Ippa physical examination for lungs ( respiratory system)
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Searching Images
chest percussion auscultation physical examination lung
Reading File
Loading Image
I now have comprehensive content. Let me compile the full IPPA respiratory examination answer.
IPPA Physical Examination of the Respiratory System (Lungs)
IPPA = Inspection → Palpation → Percussion → Auscultation
Source: Murray & Nadel's Textbook of Respiratory Medicine
Overview
Physical examination of the chest uses these four classic techniques in sequence. Optimal conditions require privacy, warmth, good lighting, and a quiet atmosphere. The patient is ideally seated with sufficient clothing removed to expose the entire thorax.
1. INSPECTION 👁️
The examination begins the moment the clinician first sees the patient.
What to Observe:
| Feature | Normal / Abnormal Findings |
|---|---|
| General appearance | Respiratory distress, cyanosis, accessory muscle use |
| Chest shape | Barrel chest (COPD), pectus excavatum, pectus carinatum, kyphoscoliosis, ankylosing spondylitis |
| Symmetry | Unilateral lag suggests consolidation, pleural effusion, pneumothorax |
| Scars/deformities | Previous surgeries, trauma |
| Breathing pattern | Rate, rhythm, depth (see below) |
| Accessory muscles | SCM, scalenes engaged → airway obstruction |
Classic Breathing Patterns:
- Eupnea — normal breathing
- Tachypnea — rapid, shallow (fever, anxiety, hypoxia)
- Bradypnea — slow (CNS depression, opioids)
- Kussmaul — deep, rapid (metabolic acidosis)
- Cheyne-Stokes — cyclical waxing/waning (heart failure, CNS disease)
- Biot's — irregular with apneic episodes (meningitis, brainstem lesion)
Associated Observations:
- Cyanosis — central (tongue) vs. peripheral
- Clubbing of fingers — chronic hypoxia (bronchiectasis, lung cancer, fibrosis)
- JVP elevation — cor pulmonale, tension pneumothorax
- Odors — tobacco stains, ketones (diabetic ketoacidosis), foul smell (anaerobic abscess), Pseudomonas (sweet odor)
2. PALPATION ✋
Tracheal Position
- Palpate trachea at the suprasternal notch
- Midline = normal
- Deviated toward lesion = collapse/fibrosis/atelectasis
- Deviated away from lesion = large effusion, tension pneumothorax
Chest Wall Assessment
- Feel for point tenderness (rib fracture, pleurisy)
- Subcutaneous emphysema — crepitus like Rice Krispies under skin (pneumothorax, trauma)
- Fluctuant areas — empyema necessitans
- Cervical rib / bony abnormalities
Chest Expansion
Place both hands symmetrically over opposite hemithoraces (anteriorly at costal margins, posteriorly at lower thorax). Ask patient to breathe deeply.
- Equal expansion = normal
- Reduced on one side = consolidation, collapse, effusion, pneumothorax on that side
Vocal Fremitus (Tactile Fremitus)
Ask patient to say "ninety-nine" or "one-two-three" while palpating with ulnar border/palm moving systematically top to bottom bilaterally:
| Finding | Cause |
|---|---|
| Increased fremitus | Consolidation (pneumonia) — better sound transmission |
| Decreased fremitus | Pleural effusion, pneumothorax, COPD — impaired transmission |
| Absent fremitus | Blocked bronchus, large effusion |
Cardiac Palpation
- Apical impulse, heaves, thrills
- In severe COPD: cardiac movements better felt at the subxiphoid (due to hyperinflation)
3. PERCUSSION 🎵
Technique
The pleximeter (middle finger of non-dominant hand) is placed flat on the chest wall; the plexor (middle finger of dominant hand) strikes it with a sharp, free wrist stroke. Move systematically comparing left and right sides at each level.
Percussion Notes:
| Sound | Quality | Cause |
|---|---|---|
| Resonant | Hollow, low-pitched | Normal air-containing lung |
| Hyperresonant | Booming, very low-pitched | Emphysema, pneumothorax |
| Tympanitic | Drum-like | Tension pneumothorax, gas-filled bowel |
| Dull | Short duration, higher pitch, low intensity | Consolidation (pneumonia), pleural effusion |
| Flat | Non-resonant, high-pitched | Massive effusion, solid tissue (like percussing liver) |
Clinical Pearls:
- Large pleural effusion: 3 zones from top to bottom — resonant → dull → flat
- Pneumothorax: hyperresonant → tympanitic if tension
- Consolidation/pneumonia: dull
4. AUSCULTATION 🔊
Use the diaphragm for higher-pitched sounds (breath sounds, normal); use the bell lightly for lower-pitched sounds. Auscultate anterior, lateral, and posterior chest systematically, comparing sides.
