
17792596066533778656010458551232.jpg
Explain m6pl
Reading File
Finding Sources
Searching the Web
TSH 133 T4 low T3 normal hypothyroidism interpretation management
Reading File
Here is a full explanation of the thyroid function panel (TFT) in the report — what each result means and what it points to clinically.
Thyroid Function Test (TFT) — Report Breakdown
| Test | Your Result | Reference Range | Status |
|---|---|---|---|
| Serum T3 | 0.93 ng/mL | 0.87 – 1.78 | ✅ Normal |
| Serum T4 | 4.96 µg/dL | 6.09 – 12.23 | 🔴 LOW |
| Serum TSH | 133.29 µIU/mL | 0.27 – 4.20 | 🔴 CRITICALLY HIGH |
What Each Hormone Does
TSH (Thyroid-Stimulating Hormone)
- Made by the pituitary gland to signal the thyroid to produce T3/T4.
- When the thyroid is underactive, the pituitary pumps out more and more TSH trying to compensate.
- Normal: 0.27–4.20 µIU/mL. A TSH of 133.29 is roughly 30–50× above the upper limit of normal — this is severely elevated.
T4 (Thyroxine)
- The main hormone secreted by the thyroid gland; it is a prohormone that gets converted to the active T3.
- Your result of 4.96 µg/dL is below the lower limit (6.09) — the thyroid is not producing enough.
T3 (Triiodothyronine)
- The biologically active thyroid hormone.
- Yours is 0.93 ng/mL — within range, but this can still occur in early or moderate hypothyroidism because the body compensates by converting more of the available T4 → T3, keeping T3 relatively normal even as T4 falls.
Clinical Interpretation: Severe Primary Hypothyroidism
The pattern — very high TSH + low T4 + relatively preserved T3 — is the textbook picture of primary hypothyroidism (the thyroid gland itself is failing, not the pituitary or hypothalamus).
Most likely causes include:
- Hashimoto's thyroiditis (autoimmune — commonest cause worldwide)
- Iodine deficiency
- Post-thyroiditis (e.g., after viral or subacute thyroiditis)
- Iatrogenic (after radioiodine therapy or thyroid surgery)
- Insufficiently treated or untreated hypothyroidism on replacement therapy
The report note on the lab slip itself confirms this: "TSH increased in primary untreated hypothyroidism, Hashimoto's thyroiditis, patients receiving insufficient thyroid hormone replacement therapy."
Why Is T3 Still Normal?
Even when the thyroid starts to fail and T4 drops, the body preferentially converts T4 → T3 in peripheral tissues (liver, kidney, muscle). T3 is spared until hypothyroidism becomes severe. This is why T3 is the last to fall and is not a reliable early marker of hypothyroidism.
What Should Happen Next?
- Clinical assessment — symptoms of hypothyroidism: fatigue, weight gain, cold intolerance, constipation, dry skin, bradycardia, puffy face (myxedema), slow reflexes.
- Anti-TPO antibodies (thyroid peroxidase) and anti-thyroglobulin antibodies — to confirm Hashimoto's thyroiditis.
- Thyroid ultrasound — to assess gland size and echogenicity.
- Start levothyroxine (LT4) therapy — dose is titrated to bring TSH into the normal range (typically 0.5–2.5 µIU/mL). A TSH this high warrants prompt treatment.
- Recheck TFTs in 6–8 weeks after starting treatment.
⚠️ This report should be reviewed urgently by an endocrinologist or physician. A TSH of 133 indicates severe, likely long-standing hypothyroidism that requires prompt medical management.
Find clinical images of thyroid pathology related to hypothyroidism
Reading File
Finding Sources
Searching Images
hypothyroidism clinical features myxedema thyroid pathology
Finding Sources
Finding Sources
Searching Images
Hashimoto thyroiditis histology microscopy lymphocytic infiltration
Reading File
Reading File
Searching Images
goiter enlarged thyroid gland clinical photo neck swelling
Reading File
Searching Images
thyroid ultrasound Hashimoto hypothyroidism hypoechoic heterogeneous
Here is a comprehensive visual gallery of thyroid pathology related to hypothyroidism, organized by category:
Clinical Images: Hypothyroidism & Thyroid Pathology
1. Myxedematous Facies — Adult (Severe Hypothyroidism)

