Aids - etiology,route of transmission, natural history, diagnosis Reference from robins
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Loading Image
I now have all the content needed. Let me compile a thorough, well-organized response from Robbins.
AIDS - Etiology, Routes of Transmission, Natural History, and Diagnosis
Reference: Robbins, Cotran & Kumar - Pathologic Basis of Disease
1. Etiology
The Causative Agent
AIDS is caused by the human immunodeficiency virus (HIV), a nontransforming human retrovirus belonging to the lentivirus family. Related lentiviruses include feline immunodeficiency virus, simian immunodeficiency virus (SIV), visna virus of sheep, bovine immunodeficiency virus, and equine infectious anemia virus.
Two genetically different but related forms exist:
- HIV-1: Most common type; associated with AIDS in the United States, Europe, and Central Africa
- HIV-2: Causes a similar disease, principally in West Africa and India
Blood donated for transfusion is routinely screened for both HIV-1 and HIV-2 seropositivity.
Structure of HIV
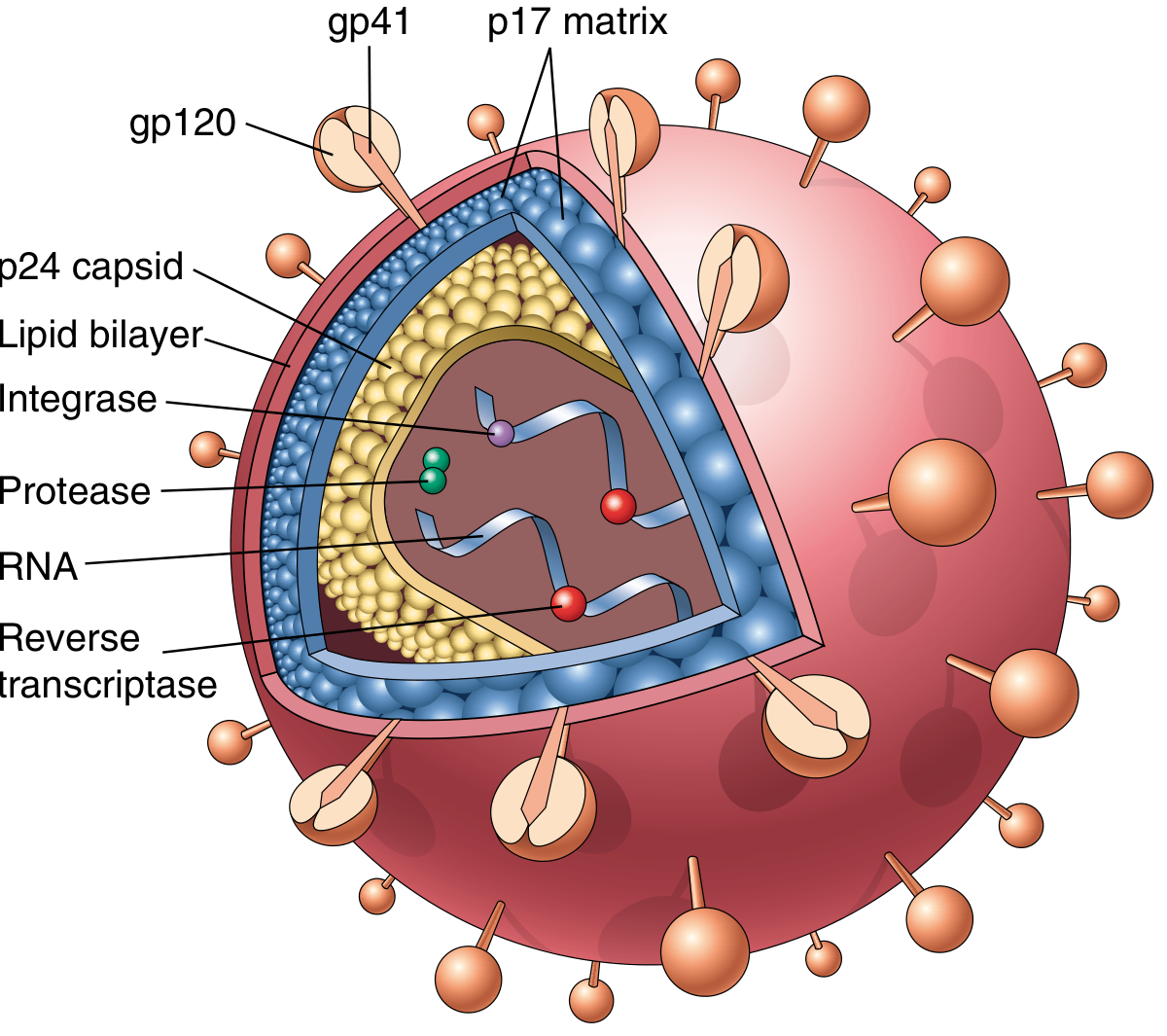
Fig. 6.38 - The structure of the HIV-1 virion. The viral particle is covered by a lipid bilayer derived from the host cell and studded with viral glycoproteins gp41 and gp120.
