What is neoplasm?
Reading File
Finding Sources
Searching the Web
neoplasm definition classification pathology
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have comprehensive textbook content. Let me compile the full answer.
Neoplasm
Definition
Neoplasia means "new growth." A neoplasm is defined as a disorder of cell growth triggered by acquired (or, less commonly, inherited) mutations affecting a single cell and its clonal progeny. These mutations alter genes regulating fundamental cellular processes - growth, survival, and senescence - giving neoplastic cells a growth advantage, resulting in excessive proliferation that is independent of normal physiologic growth signals and controls.
The classic definition by Sir Rupert Willis (1952) states:
"A neoplasm is an abnormal mass of tissue, the growth of which exceeds and is uncoordinated with that of the normal tissues, and persists in the same excessive manner after cessation of the stimuli which evoked the change."
The word tumor (originally meaning any swelling) is now used as a synonym for neoplasm. The study of tumors is called oncology (Greek oncos = tumor).
Structure of a Neoplasm
All tumors are composed of two components:
- Parenchyma - the neoplastic cells themselves. The classification and biologic behavior of a tumor are based primarily on this component.
- Reactive stroma - supportive connective tissue, blood vessels, and immune cells. Growth and spread are critically dependent on the stroma (it supplies the blood supply).
- Some tumors have scant connective tissue and are soft/fleshy.
- Others stimulate abundant collagen formation (called desmoplasia), making them stony hard (e.g., some breast cancers, called scirrhous tumors).
Classification: Benign vs. Malignant
| Feature | Benign | Malignant |
|---|---|---|
| Local invasion | No - stays localized | Yes - invades adjacent tissues |
| Metastasis | No | Yes (hallmark feature) |
| Growth rate | Slow | Often rapid |
| Differentiation | Well-differentiated, resembles tissue of origin | Variable; may be poorly differentiated |
| Nuclear features | Normal | Pleomorphism, hyperchromasia, abnormal mitoses |
| Effect on patient | Usually survives; location-dependent exceptions | Often fatal if untreated |
Benign Tumors
Remain localized and are generally curable by surgical removal. Named with the suffix "-oma" attached to the cell/tissue of origin (e.g., fibroma, chondroma, adenoma, papilloma).
Malignant Tumors ("Cancer")
Can invade and destroy adjacent structures and metastasize (spread to distant sites via lymphatics, blood, or body cavities). Named based on origin:
- Carcinomas - from epithelial cells (e.g., adenocarcinoma, squamous cell carcinoma)
- Sarcomas - from mesenchymal/solid connective tissues (e.g., fibrosarcoma, chondrosarcoma)
- Leukemias/Lymphomas - from blood-forming cells and lymphocytes
Key Molecular Concepts
Cancer is fundamentally a genetic disorder caused by DNA mutations:
- Mutations may be from mutagen exposure, spontaneous replication errors, or inheritance.
- Epigenetic changes (altered DNA methylation, histone modification) also play a role.
- Genetic alterations are heritable (passed to daughter cells), so cells with growth advantages outcompete neighbors - a process of Darwinian selection / clonal evolution.
- Individual tumors begin as clonal (progeny of a single mutated cell).
Special Types
- Mixed tumors - contain more than one cell lineage (e.g., pleomorphic adenoma of the salivary gland, with both epithelial and myxoid/cartilaginous components).
- Teratoma - arises from totipotential germ cells; contains cells from more than one germ layer (ectoderm, mesoderm, endoderm), potentially forming bone, hair, teeth, nerve tissue, etc.
- Undifferentiated malignant neoplasm - ~2% of cancers; cells of unknown origin.
Precursor / Pre-neoplastic Changes
Before frank neoplasia, cells often show abnormal growth patterns:
- Metaplasia - replacement of one cell type by another
- Dysplasia - disordered but not yet autonomous growth
- These can progress to neoplasia with further mutations.
Sources: Robbins, Cotran & Kumar - Pathologic Basis of Disease, Nomenclature section; Robbins & Kumar Basic Pathology (Robbins Pathology)
Define tumor and classify them based on their nature.
Finding Sources
Searching the Web
tumor classification benign malignant borderline pathology Robbins
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the material needed for a complete, well-illustrated answer. Here it is:
Tumor: Definition and Classification by Nature
Definition
A tumor (from Latin tumor = swelling) originally meant any swelling, but in modern medicine the term is equated with neoplasm - an abnormal mass of tissue resulting from uncontrolled, autonomous cell proliferation. Three features are used to distinguish tumor types:
- Differentiation and anaplasia
- Local invasion
- Metastasis
Growth rate also offers a clue, though it is not a reliable sole discriminator.