Features visible: Periorbital non-pitting edema, diffuse facial puffiness, pale/thickened waxy skin, dull apathetic expression, loss of the outer third of the eyebrow (Hertoghe's sign / madarosis) — a hallmark sign of hypothyroidism.
2. Myxedematous Facies — Moon Face Appearance (Uncontrolled Hypothyroidism)

Features visible: Rounded facial contour, bilateral periorbital puffiness, submental/cervical soft tissue fullness, diffuse skin thickening from mucopolysaccharide deposition in dermis. This appearance is caused by accumulation of glycosaminoglycans in subcutaneous tissue.
3. Myxedema Coma — Patient in Hospital Setting

Features visible: Severe facial puffiness, thickened pale skin, ECG monitoring (bradycardia is common in myxedema coma). This represents an endocrine emergency with hypothermia, altered consciousness, and cardiovascular compromise.
4. Congenital Hypothyroidism (Cretinism)
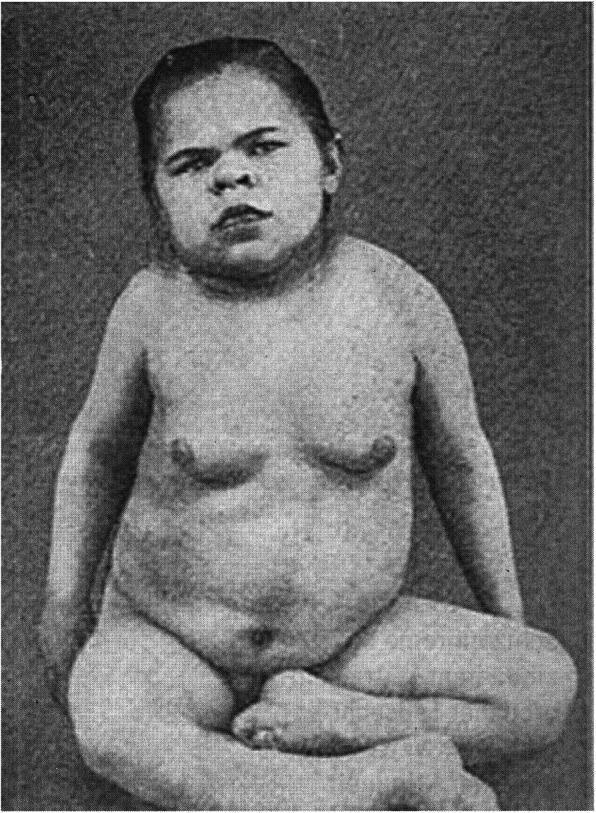
Features visible: Periorbital puffiness, depressed nasal bridge, macroglossia, protuberant abdomen, generalized subcutaneous swelling. If untreated, leads to intellectual disability and growth retardation (cretinism).
5. Before & After Levothyroxine Treatment — Congenital Hypothyroidism

Panel a/b (before treatment): Severe abdominal distension, umbilical hernia, macroglossia, sparse hair, generalized myxedema. Panel c/d (6 months after levothyroxine): Complete resolution of distension and achievement of developmental milestones — illustrates the dramatic efficacy of thyroid replacement therapy.
6. Goiter — Diffuse Thyroid Enlargement (Classic in Hashimoto)

