominant drive) |
| Peripheral chemoreception | ↓ PO2 (<60 mmHg), ↑ PCO2, ↑ H+ | Carotid/aortic body glomus cells | ↑ Ventilation (backup/rapid) |
| Hering-Breuer reflex | Lung over-inflation | Pulmonary stretch receptors (vagus) | Terminates inspiration |
| J receptor reflex | Pulmonary congestion/emboli | C fibers near capillaries | Apnea → rapid breathing |
| Exercise regulation | Muscle contraction | Motor cortex (collaterals) + proprioceptors | Immediate ↑ ventilation |
| Pneumotaxic center | Inspiratory ramp | Nucleus parabrachialis (upper pons) | Limits inspiration, ↑ rate |
Sources:
- Guyton and Hall Textbook of Medical Physiology, pp. 532-537, 543 (Neural/chemical control, chemoreceptors, exercise)
- Ganong's Review of Medical Physiology, 26th ed., pp. 659-664 (Chemical control, carotid/aortic bodies, lung receptors, acid-base responses)
This is a shared conversation. Sign in to Orris to start your own chat.