How to read a cardiotocography easily
Reading File
Finding Sources
Searching the Web
how to read cardiotocography CTG interpretation guide DR C BRAVaDO
Finding Sources
Reading Web Page
https://geekymedics.com/how-to-read-a-ctg
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have excellent content from the medical textbooks and web sources. Let me compile a thorough, well-organized answer.
How to Read a CTG (Cardiotocography)
A CTG records two things simultaneously on the same paper strip:
- Upper channel (FHR): Fetal heart rate in bpm - the wavy line you interpret
- Lower channel (UC): Uterine contractions - shown as hills/peaks
The paper runs at 3 cm/minute (standard). Each large square = 1 minute.
The Mnemonic: DR C BRaVADO
Work through every CTG in this order - never skip steps.
| Letter | Stands For | What to Do |
|---|---|---|
| DR | Define Risk | Is this a high-risk or low-risk pregnancy? (affects threshold for action) |
| C | Contractions | Count contractions per 10 minutes |
| BRa | Baseline Rate | What is the average FHR? |
| V | Variability | How much does the FHR fluctuate around the baseline? |
| A | Accelerations | Are there any heart rate spikes? |
| D | Decelerations | Are there dips in FHR, and what type are they? |
| O | Overall impression | Normal / Suspicious / Pathological / Needs urgent action |
Step 1 - Define Risk (DR)
Before you even look at the trace, ask: what clinical context am I reading this in?
High-risk features that lower your threshold for concern:
- Pre-eclampsia, diabetes, IUGR/FGR
- Prolonged pregnancy (>41 weeks), VBAC, multiple pregnancy
- Maternal medications (opioids, magnesium sulphate can alter the trace)
- Meconium-stained liquor, antepartum haemorrhage
Step 2 - Contractions (C)
Count peaks on the lower channel in any 10-minute window.
- Normal: up to 5 contractions per 10 minutes
- Tachysystole (hyperstimulation): >5 contractions per 10 minutes - this can cause fetal compromise by reducing uteroplacental perfusion time
Step 3 - Baseline Rate (BRa)
The mean FHR rounded to 5 bpm, assessed over a 10-minute window, excluding accelerations and decelerations.
| Category | Rate |
|---|---|
| Normal (reassuring) | 110-160 bpm |
| Non-reassuring (bradycardia) | 100-109 bpm |
| Abnormal | <100 bpm or >160 bpm |
- Tachycardia (>160 bpm): fever, chorioamnionitis, fetal anaemia, maternal drugs (betamimetics), fetal hypoxia
- Bradycardia (<110 bpm): cord prolapse, abruption, maternal hypotension, post-epidural, prolonged deceleration
Step 4 - Variability (V)
This is arguably the most important feature. It reflects normal autonomic nervous system function and is a sign the fetus is not acidotic.
Variability = the bandwidth of fluctuation around the baseline (measure the amplitude of the oscillations in bpm).
| Category | Amplitude | Meaning |
|---|---|---|
| Reassuring | 5-25 bpm | Normal, active fetal CNS |
| Non-reassuring | <5 bpm for 30-50 min | Suspicious; could be fetal sleep, opioids, or early hypoxia |
| Abnormal | <5 bpm for >50 min OR >25 bpm (saltatory) | Requires urgent review |
Causes of reduced variability: fetal sleep cycle (most common, lasts ~20-40 min), opioids, magnesium sulphate, fetal acidosis/hypoxia, extreme prematurity.
