Metaplasia
Reading File
Finding Sources
Searching PubMed
metaplasia cellular adaptation pathology
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
I now have comprehensive content for a thorough answer. Let me compose the full response.
Metaplasia
Definition
Metaplasia is a reversible change in which one differentiated adult cell type (epithelial or mesenchymal) is replaced by another differentiated adult cell type. It is a form of cellular adaptation in which a cell type that is sensitive to a particular stress is replaced by another type better able to withstand the adverse environment.
- Robbins & Kumar Basic Pathology, p. 680
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 2049
Mechanism
Metaplasia is thought to arise through reprogramming of tissue stem cells rather than a direct phenotypic conversion of already-differentiated cells (transdifferentiation). The stem cells, under persistent stress signals, are driven to differentiate along a new pathway that is better suited to the altered microenvironment.
Types of Metaplasia
1. Epithelial Metaplasia
A. Columnar → Squamous (Most common)
The classic example is the respiratory tract in cigarette smokers. Normal ciliated columnar epithelium of the trachea and bronchi is replaced by stratified squamous epithelium, which is tougher and more resistant to the noxious chemicals in cigarette smoke.
Schematic diagram (A) and histology (B) of bronchial squamous metaplasia:
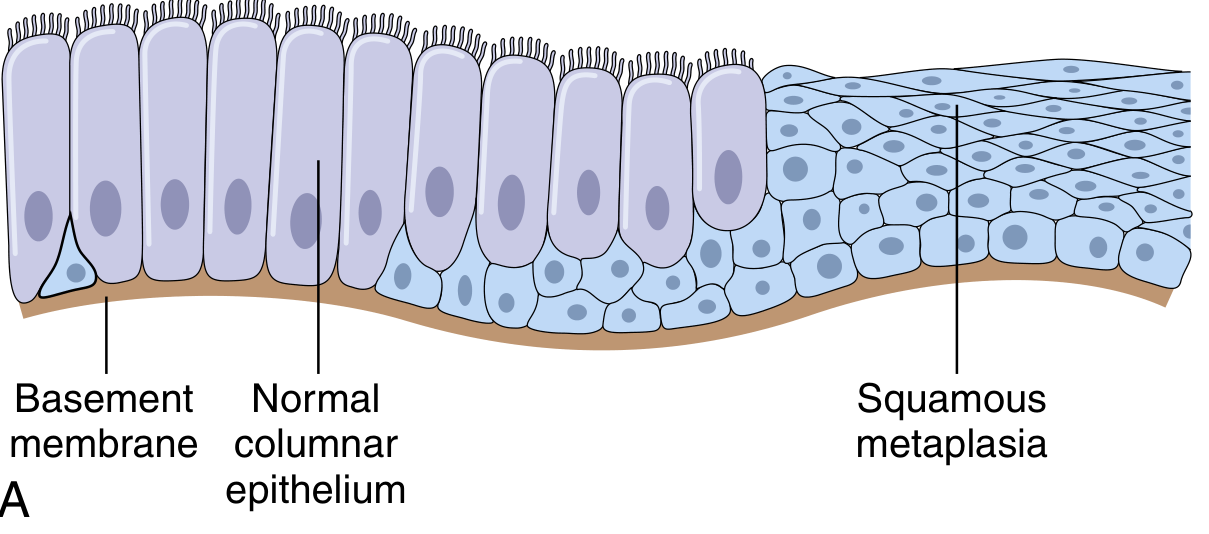
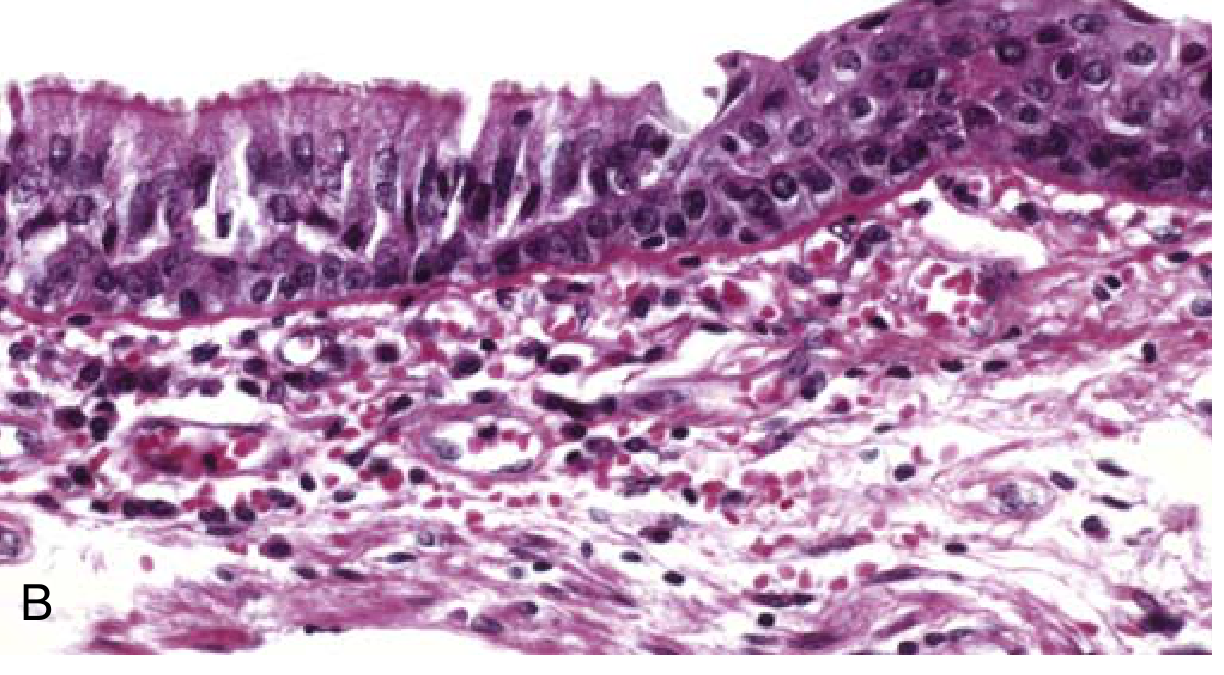
Fig. 1.23 - Robbins & Kumar Basic Pathology: Metaplasia of normal columnar (left) to squamous epithelium (right) in a bronchus.
Other causes of columnar → squamous metaplasia:
- Vitamin A (retinoic acid) deficiency - affects respiratory epithelium and the cornea (causing vision damage)
- Stones in excretory ducts of salivary glands, pancreas, or bile ducts - irritation/pressure leads to squamous metaplasia of the normally columnar secretory lining
B. Squamous → Columnar (Barrett Esophagus)
In gastroesophageal reflux disease (GERD), chronic exposure to refluxed gastric acid causes the normal stratified squamous epithelium of the lower esophagus to be replaced by intestinal-like columnar epithelium. This is called Barrett esophagus. The cancers that arise in these areas are typically gland-forming adenocarcinomas.
