Lateral wall of nose very short answer mbbs
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
Here is a complete short answer on the Lateral Wall of the Nose, suitable for MBBS exams:
Lateral Wall of the Nose
(Gray's Anatomy for Students, p. 1217-1219)
Introduction
The lateral wall of each nasal cavity is the most complex wall. It is formed by bone, cartilage, and soft tissues, and bears three scroll-like projections called conchae (turbinates) that divide the cavity into air channels (meati).
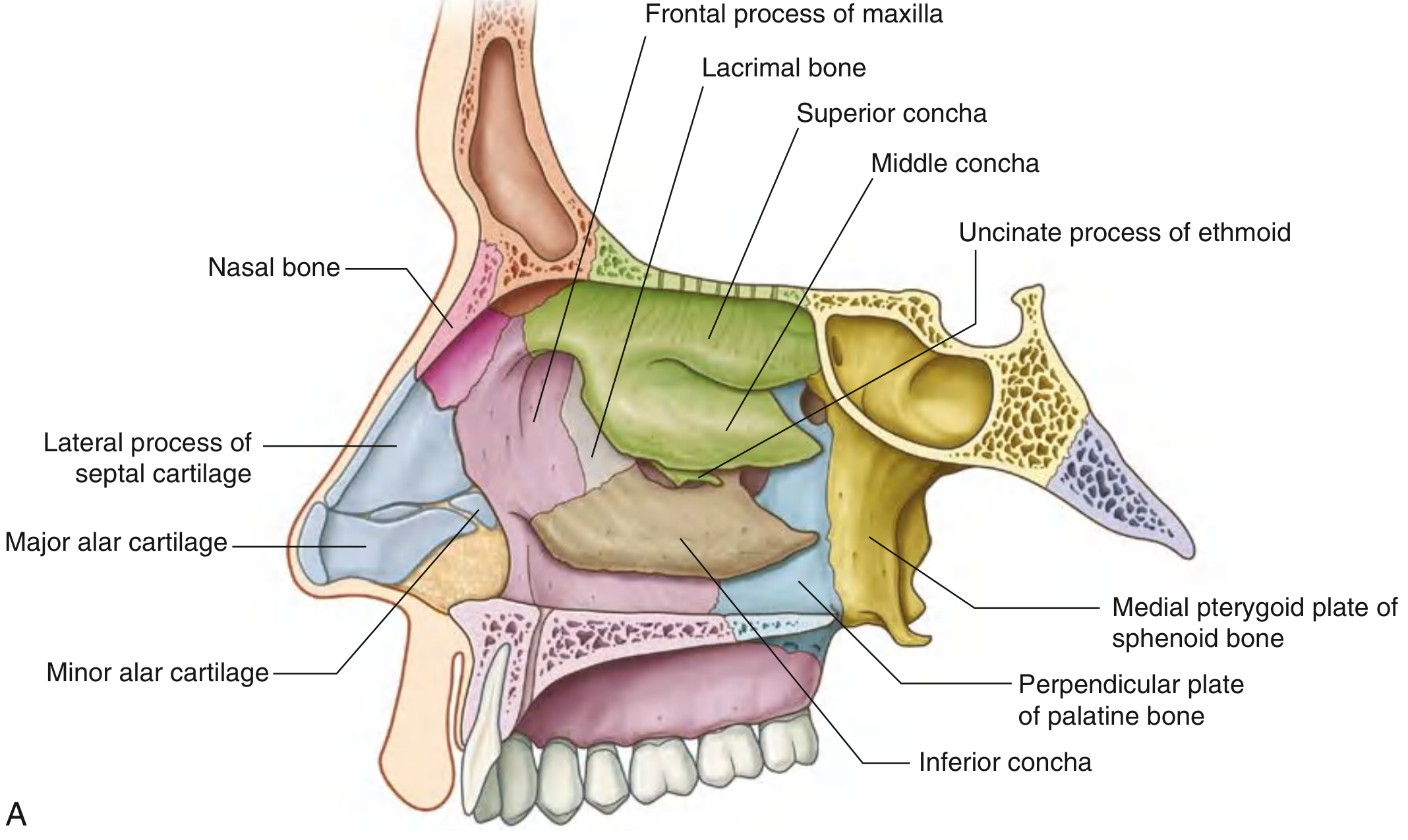
Bony Skeleton
The bony framework is contributed by six bones/structures:
| Bone | Contribution |
|---|---|
| Ethmoid bone | Ethmoidal labyrinth, superior concha, middle concha, uncinate process |
| Palatine bone | Perpendicular plate |
| Sphenoid bone | Medial pterygoid plate |
| Lacrimal bone | Medial surface |
| Maxilla | Medial surface |
| Inferior concha | A separate bone (one of the facial bones) |
In the external nose, the lateral wall is additionally supported by cartilage: the lateral process of the septal cartilage and the major alar cartilages.
