What is ductus venosus
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
ductus venosus fetal circulation diagram
Here is a comprehensive overview of the ductus venosus:
Ductus Venosus
Definition & Anatomy
The ductus venosus is a fetal vascular shunt that directly connects the umbilical vein–portal sinus confluence to the inferior vena cava (IVC), effectively bypassing the liver. Unlike the umbilical and portal veins, the ductus venosus has no direct branches to the liver — it is a dedicated bypass channel. Umbilical venous blood can enter it directly, but portal venous blood can only reach it through the portal sinus.
- Creasy & Resnik's Maternal-Fetal Medicine, p. 4025
- The Developing Human: Clinically Oriented Embryology, p. 4800
Role in Fetal Circulation
The fetal circulation has four unique pathways — placenta, ductus venosus, foramen ovale, and ductus arteriosus — to facilitate gas and nutrient exchange, since the placenta substitutes for the lungs, GI tract, liver, and kidneys.
How it works:
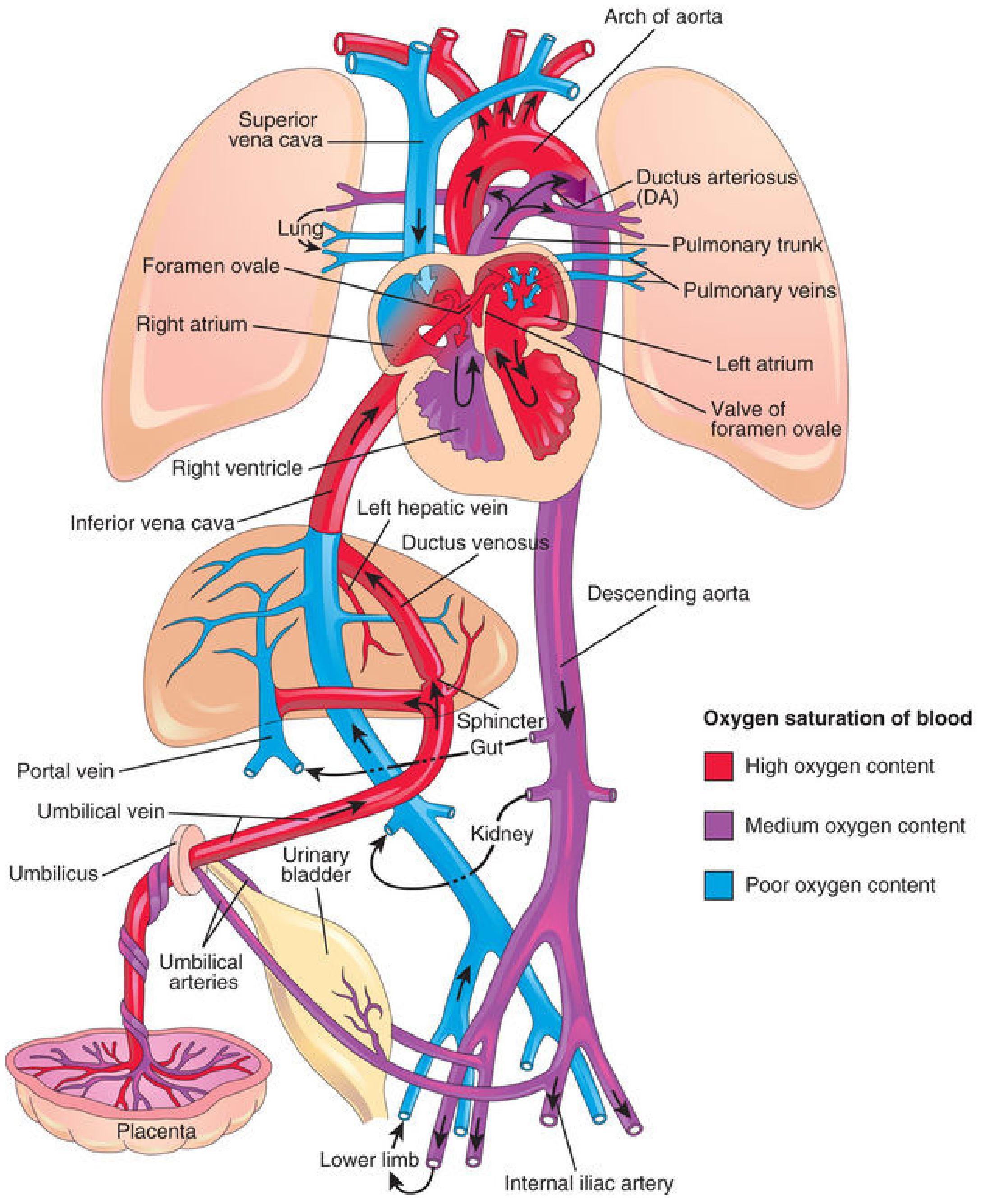
- Oxygenated blood (~O₂ saturation 80–85%) returns from the placenta via the umbilical vein.