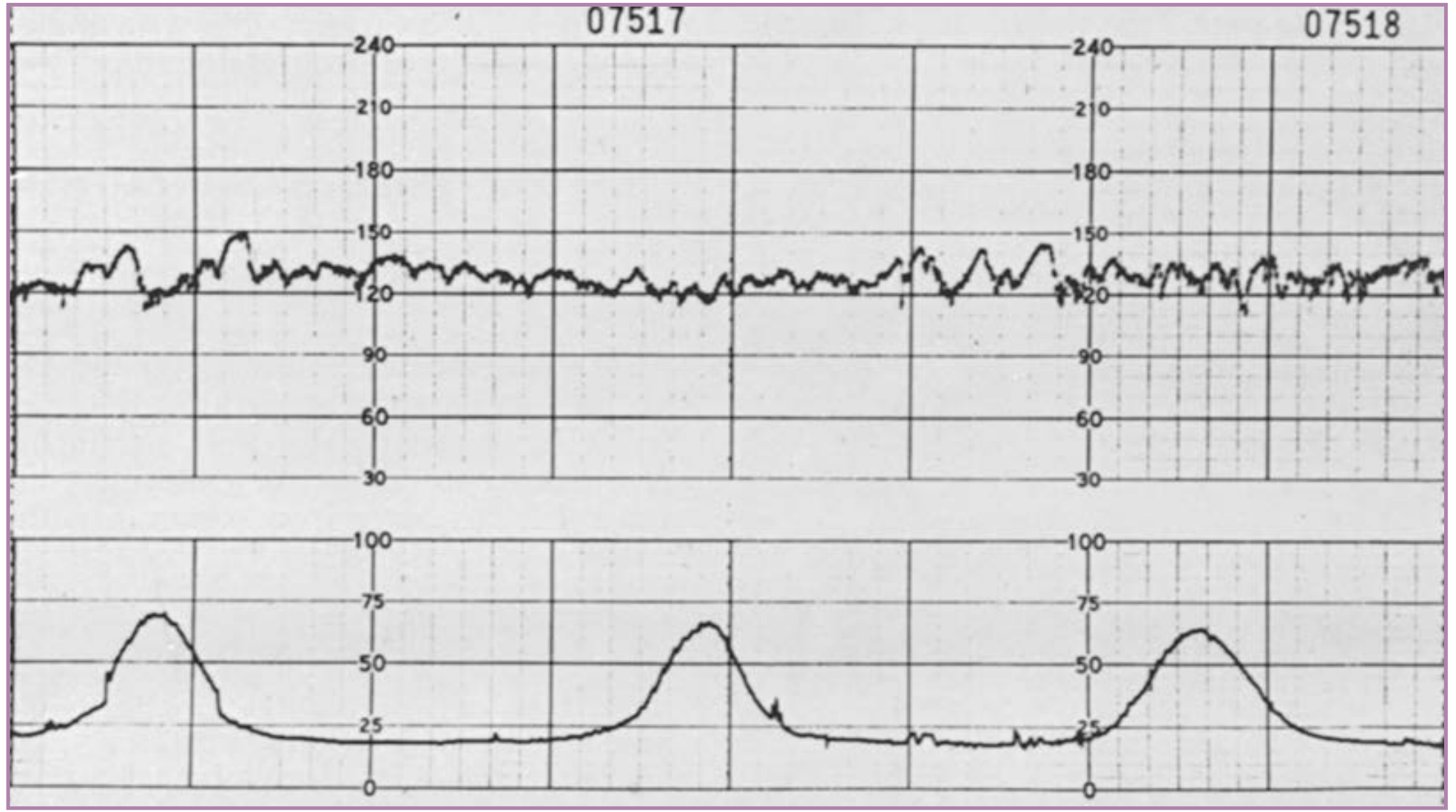
The normal CTG below shows a baseline ~120-130 bpm with good variability (5-25 bpm oscillations) and regular contractions:
Step 5 - Accelerations (A)
An acceleration = abrupt rise in FHR of ≥15 bpm above baseline, lasting ≥15 seconds (but <2 minutes), occurring in <30 seconds from onset to peak.
