Tell me about ABG from basics to clinical
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have all the key content I need. Let me compile the comprehensive ABG guide.
Arterial Blood Gas (ABG): From Basics to Clinical
1. What Is an ABG?
An arterial blood gas is a sample of blood taken from an artery (most commonly the radial artery) that measures the partial pressures of oxygen and carbon dioxide, pH, and bicarbonate directly in arterial blood. It is the gold standard for evaluating oxygenation, ventilation, and acid-base status simultaneously. Unlike a venous sample, it reflects what the lungs are actually delivering to the tissues.
2. Normal Values
| Parameter | Normal Range | Meaning |
|---|---|---|
| pH | 7.35 - 7.45 | Hydrogen ion concentration; <7.35 = acidemia, >7.45 = alkalemia |
| PaCO₂ | 35 - 45 mmHg | Partial pressure of CO₂; reflects ventilation (lung function) |
| PaO₂ | 80 - 100 mmHg | Partial pressure of O₂; reflects oxygenation |
| HCO₃⁻ | 22 - 26 mEq/L | Bicarbonate; reflects metabolic (renal) status |
| SaO₂ | 95 - 100% | Oxygen saturation of hemoglobin |
| Base Excess (BE) | -2 to +2 mEq/L | Metabolic acid-base reserve; negative = deficit |
A measured PaO₂ by ABG is the gold standard for oxygenation and can exclude interference by abnormal hemoglobins (carboxyhemoglobin, methemoglobin) that a pulse oximeter cannot detect. - Murray & Nadel's Textbook of Respiratory Medicine
3. The Physiologic Foundation: Henderson-Hasselbalch