- ~50% of umbilical blood flow passes through the ductus venosus directly into the IVC, bypassing the largely non-functional liver.
- The remaining ~50% enters the hepatic-portal system and perfuses the liver.
- Blood from the ductus venosus merges with IVC blood (~19% of combined cardiac output, CCO) draining the lower limbs, kidneys, and splanchnic organs — so ~69% of CCO enters the right atrium.
- The well-oxygenated ductus venosus stream occupies the dorsal and leftward portion of the IVC and preferentially streams through the foramen ovale into the left atrium → left ventricle → ascending aorta, ensuring the brain and myocardium receive the most oxygenated blood.
- Medical Physiology (Boron & Boulpaep), p. 182
- Creasy & Resnik's Maternal-Fetal Medicine, p. 4031
Physiologic Significance
- The ductus venosus is the only fetal vessel that can actively dilate in response to hypoxemia, providing a regulatory mechanism for oxygen-sensitive flow centralization.
- In healthy fetuses, it regulates distribution of oxygen and placental nutrients by restricting centralization of flow.
- High-velocity flow through the ductus venosus makes it easily identifiable on Doppler ultrasound.
Doppler Assessment (Clinical Use)
The ductus venosus Doppler waveform is used as a marker of fetal cardiovascular function and oxygen status:
- Normal: triphasic, pulsatile high-velocity waveform with forward flow throughout.
- Absent or reversed flow during atrial contraction (the "a-wave") signals increased cardiac afterload and fetal compromise.
- Abnormal ductus venosus pulsation is also a marker in first-trimester Down syndrome screening, with detection rates of 65–75%.
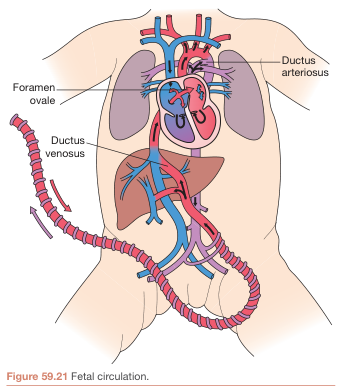
Fetal circulation showing the ductus venosus bypassing the liver to channel oxygenated umbilical blood to the IVC and heart (Bailey & Love's Short Practice of Surgery, p. 985)
Closure After Birth
| Timeframe | Event |
|---|---|
| At birth | Blood flow through the umbilical vein ceases; ductus venosus pressure and lumen diameter decrease |
| 1–3 hours | Smooth muscle in the ductus venosus wall contracts strongly |
| 2–18 days | Functional closure complete; portal venous pressure rises from ~0 to 6–10 mmHg, forcing blood through liver sinusoids |
| Weeks–months | Anatomic closure → becomes the ligamentum venosum, a fibrous remnant that passes through the liver from the left branch of the portal vein to the IVC |
The mechanisms underlying closure of the ductus venosus remain incompletely understood (unlike the ductus arteriosus, where prostaglandin withdrawal is well established).