The HIV-1 virion is spherical with an electron-dense, cone-shaped core surrounded by a lipid envelope derived from the host cell membrane. Key components:
| Component | Function |
|---|---|
| gp120 | Surface glycoprotein; binds CD4 receptor on host cells |
| gp41 | Transmembrane glycoprotein; mediates viral-cell membrane fusion |
| p17 (matrix protein) | Lies beneath the virion envelope |
| p24 (major capsid protein) | Most abundant viral antigen; detected by ELISA for HIV diagnosis |
| p7/p9 | Nucleocapsid protein |
| Two copies of viral RNA | Genome |
| Reverse transcriptase | Converts viral RNA to DNA (provirus) |
| Integrase | Integrates proviral DNA into host genome |
| Protease | Cleaves precursor proteins into mature viral proteins |
The HIV-1 RNA genome contains: LTR, gag, pol, and env genes (standard retroviral genes), plus accessory genes: tat, rev, vif, nef, vpr, and vpu. The tat (transactivator) gene product causes a ~1000-fold increase in transcription of viral genes, critical for replication.
2. Routes of Transmission
Transmission of HIV occurs under conditions that facilitate exchange of blood or body fluids containing the virus or virus-infected cells. The three major routes are:
A. Sexual Contact (most common globally)
- Men who have sex with men (MSM): account for >50% of reported cases in the United States (about 70% of new cases in 2016)
- Heterosexual transmission: ~20% of cases in the U.S.; globally, the most common mode of spread, especially in sub-Saharan Africa where >50% of infected individuals are female
- Risk is enhanced by co-existing STDs - especially those with genital ulceration (syphilis, chancroid, herpes); gonorrhea and chlamydia also serve as cofactors (genital inflammation provides more infectable cells)
B. Parenteral Inoculation
- Intravenous drug users: the largest parenteral group; transmission by sharing needles, syringes, and other paraphernalia contaminated with HIV-containing blood
- Hemophiliacs: historically received contaminated factor VIII/IX concentrates - now virtually eliminated due to recombinant clotting factors and blood screening
- Blood transfusion recipients: risk now extremely small (estimated at 1 in >2 million units transfused) due to anti-HIV antibody screening
C. Mother-to-Infant (Vertical) Transmission
The major cause of pediatric AIDS. Infected mothers can transmit infection via:
- In utero - transplacental spread
- Intrapartum - during delivery through an infected birth canal (most common in the U.S.)
- Postpartum - ingestion of breast milk
Transmission rates vary from 7% to 49% worldwide. Risk is higher with high maternal viral load, low CD4+ T-cell counts, and chorioamnionitis. ART given to infected pregnant women has virtually eliminated mother-to-child transmission in the U.S.
What Does NOT Transmit HIV
Extensive studies confirm HIV cannot be transmitted by casual personal contact in household, workplace, or school settings. Spread by insect bites is virtually impossible. The risk to healthcare workers after needle-stick injury is ~0.3% (vs. ~30% for hepatitis B); ART within 24-48 hours of needle stick reduces this risk 8-fold.