The relationship between pH, PaCO₂, and HCO₃⁻ is governed by the Henderson-Hasselbalch equation:
$$\text{pH} = \text{pK} + \log \frac{[\text{HCO}_3^-]}{[\text{H}_2\text{CO}_3]}$$
Since H₂CO₃ is in equilibrium with dissolved CO₂ (H₂CO₃ = 0.0307 × PaCO₂), this becomes:
$$\text{pH} = 6.1 + \log \frac{[\text{HCO}_3^-]}{0.0307 \times \text{PaCO}_2}$$
Key concept: pH is determined by the ratio of HCO₃⁻ to PaCO₂ - not by either value alone. This explains why compensation can normalize pH even when both values are abnormal. - Costanzo Physiology, 7th Edition
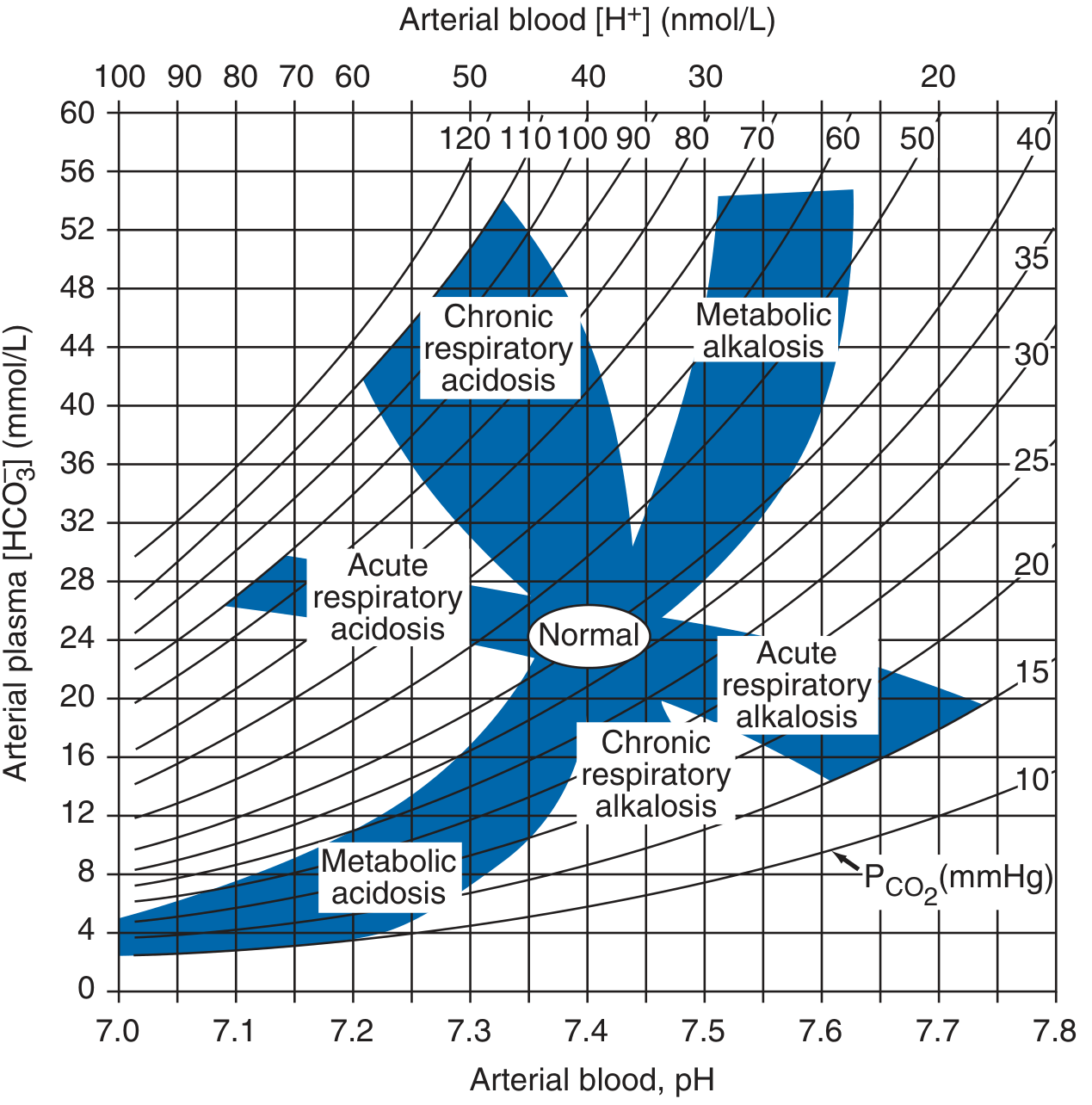
4. The Four Primary Acid-Base Disorders
Respiratory Disorders (CO₂-driven)
| Disorder | pH | PaCO₂ | HCO₃⁻ (compensatory) | Mechanism |
|---|---|---|---|---|
| Respiratory Acidosis | ↓ | ↑ (>45) | ↑ (secondary) | Hypoventilation → CO₂ retention |
| Respiratory Alkalosis | ↑ | ↓ (<35) | ↓ (secondary) | Hyperventilation → CO₂ washout |
Metabolic Disorders (HCO₃⁻-driven)
| Disorder | pH | HCO₃⁻ | PaCO₂ (compensatory) | Mechanism |
|---|---|---|---|---|
| Metabolic Acidosis | ↓ | ↓ (<22) | ↓ (secondary) | Acid gain or HCO₃⁻ loss |
| Metabolic Alkalosis | ↑ | ↑ (>26) | ↑ (secondary) | Acid loss or HCO₃⁻ gain |
5. Compensation: The Body's Response
Compensation is never complete - it brings pH toward normal but never fully corrects it. Compensation in the same direction as the primary change is the expected response; opposite directions suggest a mixed disorder.
