Classification of the breast carcinoma
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
I now have comprehensive, well-sourced content to compose a detailed answer. Let me compile it.
Classification of Breast Carcinoma
Breast carcinoma is classified along three main axes: (1) In situ vs. Invasive, (2) Histologic type, and (3) Molecular/Biologic subtype. Understanding all three is essential for prognosis and treatment planning.
I. Broad Division: In Situ vs. Invasive
| Category | Definition |
|---|---|
| Carcinoma in situ (CIS) | Malignant cells confined within ducts/lobules; basement membrane intact |
| Invasive carcinoma | Tumor cells breach the basement membrane and infiltrate stroma |
- Robbins & Kumar Basic Pathology, p. 719
II. Carcinoma In Situ (CIS)
A. Ductal Carcinoma In Situ (DCIS)
DCIS is the most common form of non-invasive breast cancer, typically detected as calcifications on mammography. It is a direct anatomic precursor to invasive ductal carcinoma - when it progresses, invasion occurs in the same breast and usually the same quadrant.
Classification of DCIS (based on nuclear grade and necrosis):
| Histologic Subtype | Nuclear Grade | Necrosis | DCIS Grade |
|---|---|---|---|
| Comedo | High | Extensive | High |
| Intermediate | Intermediate | Focal or absent | Intermediate |
| Non-comedo (solid, cribriform, papillary, micropapillary) | Low | Absent | Low |
- SCHWARTZ'S Principles of Surgery 11th Ed., p. 592
B. Lobular Carcinoma In Situ (LCIS)
- LCIS is a marker of increased risk and a precursor lesion
- It is non-palpable, often an incidental finding
- Unlike DCIS, when invasive cancer develops after LCIS: 2/3 occur in the same breast, 1/3 in the contralateral breast
- Characterized by loss of E-cadherin expression (shared with invasive lobular carcinoma)
- Relative risk of subsequent invasive carcinoma: ~8-10x (25-30%)
- Robbins, Cotran & Kumar Pathologic Basis of Disease
III. Invasive Breast Carcinoma: Histologic Classification
Most breast malignancies are adenocarcinomas, subdivided into ~20 subtypes based on morphology. The original Foote and Stewart classification remains widely used:
1. Invasive Carcinoma of No Special Type (NST) / Invasive Ductal Carcinoma - 75-80%
- Most common histologic subtype
- Also called "scirrhous," "simplex," or formerly "invasive ductal carcinoma NOS"
- Presents as a hard, irregular, radiodense mass with desmoplastic stromal reaction
- Has a characteristic grating sound when cut due to chalky-white stroma and calcification foci
- Heterogeneous group with variable grade and receptor status
- 75% express estrogen receptor (ER)
- Generally worse prognosis than special-type cancers
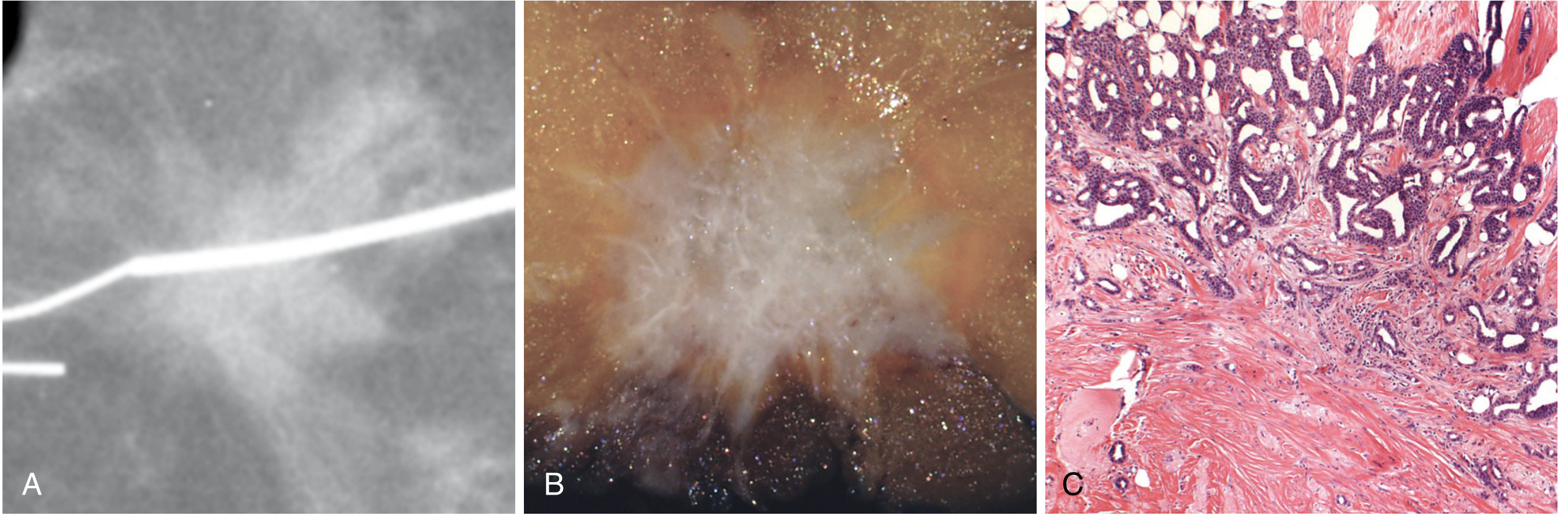
Fig: Invasive carcinoma of no special type. (A) Mammography with irregular radiodense mass. (B) Gross specimen with stellate pattern. (C) Histology showing desmoplastic stromal invasion. - Robbins, Cotran & Kumar
2. Invasive Lobular Carcinoma - ~10%
- Most common special subtype
- Associated with LCIS; shows single-file (Indian file) infiltration pattern through stroma
- E-cadherin negative - loss is characteristic and diagnostic
- Tends to be multifocal and bilateral
- Metastasizes to unusual sites (peritoneum, retroperitoneum, GI tract, meninges)
3. Medullary Carcinoma - ~4%
- Soft, hemorrhagic gross appearance
- Histology: syncytial sheets of high-grade cells + dense lymphocytic infiltrate
- Associated with BRCA1 hereditary breast cancer
- Paradoxically, despite high grade, behavior can be relatively favorable
- Now reclassified in current WHO system as invasive carcinoma NST with "medullary pattern"
4. Mucinous (Colloid) Carcinoma - ~2%
- Islands of tumor cells floating in large pools of extracellular mucin
- Typically low grade, better prognosis
- More common in elderly women
5. Tubular Carcinoma - ~2%
- Well-formed tubular glands with open lumina
- Excellent prognosis; usually Grade 1
- Almost always ER/PR positive, HER2 negative
6. Papillary Carcinoma - ~2%
- Forms fibrovascular papillary fronds
- Includes encapsulated, solid, and invasive papillary subtypes
7. Paget's Disease of the Nipple
- Chronic eczematous eruption of nipple, may progress to ulceration
- Pathognomonic: Paget cells - large, pale, vacuolated cells in the rete pegs of nipple epithelium
- Almost always associated with underlying DCIS, and sometimes invasive carcinoma
- Distinguished from melanoma by: CEA positive (Paget's) vs S-100 positive (melanoma)
8. Inflammatory Breast Carcinoma
- Clinically defined: erythema, skin thickening, peau d'orange, warmth - mimics mastitis
- Pathologically: tumor emboli in dermal lymphatics
- Most aggressive presentation; often presents as locally advanced disease
- High-grade, often ER-negative
9. Rare Special Types
- Adenoid cystic carcinoma
- Squamous cell carcinoma
- Apocrine carcinoma
- Metaplastic carcinoma
Note: To qualify as a "special type," at least 90% of the tumor must show the defining histologic features. - Schwartz's Surgery 11th Ed.