Classification Based on Nature
Tumors are classified into three broad categories based on their biologic behavior:
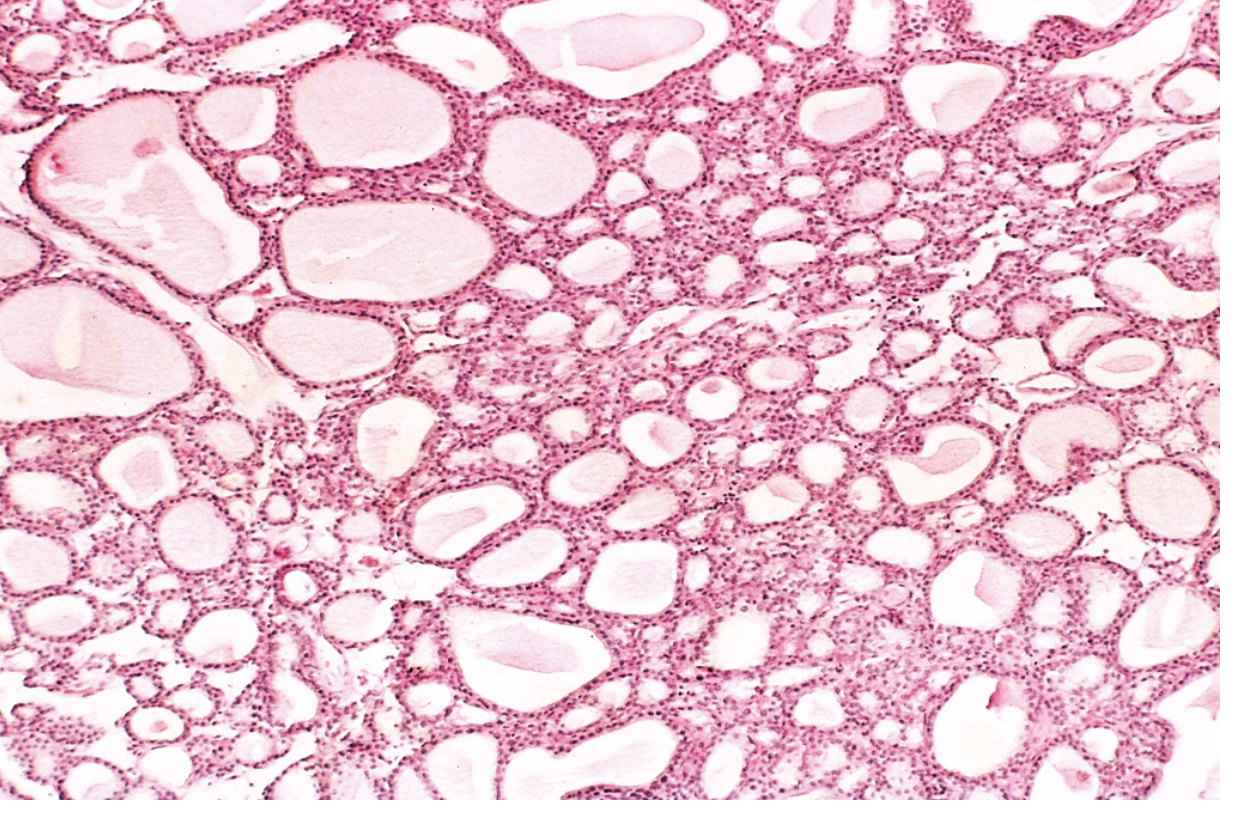
1. Benign Tumors
Benign tumors remain localized at their site of origin, do not invade surrounding tissue, and do not metastasize. They are generally curable by surgical excision.
Key features:
- Well-differentiated - cells closely resemble their normal tissue of origin, both morphologically and functionally
- Slow growth - mitoses are rare and of normal configuration
- Encapsulated - usually surrounded by a fibrous capsule, clearly demarcating them from surrounding tissue
- Non-invasive - pushing borders, not infiltrating
- No metastasis
- Usually not fatal - exceptions occur when located in critical areas (e.g., a benign brain tumor can still be life-threatening due to mass effect)
Histologic example:
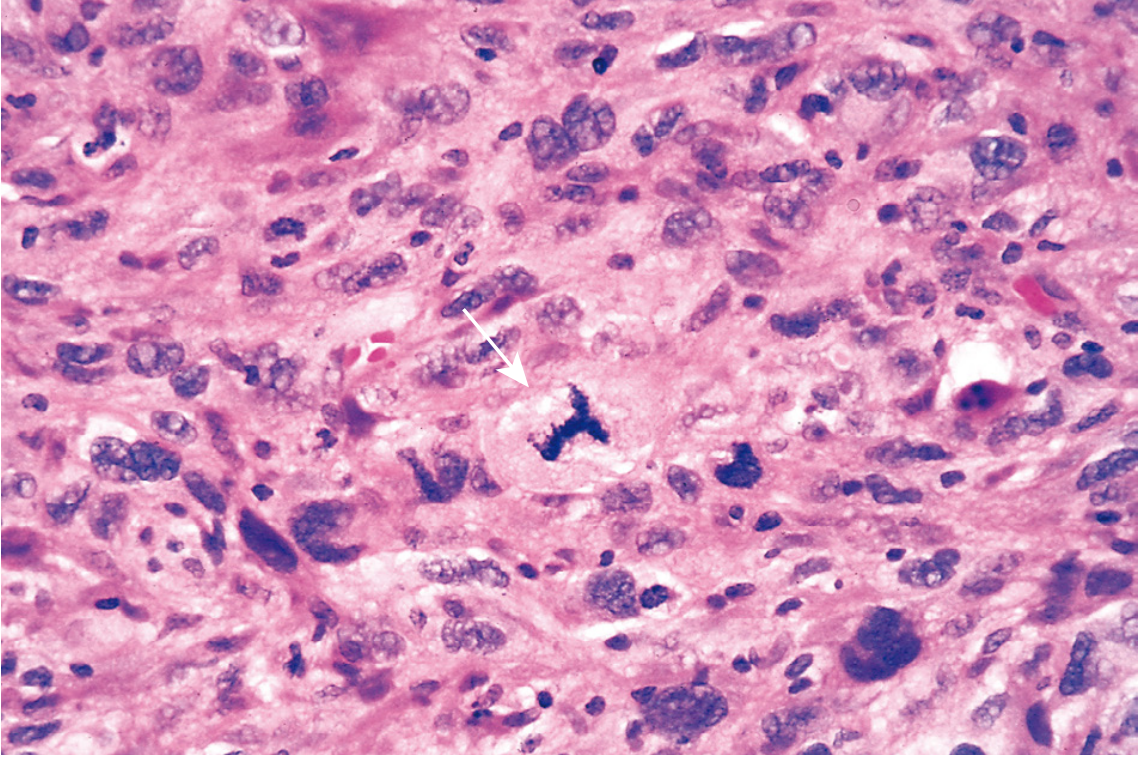
2. Malignant Tumors (Cancer)
Malignant tumors can invade adjacent structures and spread to distant sites (metastasize). They are collectively referred to as "cancers," derived from the Latin word for crab - reflecting their tendency to adhere to and grasp surrounding tissue.
Key features:
- Variable differentiation - from well-differentiated to poorly differentiated (anaplastic)
- Anaplasia - loss of differentiation; reliable indicator of malignancy. Features include:
- Pleomorphism - variation in cell size and shape
- Abnormal nuclear morphology - large, hyperchromatic nuclei; increased nuclear:cytoplasm ratio (approaches 1:1 vs normal 1:4 to 1:6); irregular nuclear shape
- Abnormal mitoses - atypical, bizarre mitotic figures (tripolar, quadripolar spindles)
- Loss of polarity - disorganized cell arrangement relative to each other and basement membranes
- Tumor giant cells - single huge polymorphic nucleus or multiple large hyperchromatic nuclei
- Invasive - infiltrating, irregular borders; destroys adjacent tissue
- Metastasis - spread via lymphatics, blood vessels, or body cavities
- Areas of necrosis - due to rapid growth outpacing vascular supply
Histologic example:
3. Borderline / Intermediate Tumors