- Presence of accelerations = reassuring - almost always indicates absence of fetal acidaemia at that moment
- Two or more accelerations in 20 minutes = reactive (non-stress test positive)
- Absence of accelerations alone is not necessarily abnormal, but combined with other features becomes significant
For preterm fetuses (<32 weeks), smaller criteria apply: ≥10 bpm rise lasting ≥10 seconds.
Step 6 - Decelerations (D)
This is where most clinical decisions are made. There are three main types, defined by their timing relative to contractions:
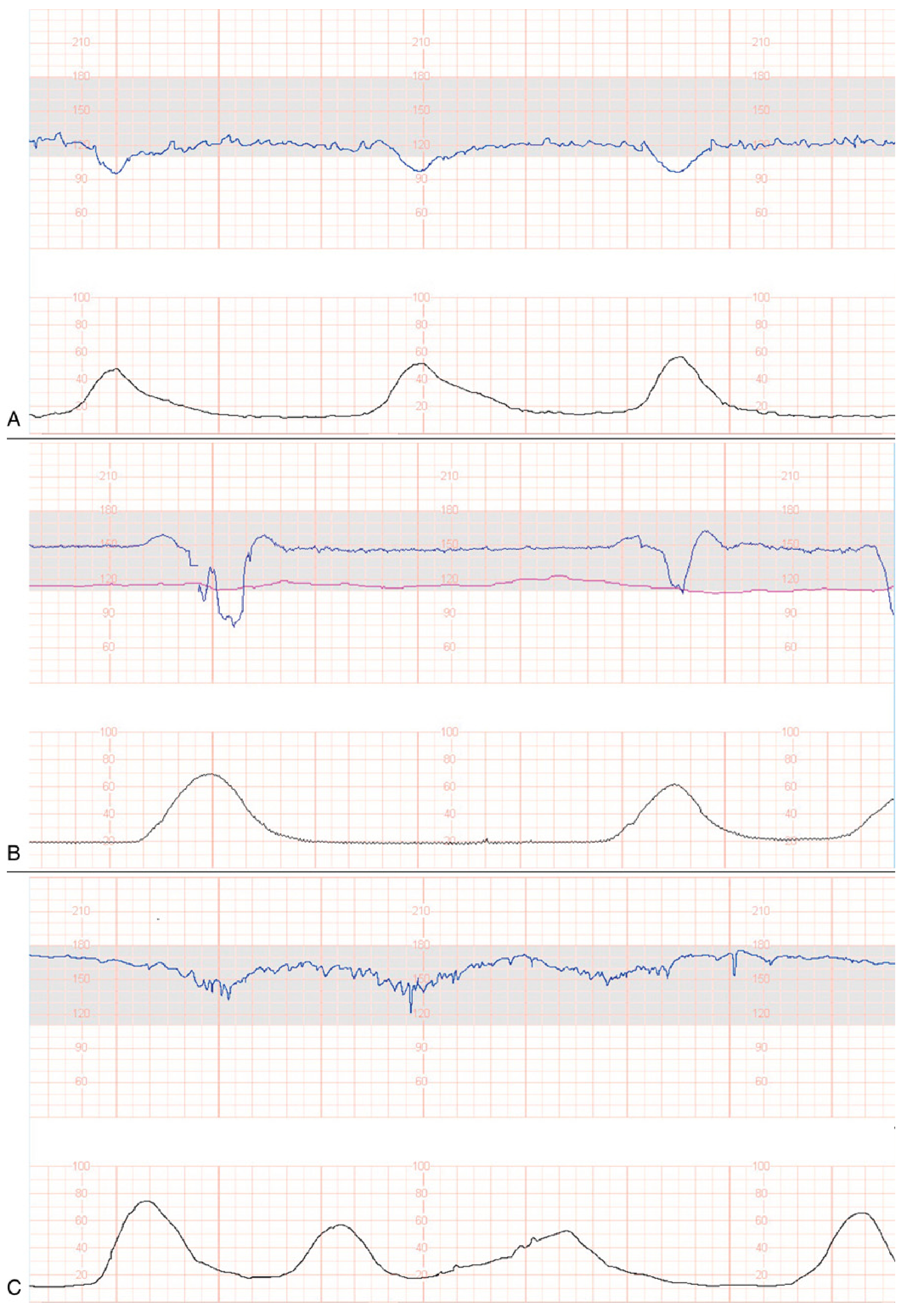
Early Decelerations (Panel A above)
- Timing: Mirror the contraction - onset, nadir and recovery match the beginning, peak and end of contraction
- Mechanism: Vagal reflex from fetal head compression
- Significance: Benign - not associated with hypoxia or acidosis
- Shape: Uniform, gradual, symmetric
Variable Decelerations (Panel B above)
- Timing: Variable - onset, depth and duration change with each contraction
- Mechanism: Umbilical cord compression (most common cause)
- Significance: Common, usually benign, but concerning if: lasting >60 sec, dropping <60 bpm, slow recovery, no shoulders (biphasic pattern), reduced variability between decelerations
- Shape: Abrupt fall (<30 sec from onset to nadir), V-shaped or W-shaped
Late Decelerations (Panel C above)
- Timing: Nadir occurs AFTER the peak of the contraction; onset, nadir and recovery are all delayed
- Mechanism: Uteroplacental insufficiency causing relative fetal hypoxia; can also indicate myocardial depression
- Significance: Always concerning - even if shallow. Recurrent late decelerations = abnormal
- Key rule: If the dip starts after the contraction peaks = late = bad
Prolonged Decelerations
- FHR drops ≥15 bpm for 2-10 minutes = prolonged deceleration
- Drop lasting >3 minutes = needs urgent intervention
- Drop <70 bpm for >60 seconds = extremely ominous, especially without variability
Step 7 - Overall Impression (O)