2. Connective Tissue (Mesenchymal) Metaplasia
This refers to formation of cartilage, bone, or adipose cells in tissues that do not normally contain them. Examples:
- Myositis ossificans - bone formation in muscle after intramuscular hemorrhage
- Bone formation in soft tissues at foci of injury
Unlike epithelial metaplasia, connective tissue metaplasia is less clearly an adaptive response and more often a result of tissue injury. It is also not associated with the same degree of malignant potential.
The Double-Edged Sword
Metaplasia represents an adaptive response, but it comes at a cost:
| Benefit | Cost |
|---|---|
| Greater durability against the offending stress | Loss of specialized functions (e.g., mucus secretion, ciliary clearance in respiratory tract) |
| Cell survival under adverse conditions | Predisposition to malignant transformation if the stimulus persists |
Malignant Potential
The persistent stimulus that drives metaplasia can also, over time, initiate malignant transformation of the metaplastic epithelium:
| Metaplastic Change | Associated Cancer |
|---|---|
| Squamous metaplasia of respiratory epithelium | Squamous cell carcinoma of the lung |
| Intestinal metaplasia of stomach | Gastric adenocarcinoma |
| Barrett esophagus (squamous → columnar) | Esophageal adenocarcinoma |
Key Points to Remember
- Metaplasia is reversible - if the stimulus is removed, cells can revert (though not always completely).
- It involves reprogramming of stem cells, not transdifferentiation of mature cells.
- It is fundamentally different from dysplasia (disordered growth with atypical cells) - metaplastic cells are normal cells of a different type.
- It is distinct from hyperplasia (increase in cell number) and hypertrophy (increase in cell size).
- Metaplasia itself is not cancer, but it is a premalignant state when the driving stimulus persists.
Sources: Robbins & Kumar Basic Pathology, pp. 680-698; Robbins, Cotran & Kumar Pathologic Basis of Disease, pp. 2049-2067
This is a shared conversation. Sign in to Orris to start your own chat.