| Primary Disorder | Compensatory Response | Formula |
|---|---|---|
| Metabolic Acidosis | Hyperventilation ↓ PaCO₂ | Expected PaCO₂ = 1.5 × [HCO₃⁻] + 8 ± 2 (Winter's formula); or ΔPaCO₂ = 1.3 × ΔHCO₃⁻ |
| Metabolic Alkalosis | Hypoventilation ↑ PaCO₂ | ΔPaCO₂ = 0.6 × ΔHCO₃⁻ |
| Acute Resp. Acidosis | Buffering ↑ HCO₃⁻ | For every ↑10 mmHg PaCO₂ → HCO₃⁻ ↑ 1 mEq/L |
| Chronic Resp. Acidosis | Renal retention of HCO₃⁻ | For every ↑10 mmHg PaCO₂ → HCO₃⁻ ↑ 3-4 mEq/L |
| Acute Resp. Alkalosis | Buffering ↓ HCO₃⁻ | For every ↓10 mmHg PaCO₂ → HCO₃⁻ ↓ 2 mEq/L |
| Chronic Resp. Alkalosis | Renal excretion of HCO₃⁻ | For every ↓10 mmHg PaCO₂ → HCO₃⁻ ↓ 5 mEq/L |
Timing matters: Respiratory compensation for metabolic disorders is rapid (minutes to hours). Metabolic/renal compensation for respiratory disorders takes 3-5 days to become fully established. - Roberts and Hedges' Clinical Procedures in Emergency Medicine
6. Step-by-Step ABG Interpretation
Harrison's 8-Step Approach (Harrison's Principles of Internal Medicine, 22nd Ed.)
- Obtain ABG and serum electrolytes simultaneously - before therapy
- Check internal consistency - calculated HCO₃⁻ on ABG should match measured HCO₃⁻ on electrolytes within ±2 mEq/L
- Assess the anion gap (AG) - correct for albumin if hypoalbuminemia present
- Identify known causes of high-AG acidosis (ketoacidosis, lactic acidosis, CKD, toxic alcohols)
- Identify known causes of non-gap acidosis (GI HCO₃⁻ loss, renal tubular acidosis)
- Estimate predicted compensatory response and compare to actual
- Compare delta values (ΔAG vs. ΔHCO₃⁻) - the delta-delta ratio
- Compare change in [Cl⁻] with change in [Na⁺]
Simplified Bedside Framework
Step 1: Look at pH
< 7.35 = Acidemia
> 7.45 = Alkalemia
Step 2: Find the primary cause
If acidemia:
- PaCO₂ >45 → Respiratory Acidosis (primary)
- HCO₃⁻ <22 → Metabolic Acidosis (primary)
If alkalemia:
- PaCO₂ <35 → Respiratory Alkalosis (primary)
- HCO₃⁻ >26 → Metabolic Alkalosis (primary)
Step 3: Check compensation (is it adequate?)
Use formulas above. If actual ≠ predicted → mixed disorder
Step 4: Calculate Anion Gap (if acidosis present)
AG = Na⁺ - (Cl⁻ + HCO₃⁻)
Normal = 8-12 mEq/L (if albumin is normal)
Step 5: If high AG, check Delta-Delta ratio
Delta-Delta = (AG - 12) / (24 - HCO₃⁻)
< 1 → mixed high-AG + normal-AG acidosis
1-2 → pure high-AG acidosis
> 2 → high-AG acidosis + concurrent metabolic alkalosis
7. The Anion Gap in Detail
The AG estimates unmeasured anions in plasma:
$$\text{AG} = \text{Na}^+ - (\text{Cl}^- + \text{HCO}_3^-)$$
Normal value = 8-12 mEq/L (average ~10). The unmeasured anions include albumin, phosphate, sulfate, and organic anions. - Harrison's Principles of Internal Medicine, 22nd Ed.