Hashimoto thyroiditis classically presents as a painless, symmetrically enlarged goiter. Over time, gland destruction leads to progressive hypothyroidism (high TSH, low T4) — exactly the pattern seen in the lab report above.
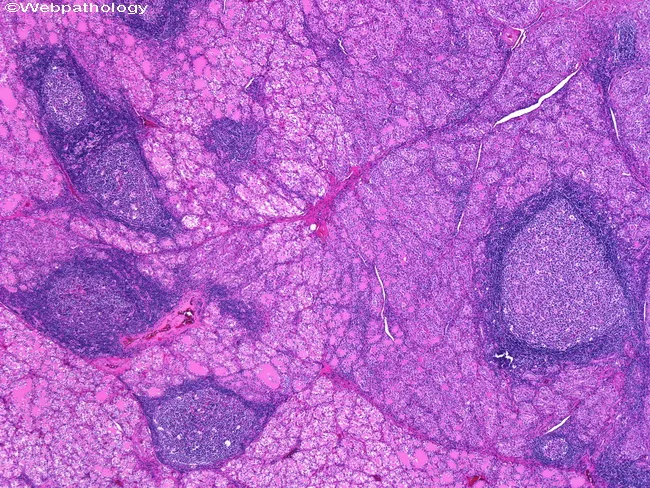
7. Hashimoto Thyroiditis — Histology (H&E, Low Power)
Microscopic features: Dense lymphocytic infiltration with well-formed germinal centers, small atrophic thyroid follicles, and Hürthle cell (oncocytic) metaplasia — follicular epithelial cells with abundant pink cytoplasm. This is the definitive pathological appearance of Hashimoto disease. (Robbins Pathologic Basis of Disease)
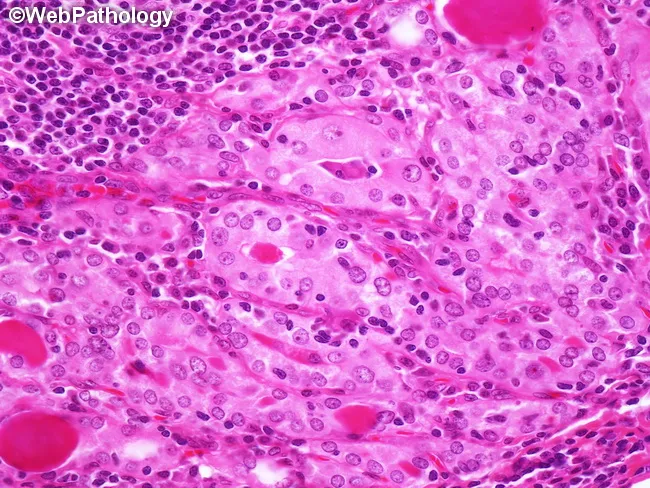
8. Hashimoto Thyroiditis — Histology (H&E, Higher Detail)
Key features: Mononuclear infiltrate (lymphocytes + plasma cells), disrupted follicular architecture, Hürthle cell change, germinal center formation reflecting active B-cell autoimmune response.
9. Thyroid Ultrasound — End-Stage Hashimoto (Atrophic)

Sonographic findings: Markedly reduced thyroid size (atrophy), diffusely hypoechoic and heterogeneous parenchyma compared to surrounding strap muscles, irregular borders — characteristic of chronic autoimmune hypothyroidism. This is the typical ultrasound appearance in patients with the kind of severe TSH elevation seen in the report above.
10. Thyroid Ultrasound — Hashimoto with Nodular Goiter + Color Doppler
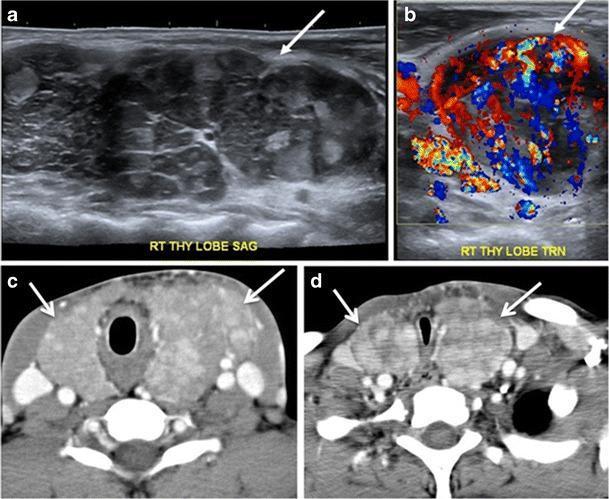
Composite imaging (19-year-old male): (a) Sagittal US — enlarged hypoechoic right lobe; (b) Color Doppler — marked hypervascularity ("thyroid inferno"); (c/d) CT — diffusely enlarged heterogeneous gland with tracheal compression. Shows how advanced Hashimoto can cause compressive symptoms requiring surgical evaluation.
Summary of Key Pathological Findings in Hypothyroidism
| Category | Key Finding |
|---|---|
| Clinical (adult) | Periorbital edema, loss of outer eyebrows, doughy skin, bradycardia |
| Clinical (pediatric) | Macroglossia, protuberant abdomen, developmental delay, umbilical hernia |
| Emergency | Myxedema coma — hypothermia, altered consciousness |
| Macroscopic | Diffuse symmetric painless goiter (Hashimoto) |
| Microscopy | Lymphocytic infiltrate, germinal centers, Hürthle cell metaplasia, atrophic follicles |
| Ultrasound | Hypoechoic, heterogeneous, atrophic gland; hypervascularity in active phase |
This is a shared conversation. Sign in to Orris to start your own chat.