IV. Histologic Grading (Nottingham System)
All invasive carcinomas are graded using the Nottingham Histologic Score based on 3 criteria:
| Feature | Score 1 | Score 2 | Score 3 |
|---|---|---|---|
| Tubule formation | >75% | 10-75% | <10% |
| Nuclear pleomorphism | Mild | Moderate | Marked |
| Mitotic rate | Low | Moderate | High |
| Total Score | Grade |
|---|---|
| 3-5 | Grade 1 - Well differentiated |
| 6-7 | Grade 2 - Moderately differentiated |
| 8-9 | Grade 3 - Poorly differentiated |
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 978
V. Molecular/Biologic Classification (Gene Expression Profiling)
Based on gene expression patterns, breast carcinomas are divided into 4 major molecular subtypes with distinct IHC profiles, clinical behavior, and treatment implications:
| Subtype | Morphology | Receptor Profile | Key Features |
|---|---|---|---|
| Luminal A | Low grade ductal | ER+, PR±, HER2-, low Ki67 | CK8/18+; most common; best prognosis; sensitive to endocrine therapy; variable chemo response |
| Luminal B | High grade ductal | ER+, PR+, HER2+, high Ki67 | More aggressive than Luminal A; tends to respond to endocrine therapy; may need chemo |
| HER2-enriched | High grade | ER-, PR-, HER2 amplified | High grade; sensitive to HER2-targeted therapy (trastuzumab); poorer prognosis without targeted therapy |
| Basal-like / Triple Negative (TNBC) | High grade; solid growth; necrosis | ER-, PR-, HER2-; CK5/6+, p63+ | High Ki67; associated with BRCA1 mutations; aggressive; chemosensitive but no targeted therapy standard; worst prognosis |
Important distinction: "Basal-like" and "Triple Negative" are not synonymous:
-
Most basal-like tumors are triple negative
-
But many triple-negative tumors do NOT have basal-like features
-
Quick Compendium of Clinical Pathology 5th Ed.; Robbins, Cotran & Kumar Pathologic Basis of Disease
VI. Clinical Biologic Grouping (AJCC 8th Edition)
The AJCC 8th edition combines anatomic stage with molecular group to create prognostic stage groups:
- ER-positive / HER2-negative (Luminal A/B) - most common ~70%
- HER2-positive - ~15-20%
- Triple Negative (ER/PR/HER2 negative) - ~15%
These groups differ in:
-
Patient demographics
-
Grade distribution
-
Mutation profile
-
Metastatic pattern
-
Response to therapy
-
Time to recurrence and prognosis
-
Robbins, Cotran & Kumar Pathologic Basis of Disease; Robbins & Kumar Basic Pathology, p. 719
Summary Diagram
BREAST CARCINOMA
│
├── IN SITU
│ ├── DCIS (Ductal) → High/Intermediate/Low grade (Comedo / Non-comedo)
│ └── LCIS (Lobular) → Risk marker + precursor
│
└── INVASIVE
│
├── HISTOLOGIC TYPE
│ ├── No Special Type (NST) / IDC - 75-80%
│ ├── Invasive Lobular Carcinoma - 10%
│ ├── Medullary - 4%
│ ├── Mucinous/Colloid - 2%
│ ├── Tubular - 2%
│ ├── Papillary - 2%
│ ├── Paget's Disease of Nipple
│ ├── Inflammatory Carcinoma
│ └── Rare (adenoid cystic, squamous, apocrine)
│
├── HISTOLOGIC GRADE (Nottingham)
│ ├── Grade 1 (Well differentiated)
│ ├── Grade 2 (Moderately differentiated)
│ └── Grade 3 (Poorly differentiated)
│
└── MOLECULAR SUBTYPE
├── Luminal A (ER+, HER2-, low Ki67) → best prognosis
├── Luminal B (ER+, HER2+, high Ki67) → intermediate
├── HER2-enriched (ER-, HER2+) → treat with trastuzumab
└── Triple Negative / Basal-like (ER-, PR-, HER2-) → worst prognosis
Classification of the breast carcinoma robbins
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
I now have all the content needed from Robbins, Cotran & Kumar (Pathologic Basis of Disease) to give a thorough, image-rich answer. Here is the full classification as presented in Robbins:
Classification of Breast Carcinoma - Robbins, Cotran & Kumar
Source: Robbins, Cotran & Kumar - Pathologic Basis of Disease (Latest Edition), Chapter 23
All breast carcinomas arise from cells of the terminal duct lobular unit (TDLU). The terms "ductal" and "lobular" do not reflect the actual cell of origin - they describe growth patterns that reflect differences in tumor cell genetics and biology.
PART 1: IN SITU CARCINOMA
Carcinoma in situ refers to cancer cells confined within ducts and lobules by an intact basement membrane. Importantly, many (if not all) molecular changes found in invasive carcinoma are already present at the in situ stage.
A. Ductal Carcinoma In Situ (DCIS)
DCIS is a neoplastic proliferation of epithelial cells limited to ducts and lobules, with myoepithelial cells generally preserved. It can spread throughout the ductal system and produce extensive disease involving an entire breast segment.
Detection: Almost always by mammography - most present as calcifications, less commonly as a density/mass, rarely as nipple discharge.