Albumin Correction
Because albumin is the major unmeasured anion, hypoalbuminemia lowers the normal AG. Correct with:
$$\text{Corrected AG} = \text{Measured AG} + 2.5 \times (4.5 - \text{albumin in g/dL})$$
High-AG Metabolic Acidosis - Causes (Mnemonic: A MUDPILE CAT)
- A spirin (salicylates)
- M ethanol / Metformin
- U remia (renal failure)
- D iabetic ketoacidosis
- P araldehyde / Phenformin
- I soniazid / Iron
- L actate (shock, sepsis, ischemia)
- E thylene glycol
- C arbon monoxide / Cyanide
- A lcoholic ketoacidosis
- T oluene
Normal-AG (Hyperchloremic) Metabolic Acidosis - Causes
- GI losses: Diarrhea (most common), ileostomy, fistula
- Renal: Renal tubular acidosis (RTA Types 1, 2, 4), post-obstructive uropathy
- Iatrogenic: Large volumes of normal saline ("dilutional" or "hyperchloremic" acidosis)
- Urinary diversion (ureteral-intestinal anastomosis)
8. Lactic Acidosis - Special Mention
Type A (tissue hypoperfusion): circulatory failure, shock, cardiac failure, severe anemia, carbon monoxide, cyanide poisoning
Type B (aerobic/metabolic): malignancies, metformin/biguanides, HIV reverse-transcriptase inhibitor drugs, hepatic failure, thiamine deficiency, seizures, toxic alcohols
Unrecognized bowel ischemia or infarction in elderly patients with severe atherosclerosis receiving vasopressors is a relatively common cause of lactic acidosis. - Harrison's Principles of Internal Medicine, 22nd Ed.
9. Metabolic Alkalosis
Causes:
- Chloride-responsive (urine Cl⁻ <20 mEq/L): Vomiting, nasogastric suction, diuretics (furosemide), post-hypercapnic alkalosis
- Chloride-resistant (urine Cl⁻ >20 mEq/L): Primary hyperaldosteronism, Cushing's syndrome, Bartter/Gitelman syndrome, exogenous steroids
Treatment: Address the underlying cause. Chloride-responsive types respond to IV saline + KCl repletion.
10. Respiratory Acidosis & Alkalosis
Respiratory Acidosis
Causes: Any cause of hypoventilation - COPD, asthma (severe), pneumonia, neuromuscular disease (Guillain-Barre, MG), obesity hypoventilation, opioid overdose, airway obstruction