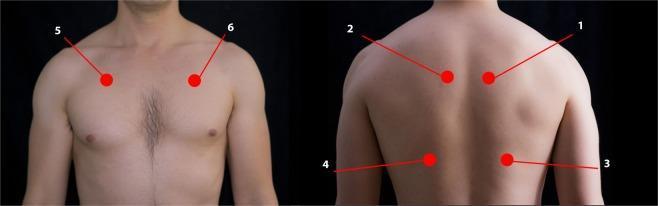
Auscultation positions — anterior, posterior (arms crossed to protract scapulae), and lateral (hands behind head):
A. Normal Breath Sounds
| Type | Location | Character |
|---|---|---|
| Normal (vesicular) | Peripheral lung fields | Soft, low-pitched; inspiration > expiration (3:1); no gap |
| Bronchovesicular | Around main bronchi (1st/2nd ICS, between scapulae) | Medium pitch; inspiration = expiration |
| Bronchial (tracheal) | Over trachea/manubrium | Loud, high-pitched, hollow; expiration > inspiration; gap between phases |
Note: "Vesicular" is a historical misnomer — normal breath sounds arise from turbulent airflow in lobar/segmental bronchi, not alveoli.
B. Adventitious (Abnormal) Sounds
(Standardized by American Thoracic Society)
| Sound | Character | Timing | Significance |
|---|---|---|---|
| Fine crackles | Soft, high-pitched, short discontinuous pops | Mid-to-late inspiratory | Fibrosis, pulmonary edema, early pneumonia — opening of collapsed distal airways |
| Coarse crackles | Loud, low-pitched, longer discontinuous | Early inspiratory or expiratory | Secretions in distal airways; may change after coughing |
| Wheeze | Continuous, high-pitched (≥400 Hz), hissing, >250 ms | Predominantly expiratory | Airway narrowing — asthma, COPD (diffuse); focal lesion (unilateral) |
| Rhonchi | Continuous, low-pitched (<200 Hz), snoring, >250 ms | Expiratory | Secretions in large airways; often clear with cough |
| Stridor | High-pitched, inspiratory, loudest over neck | Inspiratory | Extrathoracic/upper airway obstruction — urgent (anaphylaxis, epiglottitis, foreign body) |
| Bronchial sounds in periphery | Like tracheal sounds heard peripherally | Both phases | Consolidation, atelectasis — airless alveoli around patent bronchus |
| Pleural rub | Creaking, leathery, grating | Both phases | Pleuritis — inflamed pleural surfaces rubbing |
C. Voice-Transmitted Sounds (Vocal Resonance)
Ask patient to say "ninety-nine" while auscultating:
| Test | Normal | Abnormal | Cause |
|---|---|---|---|
| Bronchophony | Muffled "ninety-nine" | Clearly heard "99" | Consolidation |
| Whispered pectoriloquy | Inaudible whisper | Clearly heard whispered "1-2-3" | Consolidation |
| Egophony | Normal voice | "ee" sounds like "ay" (nasal, bleating) | Consolidation or effusion margin |
Summary: Findings by Condition
| Condition | Inspection | Palpation | Percussion | Auscultation |
|---|---|---|---|---|
| Consolidation (Pneumonia) | Reduced expansion | ↑ fremitus, lag | Dull | Bronchial breathing, crackles, ↑ vocal resonance |
| Pleural Effusion | Reduced expansion | ↓ fremitus, lag | Stony dull | Absent/reduced breath sounds; egophony at upper border |
| Pneumothorax | Reduced expansion | ↓/absent fremitus, lag, tracheal deviation away | Hyperresonant | Absent breath sounds |
| COPD/Emphysema | Barrel chest, ↑RR | ↓ fremitus | Hyperresonant | ↓ breath sounds, prolonged expiration, wheeze |
| Asthma (acute) | Accessory muscles, tachypnea | ↓ expansion | Resonant/hyperresonant | Diffuse wheeze, ↓ breath sounds |
| Fibrosis | Clubbing, tachypnea | ↓ expansion | Normal/dull | Fine "Velcro" crackles (bibasal) |
| Atelectasis/Collapse | Lag, tracheal deviation toward | ↓ fremitus, lag | Dull | Bronchial/absent breath sounds |
Murray & Nadel's Textbook of Respiratory Medicine, Chapter 18 — "Examination of the Chest"
This is a shared conversation. Sign in to Orris to start your own chat.