Two biologically distinct grades:
| Feature | Low-Grade DCIS | High-Grade DCIS |
|---|---|---|
| ER/HER2 | ER-positive, HER2-negative | May be ER-negative and/or HER2-positive |
| Molecular alterations | 16q loss, 1q gain (low-grade pathway) | Genomic instability, chromosomal changes |
| Necrosis | Absent/minimal | Central (comedo) necrosis common |
| Progression | Slow (~1% per year to invasion) | Higher risk, more rapid progression |
Architectural patterns of DCIS:
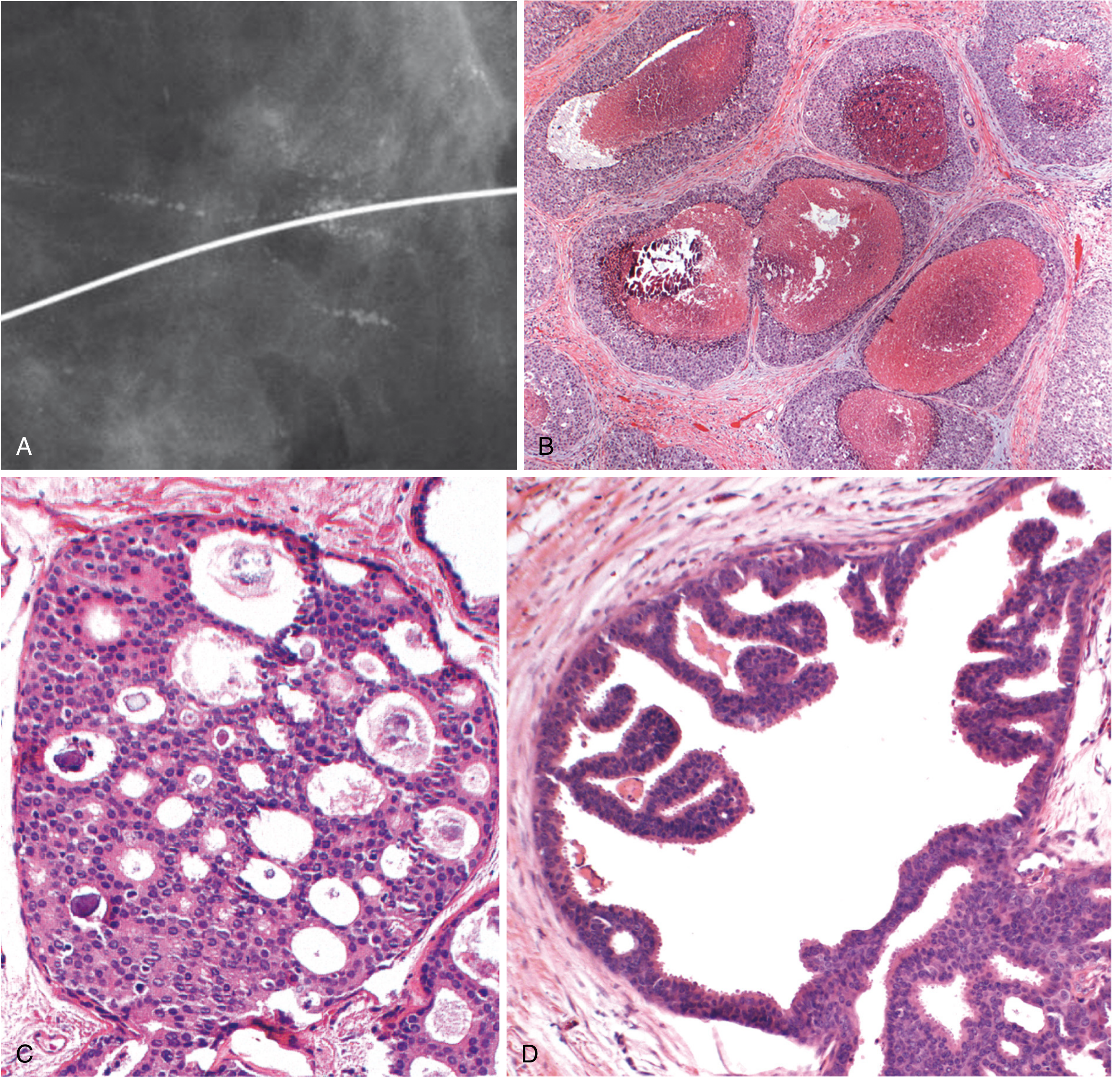
Fig. 23.12 - Robbins, Cotran & Kumar: DCIS patterns. (A-B) High-grade DCIS with comedo necrosis and calcifications. (C) Cribriform pattern - "cookie cutter" spaces. (D) Micropapillary pattern - projections without fibrovascular cores.
Architectural sub-patterns of DCIS:
- Comedo - high-grade cells with large central necrosis; calcifications linear/branching on mammogram
- Cribriform - rounded "cookie cutter" spaces filled with calcifying secretions
- Micropapillary - complex bulbous protrusions without fibrovascular cores
- Papillary - true papillae with fibrovascular cores, lacks myoepithelial layer
- Solid - sheets of cells fill and distend ducts
Clinical course:
- Low-grade DCIS: ~1% per year risk of invasion (ipsilateral, same quadrant)
- High-grade or extensive DCIS: higher risk and faster progression
- Death from metastatic disease after DCIS diagnosis: only 1-3%
Paget Disease of the Nipple
A rare manifestation of DCIS (1-4% of breast cancers) in which DCIS extends via the lactiferous ducts into the skin of the nipple without crossing the basement membrane.
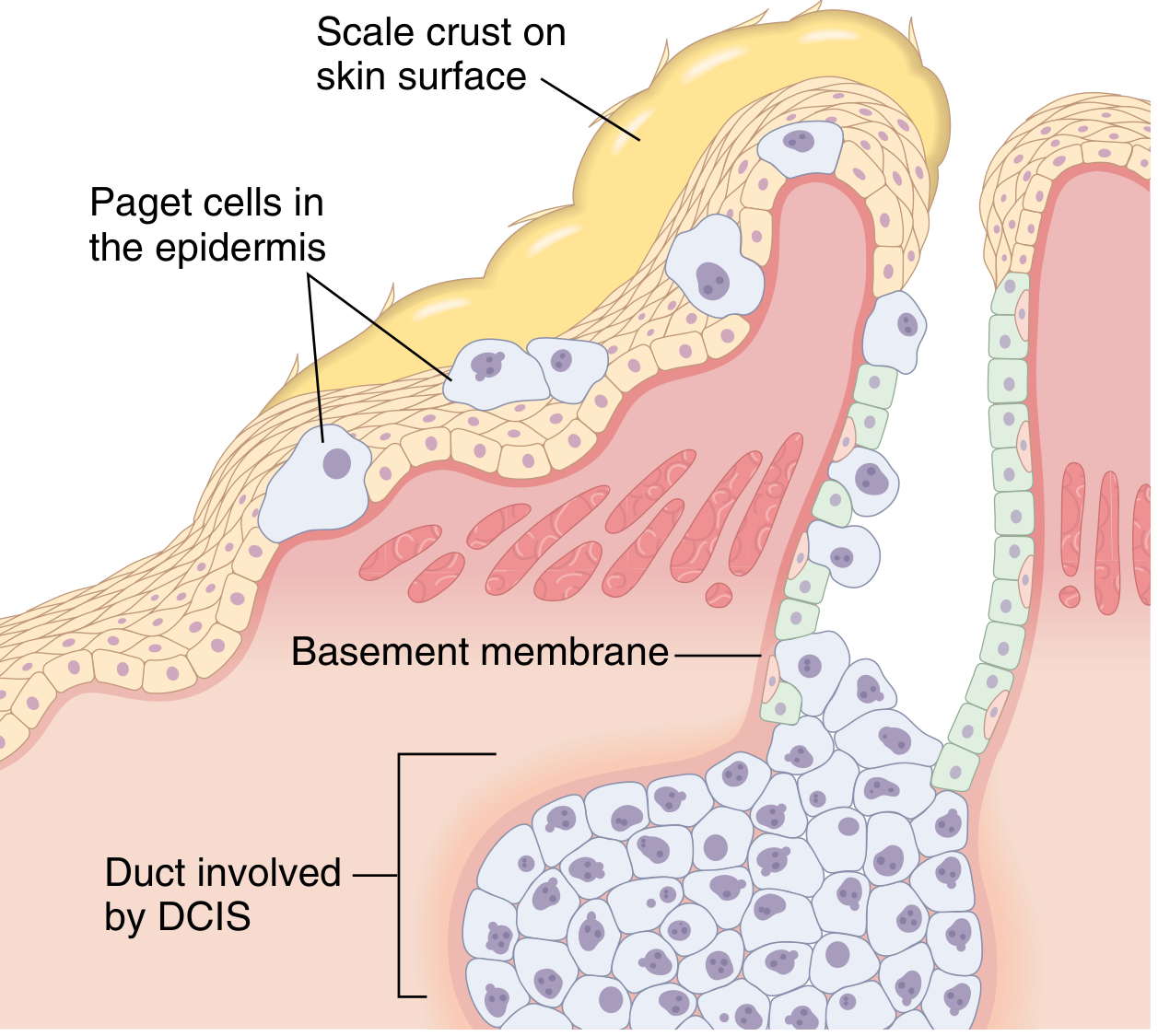
Fig. 23.13 - Robbins: DCIS extends up lactiferous ducts into nipple skin. Paget cells disrupt the epithelial barrier, causing an oozing, scaly crust.