ABG: pH ↓, PaCO₂ ↑, HCO₃⁻ slightly ↑ (acute) or markedly ↑ (chronic)
Respiratory Alkalosis
Causes: Hyperventilation - anxiety, pain, fever, sepsis (early), salicylate toxicity, hepatic encephalopathy, pregnancy, high-altitude, mechanical over-ventilation, PE (early)
ABG: pH ↑, PaCO₂ ↓, HCO₃⁻ slightly ↓
11. Oxygenation Parameters from ABG
Alveolar-Arterial (A-a) Gradient
$$P_A O_2 = F_i O_2 \times (P_{atm} - P_{H_2O}) - \frac{P_a CO_2}{R}$$
At room air (FiO₂ = 0.21, sea level):
$$P_A O_2 = 150 - \frac{PaCO_2}{0.8}$$
$$A\text{-}a \text{ gradient} = PAO_2 - PaO_2$$
Normal: <10-15 mmHg in young adults; increases with age (~2.5 mmHg per decade)
Clinical use:
| Finding | A-a Gradient | Interpretation |
|---|---|---|
| Hypoxemia + normal A-a gradient | Normal | Hypoventilation (PaCO₂ high), high altitude |
| Hypoxemia + elevated A-a gradient | Elevated | V/Q mismatch, shunt, diffusion defect |
Causes of Hypoxemia
- Hypoventilation - ↑PaCO₂, normal A-a gradient
- V/Q mismatch - most common; responds to O₂
- Shunt - does NOT respond to 100% O₂ (e.g., cyanotic heart disease, ARDS)
- Diffusion impairment - interstitial lung disease
- Low inspired O₂ - altitude
12. Pulse Oximetry vs. ABG - Key Differences
Pulse oximetry cannot detect:
- Hypercarbia (especially in patients on supplemental O₂, where SpO₂ remains normal while PaCO₂ rises silently)
- Carboxyhemoglobin (reads as normal/high SaO₂)
- Methemoglobin (reads ~85% regardless)
- Dark skin pigmentation - studies show overestimation of SaO₂ in Black patients
"Of all messages to trainees... supplemental oxygen moves the arterial PO₂ farther up onto the flat portion of the oxyhemoglobin dissociation curve, so that a similar rise in PCO₂ and fall in PO₂ cannot be detected by a drop in saturation." - Murray & Nadel's Textbook of Respiratory Medicine
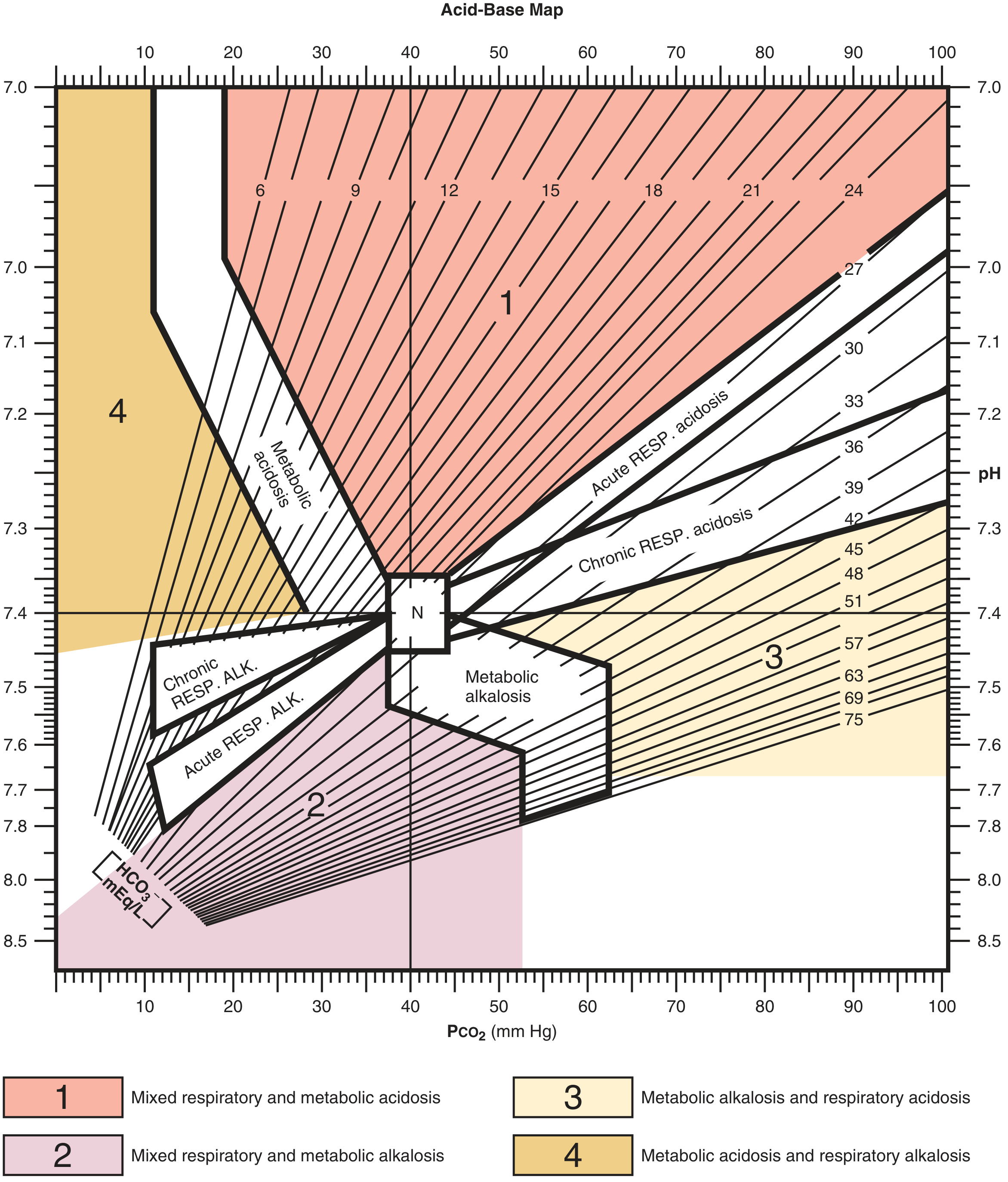
13. Mixed Acid-Base Disorders
These are independently coexisting disorders, not compensatory responses. They are common in critically ill patients and can cause dangerous pH extremes.