Some tumors occupy an uncertain middle ground - they show features of both benign and malignant behavior but do not clearly fit either category. They are called borderline, low malignant potential, or intermediate-grade tumors.
- Show nuclear abnormalities and mitotic activity exceeding benign tumors but lack frank stromal invasion
- Classic example: borderline epithelial tumors of the ovary (serous borderline tumor / tumor of low malignant potential)
- Behavior is unpredictable - they may recur locally or, rarely, metastasize
Comparison Table: Benign vs. Malignant
| Feature | Benign | Malignant |
|---|---|---|
| Differentiation | Well-differentiated | Variable; may be anaplastic |
| Growth rate | Slow | Usually rapid; may vary |
| Encapsulation | Often encapsulated | Rarely encapsulated |
| Local invasion | No - expansile, pushing | Yes - infiltrating |
| Metastasis | Never | Often (hallmark feature) |
| Mitoses | Rare, normal | Frequent, often atypical |
| Nuclear features | Normal | Pleomorphism, hyperchromasia |
| Necrosis | Rare | Common (rapidly growing tumors) |
| Recurrence after excision | Rare | More common |
| Effect on patient | Usually non-fatal | Often fatal if untreated |
Nomenclature Summary by Tissue of Origin
| Tissue | Benign | Malignant |
|---|---|---|
| Fibrous tissue | Fibroma | Fibrosarcoma |
| Fat | Lipoma | Liposarcoma |
| Cartilage | Chondroma | Chondrosarcoma |
| Bone | Osteoma | Osteosarcoma |
| Blood vessels | Hemangioma | Angiosarcoma |
| Smooth muscle | Leiomyoma | Leiomyosarcoma |
| Striated muscle | Rhabdomyoma | Rhabdomyosarcoma |
| Squamous epithelium | Squamous cell papilloma | Squamous cell carcinoma |
| Glandular epithelium | Adenoma | Adenocarcinoma |
| Melanocytes | Nevus | Melanoma |
| Hematopoietic cells | - | Leukemia |
| Lymphoid tissue | - | Lymphoma |
| Placenta | Hydatidiform mole | Choriocarcinoma |
Note on exceptions: Some malignant tumors carry names ending in -oma (misleadingly suggesting benign): lymphoma, melanoma, mesothelioma, and seminoma are all malignant. These exceptions are firmly entrenched in medical terminology.
Sources: Robbins, Cotran & Kumar - Pathologic Basis of Disease; Robbins & Kumar Basic Pathology (Robbins Pathology)
This is a shared conversation. Sign in to Orris to start your own chat.