How to start tretment of Newly detected DM in female of 40 years with Hba1c 14.6 and RBS 415
Reading File
Finding Sources
Finding Sources
Searching PubMed
newly diagnosed type 2 diabetes HbA1c treatment initiation guidelines
Finding Sources
Finding Sources
Searching PubMed
"type 2 diabetes" AND "treatment initiation" AND "insulin"
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
Searching the Web
ADA 2025 guidelines newly diagnosed type 2 diabetes HbA1c greater than 10 insulin initiation treatment
I now have comprehensive information. The ADA 2025 guideline confirms: insulin is recommended when HbA1c >10% (or with symptomatic hyperglycemia). This patient has HbA1c of 14.6% - far above that threshold. Let me compile the complete answer now.
Treatment of Newly Detected Type 2 DM - 40-year-old Female, HbA1c 14.6%, RBS 415 mg/dL
This is a case of severely uncontrolled newly diagnosed T2DM with markedly elevated HbA1c (14.6%) and RBS (415 mg/dL). The standard "start metformin alone" approach is NOT appropriate here. Here is the step-by-step management:
Step 1: Immediate Assessment Before Starting Treatment
Before prescribing, rule out:
| Check | Why |
|---|---|
| Urine ketones / ABG | Rule out DKA (even in T2DM it can occur) |
| Serum electrolytes, creatinine, eGFR | Needed before starting metformin; contraindicated if eGFR <30 |
| LFTs | Metformin caution in hepatic failure |
| CBC, lipid profile, urine microalbumin | Baseline screening |
| BP, BMI | Guide drug selection (SGLT2i if HF/CKD; GLP-1 RA if obese) |
| C-peptide / anti-GAD antibodies | If suspecting LADA (Latent Autoimmune Diabetes in Adults) - important in a 40-year-old woman |
| TSH | Autoimmune thyroid disease is common in women with new-onset DM |
Step 2: Initiate Insulin - MANDATORY at This HbA1c
Per the 2025 ADA Standards of Care, insulin is recommended (not just an option) when:
- HbA1c >10% (this patient is at 14.6%)
- Symptomatic hyperglycemia (polyuria, polydipsia, weight loss)
"GLP-1 RA or GLP/GIP preferred to insulin when there is NO evidence of insulin deficiency. Insulin recommended for A1C >10% or symptomatic." - ADA 2025
Basal Insulin Regimen:
- Insulin Glargine (U-100) or Insulin Degludec - preferred basal analogs
- Starting dose: 0.1 to 0.2 units/kg/day subcutaneously at bedtime
- For this patient (assume ~60-70 kg): start 10 units at bedtime
- If obese/insulin resistant: may start at 0.4 units/kg (10-16 units)
- Titrate by 2 units every 3 days until fasting glucose is 80-130 mg/dL
Consider Basal-Bolus or Premixed Insulin if:
- Patient has very high post-meal glucose spikes
- Premixed insulin (e.g., 70/30 NPH/Regular or 30/70 Biphasic) twice daily is an alternative for adherence convenience
Step 3: Add Metformin Simultaneously
Do NOT wait - start metformin at diagnosis alongside insulin:
- Metformin 500 mg with dinner (first week)
- Increase to 500 mg twice daily (week 2)
- Target: 1000 mg twice daily (maximum recommended in most guidelines)
- Reduces insulin dose requirements, has cardiovascular neutral/favorable profile
- Continue metformin even after insulin is started - per ADA 2025
"Metformin remains the consensus first line of therapy and should be started at the time of diagnosis." - Goodman & Gilman's, p. 1061