| Mixed Disorder | Key Clue | Clinical Example |
|---|---|---|
| Met. acidosis + Resp. alkalosis | PaCO₂ lower than predicted | Salicylate OD, septic shock, lactic acidosis |
| Met. acidosis + Resp. acidosis | PaCO₂ higher than predicted | Pneumonia + severe acidosis, COPD + sepsis |
| Met. alkalosis + Resp. alkalosis | PaCO₂ does not rise; pH very high | Liver disease + diuretics |
| Met. alkalosis + Resp. acidosis | PaCO₂ elevated but pH near normal | COPD + diuretics |
| Met. acidosis + Met. alkalosis | High AG but normal HCO₃⁻ (ΔAG >> ΔHCO₃⁻) | DKA + vomiting, uremia + vomiting |
14. Base Excess (BE) / Base Deficit
The standard base excess (SBE) is the amount of acid (or base) in mmol/L needed to return pH to 7.4 at a PaCO₂ of 40 mmHg and 37°C. It isolates the metabolic component of acid-base disturbances independent of CO₂ changes.
$$\text{SBE} = [\text{HCO}3^-]{act} - 24.8 + 16.2 \times (\text{pH} - 7.40)$$
Normal: -2 to +2 mEq/L
- Negative BE (Base Deficit): metabolic acidosis
- Positive BE: metabolic alkalosis
Base deficit is particularly used in trauma and ICU settings to estimate the degree of tissue hypoperfusion (a base deficit >6 suggests significant shock). - Miller's Anesthesia, 10th Ed.
15. The Osmolal Gap - A Critical Adjunct
Used when a high-AG metabolic acidosis is present and toxic alcohol ingestion is suspected:
$$\text{Osmolal Gap} = \text{Osm}{\text{measured}} - \text{Osm}{\text{calculated}}$$
$$\text{Osm}_{\text{calc}} = 2 \times \text{Na}^+ + \frac{\text{BUN}}{2.8} + \frac{\text{Glucose}}{18}$$
Normal gap: <10 mOsm/kg. An elevated osmolal gap + elevated AG = think methanol, ethylene glycol, isopropyl alcohol, or ethanol.
Note: Ethylene glycol and methanol raise BOTH the osmolal gap (early) AND the anion gap (later, as metabolites accumulate). Isopropyl alcohol raises the osmolal gap but NOT the anion gap (its metabolite acetone is not an acid). - Roberts & Hedges' Emergency Medicine
16. Worked Clinical Examples
Example 1 - DKA
Patient: 28-year-old diabetic with polyuria, nausea, Kussmaul breathing.
- Na⁺ 138, K⁺ 3.8, Cl⁻ 98, HCO₃⁻ 8, pH 7.18, PaCO₂ 18, PaO₂ 96
Step 1: pH 7.18 → Acidemia
Step 2: HCO₃⁻ 8 → Metabolic acidosis (primary)
Step 3: Expected PaCO₂ = 1.5 × 8 + 8 = 20 ± 2. Actual = 18. Compensation adequate.
Step 4: AG = 138 - (98 + 8) = 32 → High AG
Step 5: Delta-delta = (32-12)/(24-8) = 20/16 = 1.25 → Pure high-AG acidosis
Diagnosis: High-AG metabolic acidosis (DKA) with appropriate respiratory compensation (Kussmaul breathing).
Example 2 - Septic Shock + Resp Acidosis (Mixed)
Patient: 74-year-old with sepsis, confused, on 2L O₂.
- Na⁺ 140, K⁺ 3.2, Cl⁻ 105, HCO₃⁻ 18, pH 7.25, PaCO₂ 42
Step 1: pH 7.25 → Acidemia
Step 2: HCO₃⁻ 18 → Metabolic acidosis; but PaCO₂ should be low if compensating
Step 3: Expected PaCO₂ = 1.5 × 18 + 8 = 35. Actual = 42 → Higher than expected!