- Presents as unilateral erythematous eruption with scale crust; pruritus is common
- Paget cells = large, pale, vacuolated malignant cells in nipple epidermis
- Underlying palpable mass: ~50% of cases → these usually have invasive carcinoma
- Without palpable mass: usually pure DCIS, staged as such
- Prognosis depends on features of any underlying invasive carcinoma
B. Lobular Carcinoma In Situ (LCIS)
- Clonal proliferation within lobules with characteristic dyscohesive cells
- Loss of E-cadherin expression - shared with invasive lobular carcinoma (diagnostic marker)
- Molecular features similar to low-grade ER-positive invasive carcinoma
- Acts as both a risk marker (increased risk both breasts) and precursor lesion
- Risk of invasive carcinoma: ~8-10x relative risk (25-30% lifetime)
PART 2: INVASIVE CARCINOMA
Histologic Subtype Classification
Most breast malignancies are adenocarcinomas, subdivided into ~20 subtypes based on morphology.
1. Invasive Carcinoma of No Special Type (NST) - ~75%
Also formerly called "invasive ductal carcinoma, NOS." The largest, most heterogeneous group.
Gross/mammographic features:
- Hard, irregular, radiodense mass with irregular margins
- Desmoplastic stromal reaction - produces characteristic grating sound when cut
- Chalky-white stroma with foci of calcification
- Less commonly: well-circumscribed mass with scant stroma, or scattered infiltrating glands
Note: High-grade NST tumors with prominent tumor-infiltrating lymphocytes (TILs) were previously called "medullary carcinoma" - this entity proved not to be diagnostically reproducible and is now classified as invasive carcinoma NST with medullary pattern.
Fig. 23.20 - Robbins: NST carcinoma. (A) Irregular radiodense margins on mammography. (B) Gross stellate, fibrotic mass. (C) Desmoplastic stromal response on histology.
Nottingham Histologic Grade (all invasive carcinomas graded this way):
| Parameter | Score 1 | Score 2 | Score 3 |
|---|---|---|---|
| Tubule formation | >75% | 10-75% | <10% |
| Nuclear pleomorphism | Mild | Moderate | Marked |
| Mitotic rate | Low | Moderate | High |
| Total Score | Grade | Description |
|---|---|---|
| 3-5 | Grade 1 | Well-differentiated; tubular/cribriform growth, small uniform nuclei, low proliferation |
| 6-7 | Grade 2 | Moderately differentiated; solid clusters + single cells, greater pleomorphism |
| 8-9 | Grade 3 | Poorly differentiated; ragged nests/solid sheets, enlarged irregular nuclei, necrosis common |
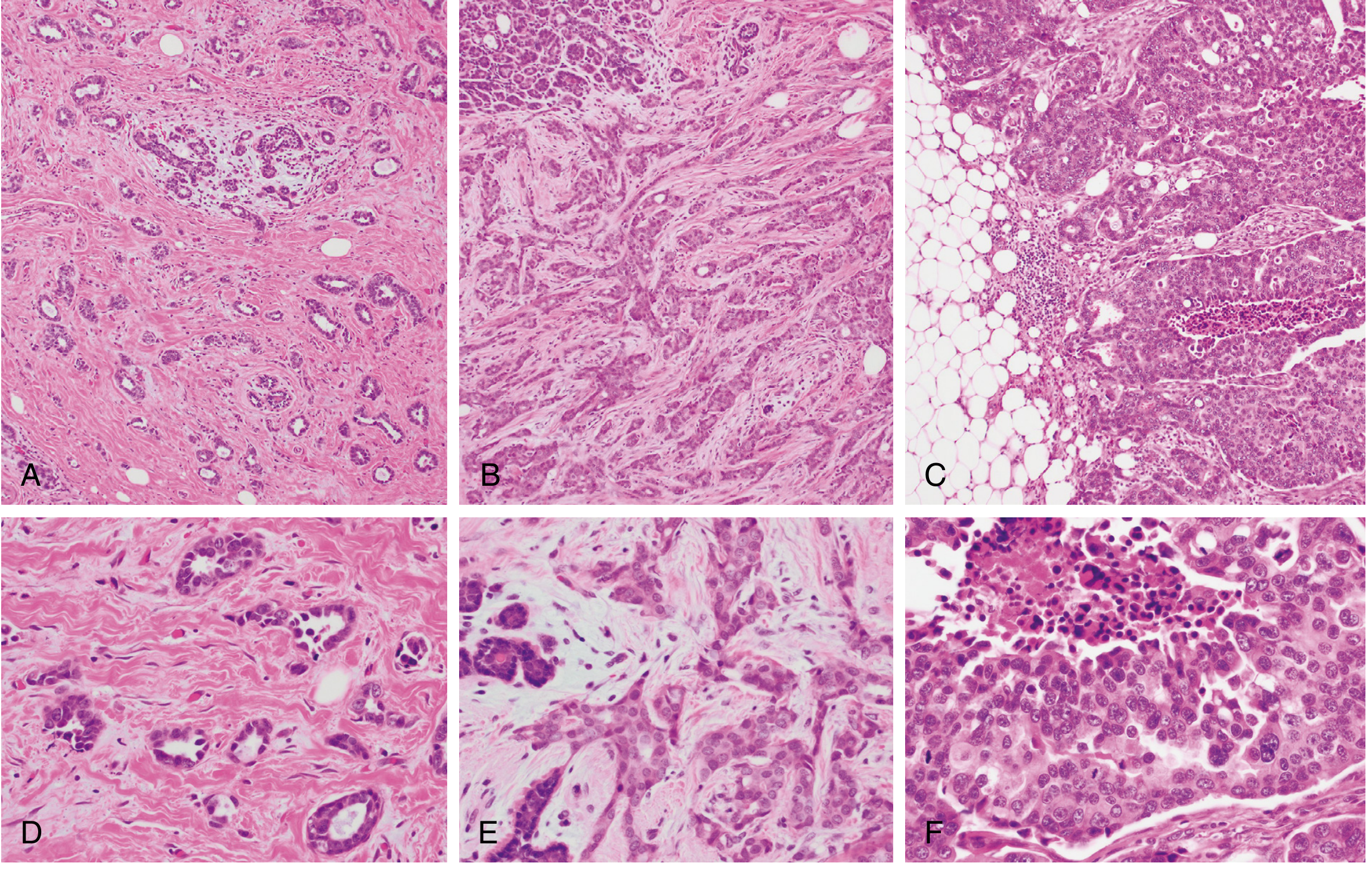
Fig. 23.21 - Robbins: Nottingham grading. Top row (A-C): Low-power Grade 1 (tubular), Grade 2 (mixed), Grade 3 (solid sheets). Bottom row (D-F): High-power views showing increasing nuclear pleomorphism and mitoses.