Classify the CTG using NICE 2017 categories:
| Category | Criteria | Action |
|---|---|---|
| Normal | All features reassuring | Continue monitoring |
| Suspicious | 1 non-reassuring feature | Review, consider further assessment |
| Pathological | 2+ non-reassuring OR 1 abnormal feature | Urgent review, consider conservative measures or delivery |
| Needs urgent action | Acute bradycardia or prolonged deceleration >3 min | Immediate intervention |
The three-tier NICHD system used in the US categorises as:
- Category I (normal): baseline 110-160, moderate variability, no late/variable decels, accelerations may or may not be present
- Category II (indeterminate): all tracings not I or III - continue monitoring, reassess
- Category III (abnormal): sinusoidal pattern, OR absent variability WITH late/variable decels or bradycardia - requires prompt intervention
(Miller's Anesthesia, 10e; Creasy & Resnik's Maternal-Fetal Medicine)
Quick Reference: Red Flags on a CTG
| Feature | Red Flag Finding |
|---|---|
| Baseline | <100 or >160 bpm |
| Variability | <5 bpm for >50 min |
| Accelerations | Absent after fetal stimulation |
| Decelerations | Late decelerations (any depth), variable decels lasting >60 sec or dropping <60 bpm, prolonged decel >3 min |
| Pattern | Sinusoidal pattern (smooth sine wave 5-15 bpm amplitude) = severe fetal anaemia |
| Contractions | >5 in 10 min (hyperstimulation) |
A Practical Memory Tip for Decelerations
"Early = OK, Variable = Maybe, Late = Late for lunch (bad)"
Or put spatially:
- Early dip mirrors the contraction hill - same shape, same time
- Variable dip is unpredictable - changes shape and timing each time
- Late dip lags behind - the heart rate only drops after the contraction peaks
Sources: Creasy & Resnik's Maternal-Fetal Medicine (Principles and Practice), Miller's Anesthesia 10e, Rosen's Emergency Medicine; Geeky Medics CTG guide; Zero to Finals CTG
This is a shared conversation. Sign in to Orris to start your own chat.