Step 4: Add a GLP-1 RA or SGLT-2 Inhibitor (Second Agent)
Per ADA 2025, these are now the preferred second agents due to cardiorenal benefits. Since this is a 40-year-old woman (premenopausal, likely risk for cardiovascular disease over lifetime):
Option A - GLP-1 Receptor Agonist (preferred if obese, ASCVD, or MASLD/NASH):
- Semaglutide (Ozempic) 0.5 mg SC weekly → titrate to 1 mg
- OR Dulaglutide 0.75 mg SC weekly → titrate to 1.5 mg
- Benefits: significant weight loss + glycemic reduction + CV protection
Option B - SGLT-2 Inhibitor (preferred if heart failure, CKD, or eGFR ≥30):
- Empagliflozin 10 mg OD or Dapagliflozin 10 mg OD
- Benefits: weight loss, BP reduction, cardioprotective, renoprotective
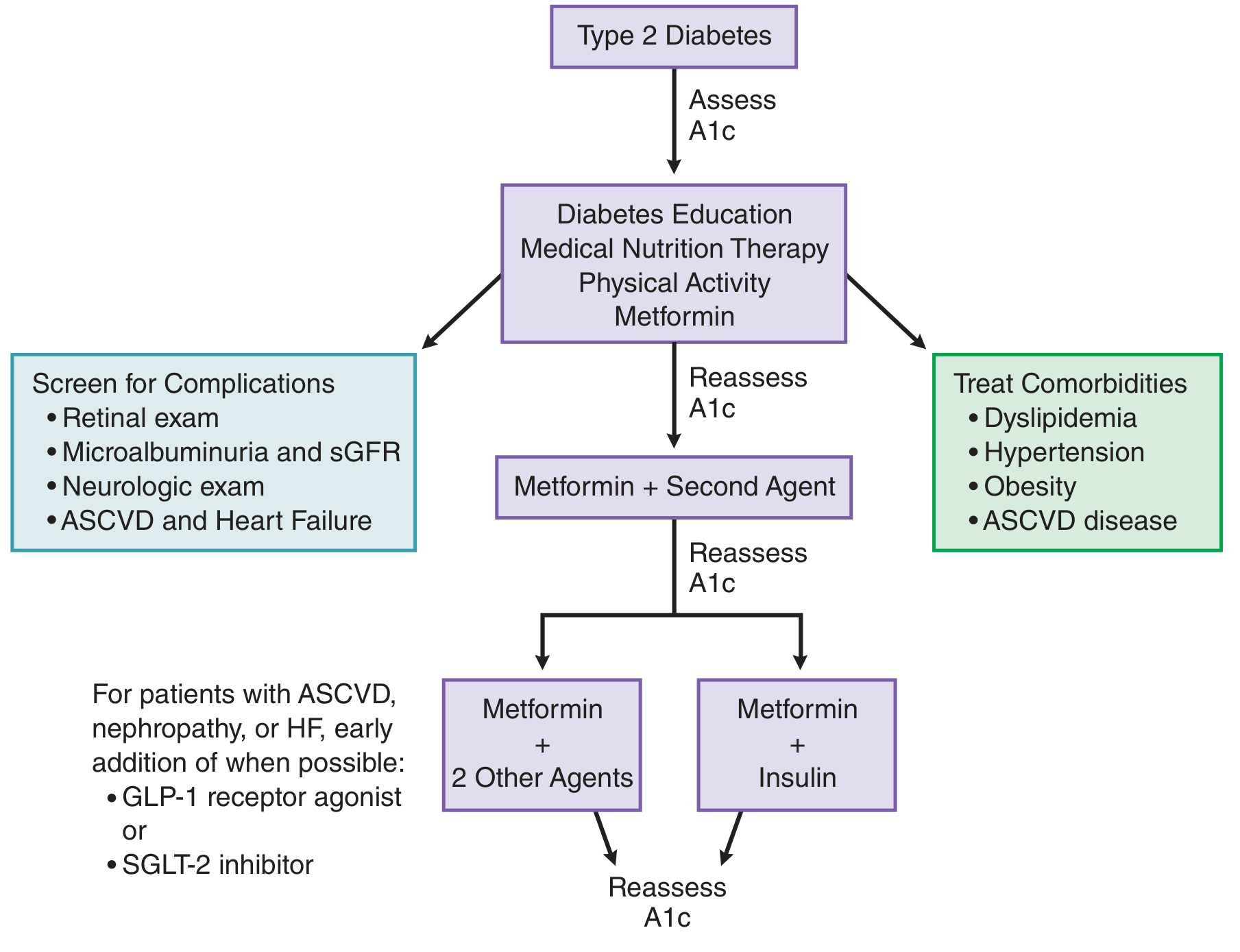
Treatment algorithm for type 2 diabetes - Goodman & Gilman's Pharmacological Basis of Therapeutics
Step 5: Lifestyle Modification - Non-Negotiable
Start immediately alongside pharmacotherapy:
- Medical Nutrition Therapy (MNT): Low-carbohydrate or low-glycemic index diet, restrict simple sugars, total caloric restriction if overweight
- Physical Activity: 150 minutes/week of moderate aerobic exercise + resistance training
- Diabetes Self-Management Education (DSMES): Teach SMBG, insulin injection technique, hypoglycemia recognition and treatment
Step 6: Monitor and Titrate
| Parameter | Target | Frequency |
|---|---|---|
| Fasting blood glucose (SMBG) | 80-130 mg/dL | Daily |
| Post-meal glucose (2hr) | <180 mg/dL | Daily |
| HbA1c | <7% (individualize) | Every 3 months initially |
| Insulin dose titration | 2 units every 3 days | Until FBG target met |
| Hypoglycemia check | BG <70 mg/dL | Each visit |
Important: With HbA1c at 14.6%, target a gradual reduction - avoid dropping HbA1c by more than 2-3% in 3 months to prevent worsening of diabetic retinopathy.
Step 7: Screen for Complications at Diagnosis
Since this is newly detected, complications may already be present (years of undetected hyperglycemia):
- Retinal examination (diabetic retinopathy)
- Urine albumin/creatinine ratio (nephropathy)
- Neurological exam / monofilament test (peripheral neuropathy)
- Foot examination (diabetic foot risk)
- ECG + lipid panel (cardiovascular risk)
Summary Prescription Plan
| Drug | Dose | Timing | Purpose |
|---|---|---|---|
| Insulin Glargine | 10 units SC | Bedtime, titrate | Basal glycemic control |
| Metformin | 500 mg → 1000 mg BD | With meals | First-line OAD |
| GLP-1 RA (Semaglutide) or SGLT-2i (Empagliflozin) | Per schedule | As directed | Cardiometabolic benefit |
Follow-up: 2 weeks after initiation (to check FBG, adjust insulin dose, check for hypoglycemia), then monthly until HbA1c <8%, then every 3 months.
Key References:
- ADA 2025 Standards of Medical Care in Diabetes - Section 9: Pharmacologic Approaches
- Goodman & Gilman's Pharmacological Basis of Therapeutics, 14th Ed. - Chapter 51, p. 1061
- Textbook of Family Medicine, 9th Ed. - Chapter 34: Insulin Initiation
Clinical Pearl: In a 40-year-old woman with HbA1c 14.6%, always consider LADA (anti-GAD antibodies). If LADA is confirmed, she will require insulin long-term and GLP-1 RAs become the preferred add-on rather than sulfonylureas (which accelerate beta-cell failure in LADA).
This is a shared conversation. Sign in to Orris to start your own chat.