2. Special Histologic Subtypes
Special subtypes require that their defining features be present in the majority of the tumor. They are organized by their usual molecular group:
Luminal (ER-positive / HER2-negative) Special Types
| Subtype | Frequency | Key Morphology | Prognosis |
|---|---|---|---|
| Invasive Lobular Carcinoma | Up to 15% | Dyscohesive cells in single-file linear cords; signet ring cells; E-cadherin negative; minimal desmoplasia | Intermediate; distinct metastatic pattern |
| Mucinous (Colloid) Carcinoma | Uncommon | Tumor cell clusters floating in large extracellular lakes of mucin; soft/gelatinous gross appearance | Favorable |
| Tubular Carcinoma | Uncommon | Exclusively well-formed tubules; sometimes mistaken for benign sclerosing lesion | Excellent |
| Cribriform Carcinoma | Uncommon | Invasive nests with cribriform (sieve-like) morphology | Excellent |
| Papillary Carcinoma | Uncommon | True papillary fronds lined by tumor cells | Good |
Invasive lobular carcinoma - special features:
- Second most common invasive subtype (up to 15%)
- Loss of E-cadherin → dyscohesive cells
- CDH1 germline mutations increase risk of lobular breast carcinoma AND signet ring gastric carcinoma
- Unique metastatic sites: peritoneum, retroperitoneum, leptomeninges, GI tract, ovaries, uterus
- Difficult to detect on imaging due to minimal desmoplasia and diffuse infiltration
HER2-Positive Special Types
| Subtype | Key Morphology |
|---|---|
| Apocrine Carcinoma | Cells resemble sweat gland cells; enlarged round nuclei with prominent nucleoli; abundant eosinophilic/granular cytoplasm |
| Invasive Micropapillary Carcinoma | Hollow balls of cells floating within intercellular fluid; mimic papillae but lack true fibrovascular cores |
Triple-Negative (ER/PR/HER2-negative) Special Types
| Subtype | Key Features | Prognosis |
|---|---|---|
| Metaplastic Carcinoma | Squamous or mesenchymal (spindle/chondroid/osseous) differentiation; myoepithelial gene expression profile | Poor (mostly) |
| Adenoid Cystic Carcinoma | Resembles salivary gland tumor; biphasic pattern | Favorable |
| Mucoepidermoid Carcinoma | Resembles salivary gland tumor | Favorable |
| Secretory Carcinoma | Often in young patients; secretory vacuoles | Favorable |
Note: The rare indolent TNBC subtypes (adenoid cystic, secretory, mucoepidermoid) are "salivary gland-like" tumors with an excellent prognosis despite being triple negative.
PART 3: MOLECULAR/BIOLOGIC CLASSIFICATION
Based on gene expression profiling, breast carcinomas cluster into 3 major molecular groups, each with distinct biology, clinical behavior, and targeted treatments:
| Molecular Group | IHC Profile | Key Biology | Prognosis | Targeted Therapy |
|---|---|---|---|---|
| Luminal A | ER+, PR+, HER2-, low Ki67 | Low proliferation; ER-driven | Best | Endocrine therapy (tamoxifen, aromatase inhibitors) |
| Luminal B | ER+, PR±, HER2±, high Ki67 | Higher proliferation than A | Intermediate | Endocrine therapy + CDK4/6 inhibitors ± chemo |
| HER2-enriched | ER-, PR-, HER2-amplified | HER2 gene amplification; high grade | Intermediate-poor without HER2-targeting | Trastuzumab, T-DM1, lapatinib |
| Triple Negative (TNBC) / Basal-like | ER-, PR-, HER2-; CK5/6+, p63+ | BRCA1 silencing; genomic instability; TP53 mutation; high grade | Worst | PARP inhibitors (if BRCA mutated); chemotherapy; immune checkpoint |
Key distinctions (Robbins):
- Luminal A vs. B: differ mainly in proliferative rate (Ki67)
- HER2 cancers: defined by HER2 overexpression due to gene amplification; respond well to HER2 inhibitors
- TNBC: often associated with BRCA1 silencing or TP53 mutation; typically high-grade solid tumors with necrosis and very high proliferation
- A small subset of low-grade TNBC exists with excellent prognosis (e.g., secretory carcinoma, adenoid cystic) - these are biologically distinct
"Basal-like" and "triple negative" are not synonymous - most basal-like tumors are TNBC, but many TNBCs do not have basal-like features.
PART 4: STAGING - AJCC 8th Edition
The AJCC 8th edition combines anatomic stage (tumor size, nodal status, metastasis) with molecular group to create prognostic stage groups that better estimate likely survival.
| Factor | Significance |
|---|---|
| Biologic subtype (ER, PR, HER2, Ki67) | Most powerful prognostic variable |
| Anatomic extent (TNM stage) | Combined with molecular group |
| Grade (Nottingham) | Feeds into molecular-anatomic staging |
Prognosis is dependent on both biologic features and the extent of cancer at the time of diagnosis.
Summary Flowchart (Robbins Framework)
BREAST CARCINOMA (all from TDLU)
│
├── IN SITU (basement membrane intact)
│ ├── DCIS ──── Low-grade (ER+, HER2−, 16q loss)
│ │ High-grade (ER−/HER2+, genomic instability)
│ │ Patterns: comedo, cribriform, micropapillary, papillary, solid
│ │ + Paget disease of nipple (DCIS → nipple skin)
│ └── LCIS ──── E-cadherin negative; risk marker + precursor
│
└── INVASIVE (basement membrane breached)
│
├── NO SPECIAL TYPE (NST) ~75% ── Graded I, II, III (Nottingham)
│
├── SPECIAL TYPES (organized by molecular group)
│ ├── Luminal (ER+/HER2−): Lobular, Mucinous, Tubular, Cribriform, Papillary
│ ├── HER2+: Apocrine, Micropapillary
│ └── TNBC: Metaplastic (aggressive); Adenoid cystic/Secretory (favorable)
│
└── MOLECULAR GROUPS
├── Luminal A (ER+, low Ki67) ── best prognosis
├── Luminal B (ER+, high Ki67) ── intermediate
├── HER2-enriched (HER2 amp) ── trastuzumab-sensitive
└── TNBC / Basal-like (ER−PR−HER2−) ── worst prognosis
- Robbins, Cotran & Kumar Pathologic Basis of Disease, Chapter 23, pp. 966-984
Breast carcinoma Pathology
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
I now have a comprehensive body of text and images from Robbins. Let me compile the full pathology answer.
Breast Carcinoma - Complete Pathology
Robbins, Cotran & Kumar - Pathologic Basis of Disease, Chapter 23
OVERVIEW
Breast cancer is the most common malignancy globally and the leading cause of cancer death in females worldwide. In 2020, it surpassed lung cancer as the most common cancer overall with ~2.3 million new cases (almost 12% of all new cancer diagnoses). The lifetime risk is 1 in 8 for females living to age 90 in the United States.