Step 4: AG = 140 - (105 + 18) = 17 → High AG (lactic acidosis)
Diagnosis: Mixed metabolic acidosis + respiratory acidosis (sepsis + failure to compensate due to respiratory fatigue). This is dangerous - additive acidemia. - Harrison's Principles of Internal Medicine, 22nd Ed.
Example 3 - COPD Exacerbation
Patient: 65-year-old smoker with worsening dyspnea.
- pH 7.28, PaCO₂ 72, HCO₃⁻ 33, PaO₂ 52
Step 1: pH 7.28 → Acidemia
Step 2: PaCO₂ 72 → Respiratory acidosis
Step 3: HCO₃⁻ rose by 9 from baseline 24. For chronic: expected ↑ = 3-4 × (72-40)/10 = 9.6-12.8. Partially compensated chronic respiratory acidosis with acute-on-chronic component.
Diagnosis: Acute-on-chronic respiratory acidosis with partial renal compensation. Requires NIV/BiPAP.
17. Clinical Pearls
- pH 7.40 with abnormal PaCO₂ and HCO₃⁻ is NOT normal - think mixed disorder (e.g., met. alkalosis + resp. acidosis in COPD on diuretics)
- Normal SpO₂ does not exclude hypercarbia - always check PaCO₂ in patients at risk
- Always correct AG for albumin - a "normal" AG of 12 in a patient with albumin of 2 g/dL is actually markedly elevated
- Venous blood gas (VBG) is adequate for pH and CO₂ assessment in most patients; a pH within 0.03-0.05 and PaCO₂ within 5-6 mmHg of arterial values. Use ABG when precise PaO₂ is needed.
- Treat the patient, not the number - mild acidemia (pH 7.20-7.35) may not need bicarbonate; treat the underlying cause
- In DKA, bicarbonate is only given if pH <7.0 with hemodynamic compromise - not routinely - Harrison's Principles of Internal Medicine, 22nd Ed.
- Check for co-existing disorders using delta-delta: a ratio >2 means high-AG acidosis is masking an underlying metabolic alkalosis
18. Quick Reference Summary Table
| Disorder | pH | PaCO₂ | HCO₃⁻ | Key Causes |
|---|---|---|---|---|
| Metabolic acidosis (high AG) | ↓ | ↓ (comp.) | ↓↓ | DKA, lactic acidosis, uremia, toxins |
| Metabolic acidosis (normal AG) | ↓ | ↓ (comp.) | ↓↓ | Diarrhea, RTA, saline infusion |
| Metabolic alkalosis | ↑ | ↑ (comp.) | ↑↑ | Vomiting, diuretics, hyperaldosteronism |
| Acute resp. acidosis | ↓↓ | ↑↑ | ↑ (slight) | Acute asthma, narcotic OD, airway obstruction |
| Chronic resp. acidosis | ↓ (mild) | ↑↑ | ↑↑ | COPD, obesity hypoventilation |
| Acute resp. alkalosis | ↑↑ | ↓↓ | ↓ (slight) | Anxiety, pain, early sepsis, PE |
| Chronic resp. alkalosis | ↑ (mild) | ↓↓ | ↓↓ | Hepatic encephalopathy, high altitude |
Sources:
- Harrison's Principles of Internal Medicine, 22nd Ed. (2025), Chapter 58 - Acid-Base Disorders
- Roberts and Hedges' Clinical Procedures in Emergency Medicine, Appendix A - Acid-Base Interpretation
- Murray & Nadel's Textbook of Respiratory Medicine - ABG & Oxygenation
- Miller's Anesthesia, 10th Ed. - Chapter 44, Acid-Base Disorders
- Costanzo Physiology, 7th Ed. - Henderson-Hasselbalch Equation
- Ganong's Review of Medical Physiology, 26th Ed. - Metabolic Acid-Base
This is a shared conversation. Sign in to Orris to start your own chat.