3. Natural History (Clinical Course)
HIV infection progresses through three distinct phases:
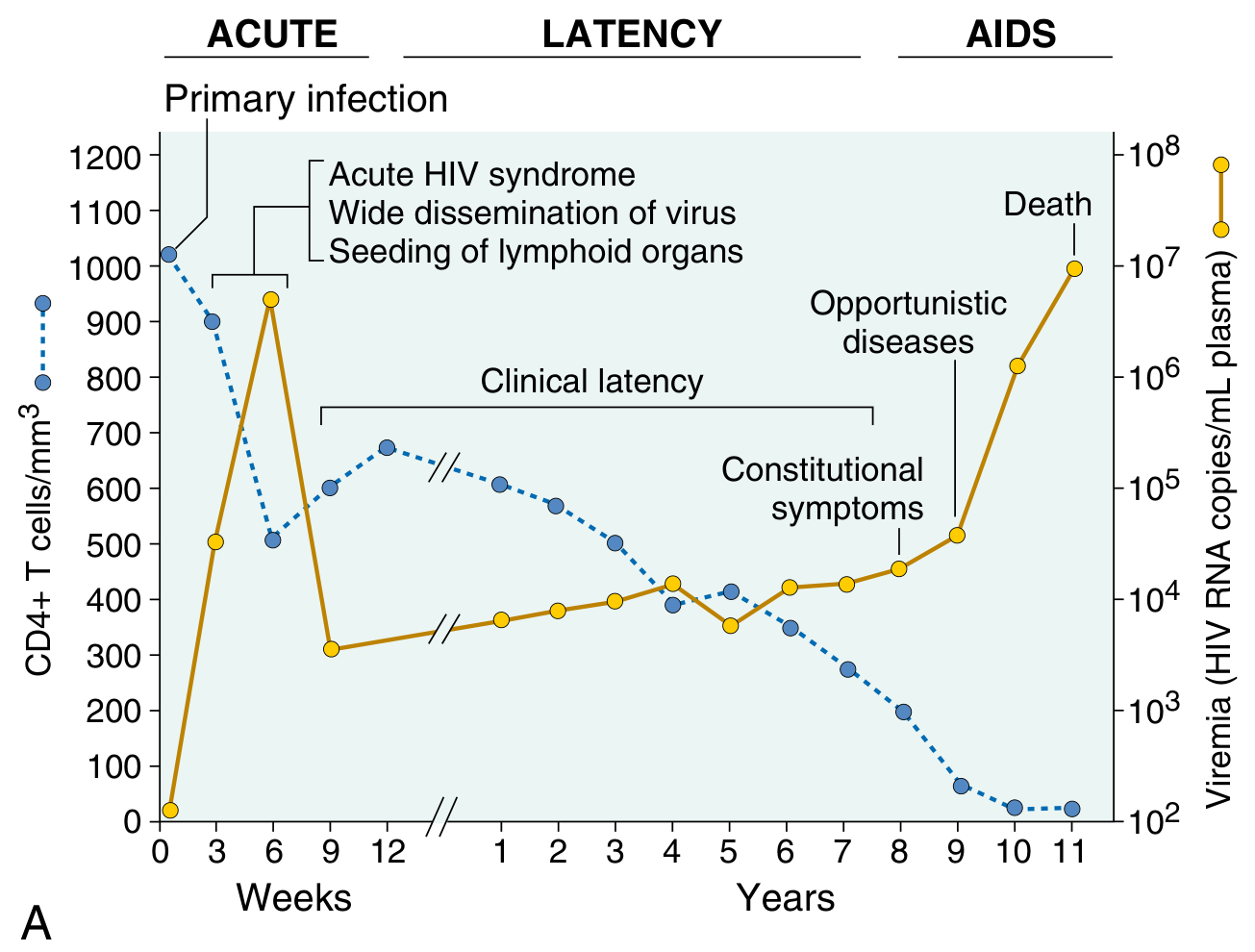
Fig. 6.42 - Clinical course of HIV infection showing CD4+ T-cell count (blue dashed) and viral load (gold) over time across three phases.