Breast cancer is a heterogeneous disease defined by distinct clinical, morphological, and molecular phenotypes. Classification is based on three parallel approaches:
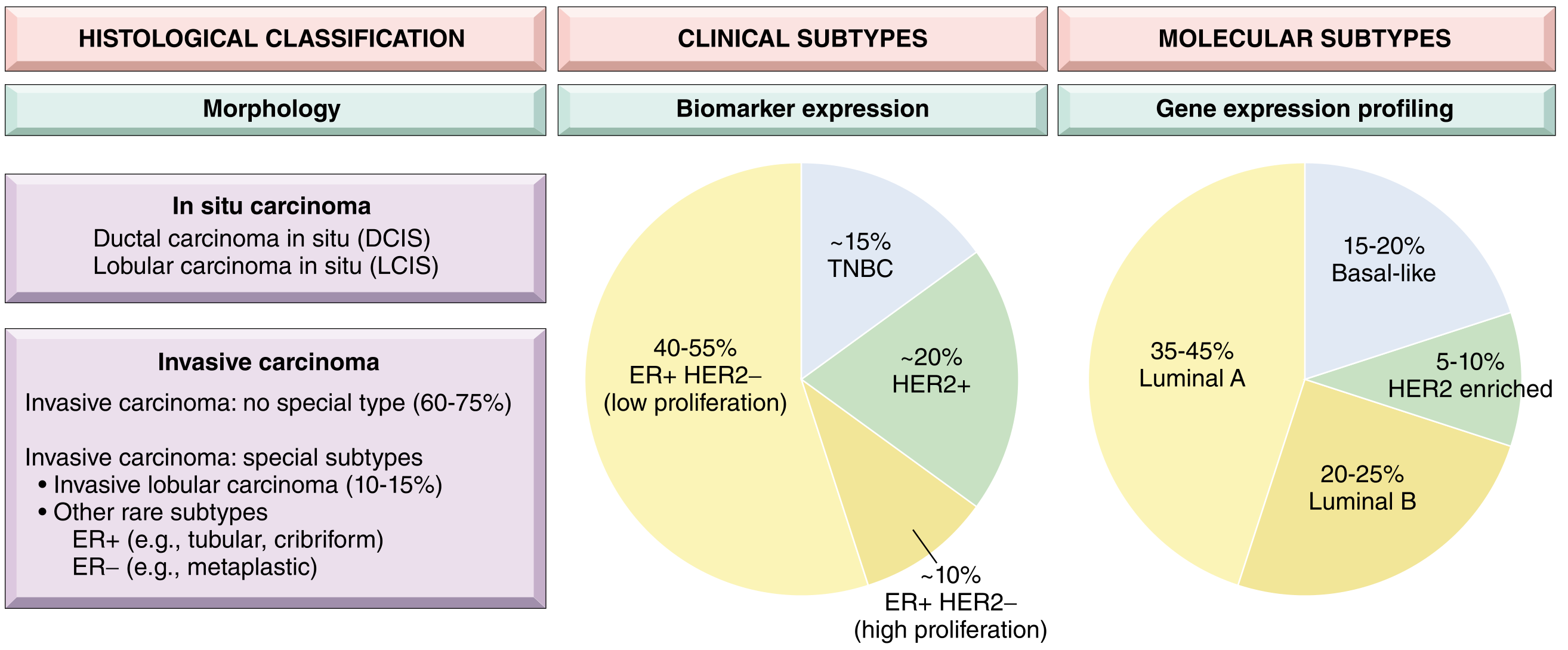
Fig. 23.15 - Robbins: Breast cancer classification based on morphology, biomarkers, and gene expression profiling.
EPIDEMIOLOGY & RISK FACTORS
Age & Incidence Patterns
- Rare before age 25; increases rapidly after age 30
- Luminal (ER+) cancer: incidence continues to rise with age and peaks late in life
- TNBC & HER2 cancer: incidence plateaus in middle age (~40 years)
- Therefore, TNBC/HER2 cancers account for nearly half of breast cancers in young females vs. <20% in older females
Hormonal Risk Factors
- Prolonged estrogenic stimulation (early menarche, late menopause, nulliparity, late first pregnancy, exogenous postmenopausal hormones)
- Hormone receptor-positive tumors are especially susceptible to estrogen-driven proliferation
Genetic/Familial Risk
25-35% of breast cancers are familial. High-penetrance single-gene mutations account for 8-17% of all cases:
| Gene (Syndrome) | % of Single Gene Cancers | Risk by Age 70 | Tumor Type |
|---|---|---|---|
| BRCA1 (HBOC) | ~55% | 40-90% (females) | Majority are TNBC |
| BRCA2 (HBOC) | ~35% | 30-60% (females); 6% (males) | Majority are ER-positive |
| PALB2 | <1% | 30-60% | ER+ or TNBC |
| TP53 (Li-Fraumeni) | <1% | 50-60% | ER+ and HER2+ |
| PTEN (Cowden) | <1% | 20-80% | Apocrine differentiation |
| CDH1 (Hereditary diffuse gastric cancer) | <1% | ~50% | Lobular carcinoma |
| STK11 (Peutz-Jeghers) | <1% | 40-60% | — |
BRCA1 and BRCA2 mutations together account for 80-90% of single-gene familial breast cancers and ~3-6% of all breast cancers. Both genes encode proteins involved in DNA repair by homologous recombination (HRR).
PATHOGENESIS
Cell of Origin
All breast carcinomas arise from cells of the terminal duct lobular unit (TDLU), regardless of whether they are called "ductal" or "lobular." These terms reflect growth pattern/genetics, not cell of origin.
Two Major Pathways of Breast Cancer Evolution (Low-grade vs. High-grade)
Low-Grade Pathway:
- Progression: Columnar cell lesions → Flat epithelial atypia → Atypical ductal hyperplasia → Low-grade DCIS → Low-grade invasive carcinoma
- Molecular hallmarks: 16q deletion, 1q gain
- Phenotype: ER-positive/HER2-negative (Luminal A)
- Slow, stepwise accumulation of mutations
High-Grade Pathway:
- More complex, often arising de novo or from high-grade DCIS
- Molecular hallmarks: TP53 mutation, genomic instability, chromosomal changes
- Phenotypes: HER2-enriched, TNBC/basal-like
- More aggressive biological behavior
Tumor Microenvironment
- Cancer-associated fibroblasts (CAFs) facilitate adhesion, ECM remodeling, and immunosuppression
- Myoepithelial cell loss creates gaps in the basement membrane, predisposing to stromal invasion
- Tumor cells upregulate PD-L1 (immune checkpoint) to evade host immune response
PART I: CARCINOMA IN SITU
A. Ductal Carcinoma In Situ (DCIS)
Neoplastic proliferation of epithelial cells confined within ducts and lobules - basement membrane intact, myoepithelial cells generally preserved.
Detection: Almost exclusively by mammography (calcifications, rarely a density)
Two biologically distinct grades:
| Feature | Low-grade DCIS | High-grade DCIS |
|---|---|---|
| ER/HER2 | ER+, HER2- | May be ER- and/or HER2+ |
| Molecular changes | 16q loss, 1q gain | Genomic instability |
| Necrosis | Absent/minimal | Central (comedo) necrosis |
| Rate of invasion | ~1%/year | Higher; faster progression |
Architectural patterns:
- Comedo: High-grade cells + large central necrosis; linear/branching calcifications on mammogram
- Cribriform: "Cookie-cutter" rounded spaces filled with calcifying secretions
- Micropapillary: Bulbous protrusions without fibrovascular cores
- Papillary: True papillae with fibrovascular cores; lacks myoepithelial layer
- Solid: Sheets of cells filling and distending ducts
Fig. 23.12 - Robbins: DCIS patterns. (A) Mammographic calcifications. (B) High-grade DCIS with comedo necrosis. (C) Cribriform DCIS - "cookie cutter" spaces. (D) Micropapillary DCIS.