- Guyton & Hall Textbook of Medical Physiology, p. 1725
- Medical Physiology (Boron & Boulpaep), p. 301
- The Developing Human, p. 4800
Summary Table
| Feature | Detail |
|---|---|
| Location | Connects umbilical vein/portal sinus to IVC |
| Purpose | Bypass liver; deliver oxygenated blood to heart |
| % of umbilical flow | ~50% passes through it |
| Postnatal remnant | Ligamentum venosum |
| Closure timing | Functionally: 1–3 hrs to 2–18 days; Anatomically: weeks |
| Clinical tool | Doppler waveform for fetal well-being and aneuploidy screening |
In fetus ...there is a structure called ductus arteriosus ... RA - Rv - pulmonary artery - ductus arteriosus - aorta ...thn it means it doesnt go to lungs ???? Or does it go ??? There is also foramen ovale ...then what is tge purpose of foramen ovale when there is ductus arteriouss
Reading File
Finding Sources
Reading File
Loading Image
This is a brilliant question. Your instinct is right — both shunts exist, and they actually serve different blood streams. Here's the full picture:
The Core Answer: The Right Atrium Receives TWO Different Streams
The key insight is that not all blood in the right atrium is the same, and the two shunts handle these two different streams.
What Enters the Right Atrium?
Two separate streams pour into the right atrium simultaneously:
| Stream | Source | O₂ Saturation | Route |
|---|---|---|---|
| Stream 1 | IVC (carrying ductus venosus blood — well-oxygenated from placenta) | ~70% | → Foramen ovale → Left atrium |
| Stream 2 | SVC (deoxygenated blood from head/arms) + lower IVC (from body) | ~29–55% | → Right ventricle → Pulmonary artery → Ductus arteriosus → Aorta |
The two streams do not mix in the right atrium — they stream separately because of the anatomy of the IVC and the crista dividens (a ridge of tissue that physically splits them).
So Does ANY Blood Go to the Lungs?
Yes — but only a tiny amount (~10% of right ventricular output).
- The ductus arteriosus is so large and low-resistance that it accepts ~90% of right ventricular output and dumps it into the descending aorta.
- Only ~10% trickles into the pulmonary vessels — just enough to nourish the developing lung tissue, not for gas exchange (because the lungs aren't doing gas exchange yet).
- The lungs are fluid-filled and have high vascular resistance in utero, which is why blood preferentially avoids them.
So Why Do You Need BOTH Shunts? What's the Difference?
This is your real question. Here's the logic:
Foramen Ovale — Shortcut BEFORE the right ventricle
- The well-oxygenated IVC stream enters the RA and immediately crosses to the left atrium, skipping the right ventricle and pulmonary artery entirely.
- This blood → Left ventricle → Ascending aorta → Brain and heart (coronaries)
- Purpose: Deliver the best, most oxygenated blood directly to the most oxygen-sensitive organs (brain and heart)
Ductus Arteriosus — Shortcut AFTER the right ventricle
- The deoxygenated SVC stream goes: RA → Right ventricle → Pulmonary artery → Ductus arteriosus → Descending aorta → Lower body and back to placenta
- This blood supplies the lower body and then returns to the placenta via umbilical arteries to get re-oxygenated
- Purpose: Bypass the non-functional, high-resistance lungs
They handle two different blood streams going in two different directions.
The Complete Fetal Flow Map
Placenta (oxygenated)
↓
Umbilical vein
↓
Ductus venosus → IVC
↓
RIGHT ATRIUM ─── splits here ───────────────────────┐
│ │
(Well-oxygenated IVC stream) (Deoxygenated SVC stream)
↓ ↓
FORAMEN OVALE Right Ventricle
↓ ↓
Left Atrium Pulmonary Artery
↓ ↙ ↘
Left Ventricle 10% to lungs 90% via DUCTUS ARTERIOSUS
↓ (nourishment) ↓
Ascending Aorta Descending Aorta
↓ ↓
BRAIN + HEART ✓ Lower body → Umbilical arteries
(best blood goes here) → Placenta (re-oxygenate)
Summary in One Line
The foramen ovale diverts the best blood to the brain and heart before it reaches the lungs. The ductus arteriosus diverts the remaining blood away from the lungs after it's already been through the right ventricle. They are complementary, not redundant.
- Medical Physiology (Boron & Boulpaep), pp. 182–192
- The Developing Human: Clinically Oriented Embryology, pp. 4691–4716
This is a shared conversation. Sign in to Orris to start your own chat.