Phase 1: Acute Retroviral Syndrome (Weeks 3-6 post-infection)
- HIV enters the body through mucosal tissues - DCs in epithelia capture the virus, migrate to lymph nodes, and pass HIV to CD4+ T cells via direct cell-to-cell contact
- Within days of first exposure: viral replication detected in lymph nodes, followed by viremia (high HIV particles in blood)
- Virus disseminates throughout the body, seeding helper T cells and macrophages in peripheral lymphoid tissues
- Host mounts antiviral humoral and cell-mediated responses - seroconversion occurs within 3 to 7 weeks of presumed exposure
- By ~12 weeks: CD8+ cytotoxic T cells develop; immune response partially controls viremia (drops to low but detectable levels - the "viral set point")
Clinical presentation (occurs in 40%-90% of primary infections):
- Non-specific, self-limited flu-like illness lasting 2-4 weeks
- Sore throat, myalgias, fever, weight loss, fatigue, generalized lymphadenopathy, rash
- Often accompanied by a transient drop in CD4+ T-cell count followed by partial recovery
Phase 2: Chronic Infection / Clinical Latency (Years 1-10)
- Lymph nodes and spleen are sites of continuous HIV replication and cell destruction
- Few or no clinical manifestations (hence "clinical latency") - but viral destruction of CD4+ T cells continues silently
- HIV destroys up to 2 × 10⁹ CD4+ T cells every day; early on, T cells are replaced almost as quickly as destroyed
- CD4+ count steadily declines from ~1000 cells/µL at baseline, falling at ~50-80 cells/µL per year in untreated patients
- The viral set point at end of acute phase predicts rate of CD4+ decline: only 8% of patients with <4,350 viral RNA copies/µL progressed to AIDS in 5 years, vs. 62% with >36,270 copies
Minor manifestations during this phase:
- Oral candidiasis (thrush)
- Vaginal candidiasis
- Herpes zoster
- Tuberculosis (especially common in sub-Saharan Africa)
- Autoimmune thrombocytopenia
Phase 3: AIDS (End Stage)
- Triggered when CD4+ count falls below 200 cells/µL (CDC definition)
- Characterized by breakdown of host defense, a dramatic increase in viral load, and severe life-threatening clinical disease
- Without treatment, most patients progress to AIDS after 7 to 10 years of chronic phase
Constitutional symptoms:
- Long-lasting fever (>1 month), fatigue, weight loss, diarrhea, generalized lymphadenopathy
AIDS Indicator / Defining Conditions:
| Category | Examples |
|---|---|
| Opportunistic Infections | Pneumocystis jirovecii pneumonia (15%-30%), Toxoplasma encephalitis, CMV retinitis/colitis, Candida esophagitis, Cryptococcal meningitis, Mycobacterium avium complex (MAC), Cryptosporidium diarrhea |
| Secondary Neoplasms | Kaposi sarcoma (HHV-8), Non-Hodgkin lymphoma, CNS lymphoma, invasive cervical carcinoma |
| Neurologic Disease | HIV encephalopathy ("AIDS dementia"), vacuolar myelopathy |
Special variants of disease course:
- Rapid progressors: Chronic phase telescoped to 2-3 years
- Long-term nonprogressors: ~1% remain asymptomatic for 10+ years with stable CD4+ counts and low viral loads without ART
- Elite controllers: Usually <50 viral RNA copies/mL; have vigorous anti-HIV immune responses and favorable HLA alleles
CDC Classification of HIV Infection
| Clinical Category | CD4 ≥500/µL | CD4 200-499/µL | CD4 <200/µL |
|---|---|---|---|
| A - Asymptomatic, acute HIV, or PGL | A1 | A2 | A3 |
| B - Symptomatic (not A or C) | B1 | B2 | B3 |
| C - AIDS indicator conditions | C1 | C2 | C3 |
(PGL = persistent generalized lymphadenopathy)
4. Diagnosis
A. Serologic Tests (Antibody-Based)
- ELISA for anti-HIV antibodies (also detects p24 antigen in 4th-generation combination assays): Standard screening test
- Highly sensitive but less specific; positive results must be confirmed
- Western blot: Confirmatory test - identifies antibodies against specific viral proteins (gp120, gp41, p24)
- Seroconversion occurs within 3-7 weeks of exposure; the "window period" (antibody-negative but infected) is a source of false-negative screening
B. Virologic / Molecular Tests
-
HIV-1 RNA PCR (viral load): Quantifies HIV RNA copies/mL plasma
- Diagnostic in acute infection (before seroconversion)
- Marker of disease progression and treatment response
- Viral set point correlates with rate of CD4+ decline and risk of progression
-
p24 antigen detection (ELISA): p24 is the most abundant viral antigen; detected in early infection when antibody tests may be negative
C. CD4+ T-Cell Count
- Primary clinical measurement for determining when to start ART and assessing immune status
- CD4+ <200 cells/µL = AIDS diagnosis, regardless of symptoms
- Most reliable short-term indicator of disease progression
D. Nucleic Acid Amplification Tests (NAATs)
- Used in early/acute infection and in neonates of HIV-positive mothers where maternal antibodies confound serologic testing
- HIV DNA PCR used in infants to detect integrated proviral DNA
E. Additional Testing
- HIV genotyping / resistance testing: before starting or changing ART
- CBC with differential: to detect lymphopenia and thrombocytopenia
- Opportunistic infection workup: chest X-ray, sputum for P. jirovecii, toxoplasma serology, CMV load, fungal cultures
Source: Robbins, Cotran & Kumar - Pathologic Basis of Disease, Chapter 6 (Diseases of the Immune System), pp. 235-246
This is a shared conversation. Sign in to Orris to start your own chat.