Natural history:
- Females with small, low-grade DCIS: ~1% per year invasion risk
- Invasive cancer in the same breast quadrant with same grade/receptor profile as DCIS
- Death from metastatic disease after DCIS: only 1-3%
- Overall death rate after DCIS diagnosis is lower than the general population (partly reflects better access to care)
Paget Disease of the Nipple
- Rare manifestation (1-4% of cases)
- DCIS extends via lactiferous ducts into nipple skin WITHOUT crossing the basement membrane
- Paget cells: Large, pale, vacuolated malignant cells within nipple epidermis
- Presentation: Unilateral erythematous eruption with scale crust; pruritus; may be mistaken for eczema
- ~50% have a palpable mass (usually invasive carcinoma underneath)
- Without palpable mass: usually pure DCIS, staged as such
- Prognosis depends on features of underlying invasive carcinoma (if present)
Fig. 23.13 - Robbins: DCIS extends up lactiferous ducts into nipple skin. Paget cells disrupt the epithelial barrier, causing oozing and scale crust.
B. Lobular Carcinoma In Situ (LCIS)
- Clonal proliferation of dyscohesive cells within lobules
- Loss of E-cadherin (CDH1) expression - shared with invasive lobular carcinoma
- Molecular features overlap with low-grade ER-positive invasive carcinoma
- Serves as both a risk marker (both breasts) and direct precursor (ipsilateral)
- Risk of invasive carcinoma: ~8-10x relative risk (~25-30% lifetime risk)
PART II: INVASIVE CARCINOMA
A. Histologic Classification
Most breast carcinomas are adenocarcinomas, subdivided into ~20 subtypes.
1. Invasive Carcinoma of No Special Type (NST) - ~75%
Also called "invasive ductal carcinoma, NOS." The largest and most heterogeneous group.
Gross/Radiologic:
- Hard, irregular, radiodense mass with irregular margins on mammography
- Stellate, fibrotic cut surface with desmoplastic stroma
- Characteristic grating sound when cut - due to chalky-white stroma and calcifications
Microscopic patterns:
- Most common: small clusters/nests/glands infiltrating stroma with desmoplastic reaction
- Less common: well-circumscribed mass with scant stroma (sheets of cells)
- Rare: scattered single cells infiltrating fibrofatty tissue (mimics lobular)
- High-grade NST with prominent tumor-infiltrating lymphocytes (TILs) = "medullary pattern" (previously called medullary carcinoma - no longer a reproducible entity)
Fig. 23.20 - Robbins: NST carcinoma: irregular mass on imaging (A), gross stellate appearance (B), desmoplastic stroma on histology (C).
Nottingham Histologic Grading (applies to all invasive carcinomas)
| Criterion | Score 1 | Score 2 | Score 3 |
|---|---|---|---|
| Tubule formation | >75% | 10-75% | <10% |
| Nuclear pleomorphism | Mild | Moderate | Marked |
| Mitotic rate | Low | Moderate | High |
| Total Score | Grade | Appearance |
|---|---|---|
| 3-5 | Grade 1 (well differentiated) | Tubular/cribriform growth; small uniform nuclei; rare mitoses |
| 6-7 | Grade 2 (moderately differentiated) | Mixed tubules + solid nests; pleomorphic nuclei; occasional mitoses |
| 8-9 | Grade 3 (poorly differentiated) | Ragged sheets; enlarged irregular nuclei; necrosis; high mitoses |
Fig. 23.21 - Robbins: Nottingham grading. (A,D) Grade 1: tubule-forming cells with monomorphic nuclei. (B,E) Grade 2: less tubule formation, pleomorphic nuclei, occasional mitoses. (C,F) Grade 3: solid sheets, marked pleomorphism, tumor necrosis.
2. Special Histologic Subtypes
Organized by molecular group:
Luminal (ER+/HER2-) Special Types
| Subtype | Morphology | Key Features | Prognosis |
|---|---|---|---|
| Invasive Lobular Carcinoma (~15%) | Dyscohesive cells in single-file linear cords; signet ring cells with intracytoplasmic mucin; minimal desmoplasia | E-cadherin negative; CDH1 mutation; unusual metastatic sites (peritoneum, leptomeninges, GI tract, ovaries) | Intermediate |
| Mucinous (Colloid) Carcinoma | Clusters of cells in large extracellular lakes of mucin; soft/gelatinous | Low grade | Favorable |
| Tubular Carcinoma | Exclusively well-formed open tubules; can mimic sclerosing adenosis | Always Grade 1 | Excellent |
| Cribriform Carcinoma | Invasive nests with cribriform (sieve-like) spaces | — | Excellent |
| Papillary Carcinoma | True papillary fronds lined by tumor cells | — | Good |
HER2-Enriched Special Types
| Subtype | Morphology |
|---|---|
| Apocrine Carcinoma | Cells resemble sweat glands; enlarged round nuclei with prominent nucleoli; abundant eosinophilic/granular cytoplasm |
| Invasive Micropapillary Carcinoma | Hollow balls of cells floating in intercellular fluid; mimic papillae but lack true fibrovascular cores |
Triple-Negative (ER-/PR-/HER2-) Special Types
| Subtype | Features | Prognosis |
|---|---|---|
| Metaplastic Carcinoma | Squamous or mesenchymal differentiation (spindle, chondroid, osseous); myoepithelial gene expression | Poor (mostly) |
| Adenoid Cystic Carcinoma | Identical to salivary gland tumor; biphasic pattern | Favorable |
| Mucoepidermoid Carcinoma | "Salivary gland-like" | Favorable |
| Secretory Carcinoma | Secretory vacuoles; often in young patients | Favorable |
These rare TNBC subtypes (adenoid cystic, secretory, mucoepidermoid) are called "salivary gland-like carcinomas" - they are biologically distinct and have excellent prognosis despite being triple-negative.
Inflammatory Carcinoma (Clinical Presentation, not a histologic type)
- NOT a special histologic type - it is a clinical presentation
- Caused by extensive plugging of dermal lymphovascular spaces by carcinoma cells
- Results in: diffuse breast erythema, swelling, skin thickening, peau d'orange (skin tethered by Cooper ligaments)
- Mimics infection/mastitis → delayed diagnosis
- The name "inflammatory" is a misnomer - typically NO actual inflammation is present
- Underlying carcinoma: usually high-grade, diffusely infiltrative, no discrete palpable mass
- Very poor prognosis: 3-year survival rate only 3-10%
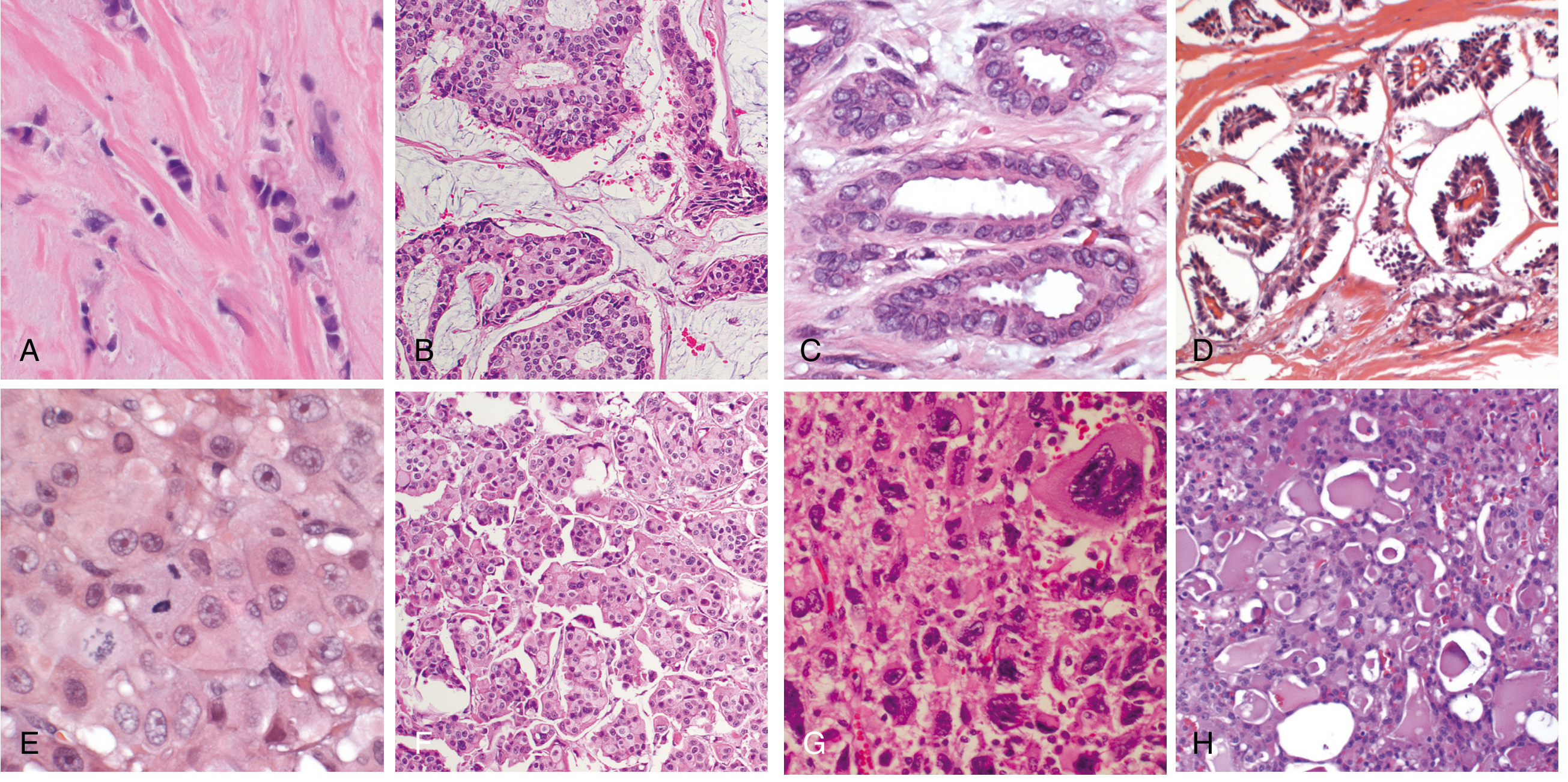
Fig. 23.22 - Robbins: Special histologic types. (A) Lobular - single-file cords. (B) Mucinous - cells in mucin lakes. (C) Tubular - open tubules. (D) Papillary. (E) Apocrine - eosinophilic granular cytoplasm. (F) Micropapillary - hollow balls. (G) Metaplastic - squamous differentiation. (H) Secretory.
PART III: MOLECULAR SUBTYPES
Based on gene expression profiling, 6 "intrinsic" subtypes are recognized, but clinically these are condensed to 3 major groups based on ER and HER2 IHC:
| Clinical Group | IHC Profile | Molecular Subtype | Frequency | Key Biology |
|---|---|---|---|---|
| Luminal | ER+, HER2- | Luminal A (low Ki67): 35-45% / Luminal B (high Ki67): 20-25% | 60-65% total | ER-driven; hormone-responsive |
| HER2 | HER2-amplified (ER+ or ER-) | HER2-enriched: 5-10% | ~20% | HER2 gene amplification; trastuzumab-sensitive |
| TNBC | ER-, PR-, HER2- | Basal-like: 15-20% | ~15% | BRCA1 silencing; genomic instability; TP53 mutation |
Additional molecular subtypes from gene expression profiling:
- Normal-like: Gene expression resembles normal breast tissue
- Claudin-low: Low expression of cell-cell junction proteins; enriched for mesenchymal/stem cell features; associated with TNBC
PART IV: CLINICAL FEATURES
Presentation by subtype:
- Luminal cancers: More often detected by mammographic screening as small masses; limited to breast
- HER2+ and TNBC: More aggressive; more likely to present as palpable masses
Signs of local advancement:
- Fixed to pectoralis muscle / chest wall (skin/muscle invasion)
- Skin dimpling or retraction (dermal invasion)
- Nipple retraction (central breast involvement)
- Peau d'orange (dermal lymphatic blockage → inflammatory carcinoma)
- Rare: presents first as axillary lymph node metastasis before breast primary is found
PART V: PROGNOSTIC FACTORS
The outcome depends on both biologic features and extent of disease at diagnosis (AJCC 8th edition combines anatomic stage + molecular group into prognostic stage groups).
| Prognostic Factor | Details |
|---|---|
| Distant metastases | Most important overall factor; cure unlikely once present |
| Lymph node status | Most important in absence of distant mets; 10-yr DFS: 70-80% (N0) → 35-40% (1-3 nodes) → 10-15% (>10 nodes) |
| Tumor size | <1 cm N0: >90% 10-yr survival; >2 cm: 77% |
| Histologic grade | Higher grade = worse prognosis |
| ER, PR, HER2 expression | Best prognosis: high ER/PR, HER2-; worst: ER-/PR-/HER2- |
| Lymphovascular invasion | Poor prognostic factor; higher local recurrence risk |
| Special histologic type | Tubular/cribriform = excellent; metaplastic (most) = poor |
| Inflammatory carcinoma | 3-yr survival 3-10% |
| Response to neoadjuvant chemo | Strong prognostic factor in TNBC and HER2+; not for luminal cancers |
| Gene expression profiling | Identifies luminal patients who do NOT need chemotherapy |
PART VI: TARGETED THERAPIES (Summary)
| Target | Treatment | Companion Assay |
|---|---|---|
| ER | Tamoxifen, aromatase inhibitors (letrozole), fulvestrant | IHC for nuclear ER |
| CDK4/6 | Palbociclib, abemaciclib, ribociclib | Ki67 index |
| HER2 | Trastuzumab, T-DM1, lapatinib | IHC + ISH for HER2 |
| BRCA1/2 (HRR defects) | PARP inhibitors (olaparib), platinum agents | BRCA1/2 sequencing |
| PI3K/AKT/mTOR | Everolimus, alpelisib | PI3K mutation testing |
| PD-L1 (TNBC) | Immune checkpoint inhibitors | PD-L1 IHC |
- Robbins, Cotran & Kumar Pathologic Basis of Disease, Chapter 23, pp. 966-984
This is a shared conversation. Sign in to Orris to start your own chat.