Conchae (Turbinates)
Three shelf-like projections extend medially into the nasal cavity:
- Superior concha - part of ethmoid
- Middle concha - part of ethmoid
- Inferior concha - independent bone
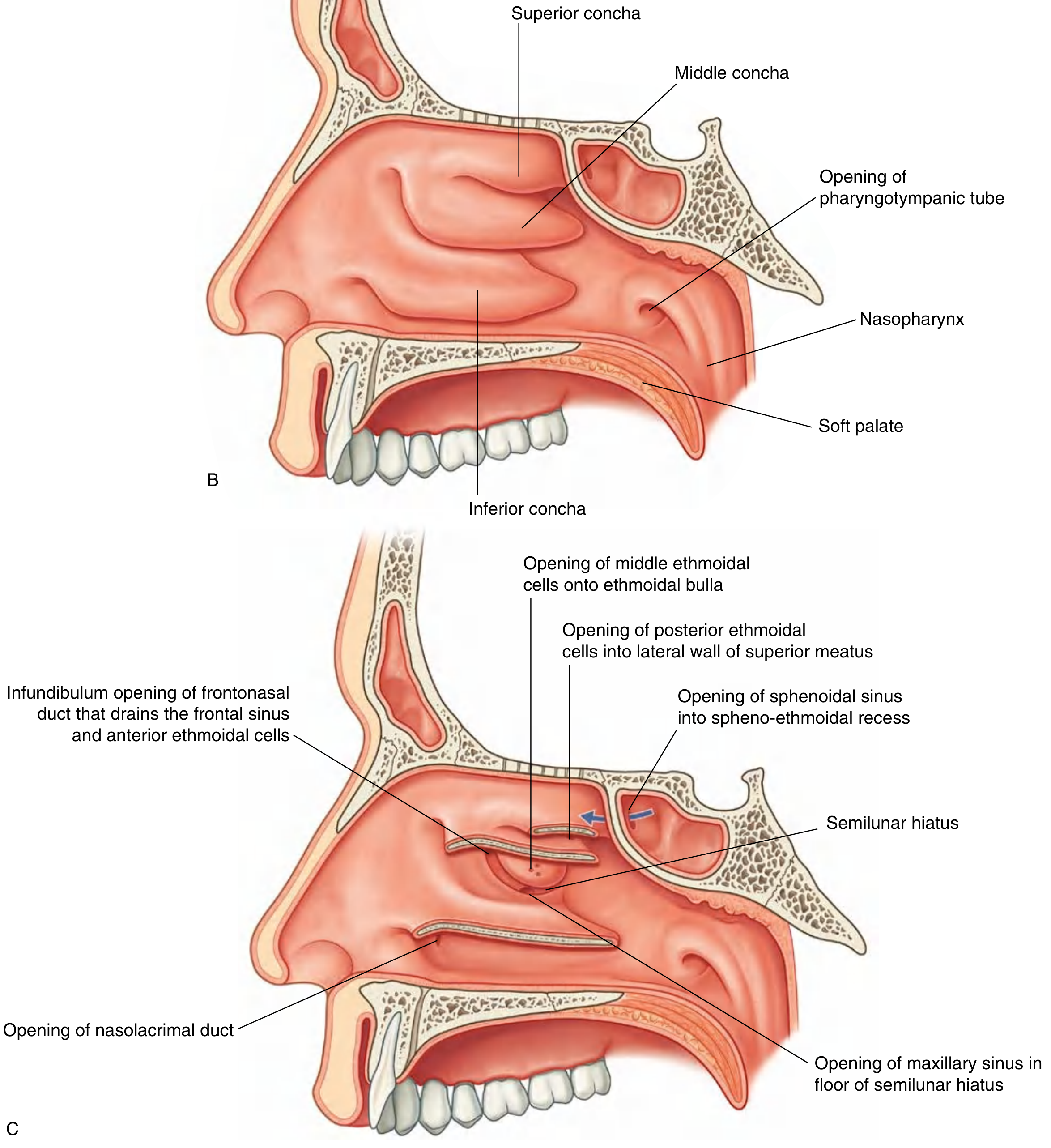
These divide the cavity into four air channels:
- Inferior meatus (below inferior concha)
- Middle meatus (below middle concha)
- Superior meatus (below superior concha)
- Spheno-ethmoidal recess (above superior concha)
The anterior end of each concha curves inferiorly to form a lip that overlies the end of the related meatus.
Important Landmarks in the Middle Meatus
- Ethmoidal bulla: dome-shaped elevation formed by underlying middle ethmoidal air cells, just below the attachment of the middle concha
- Semilunar hiatus: curved gutter inferior to the ethmoidal bulla, between the bulla above and the uncinate process below
- Ethmoidal infundibulum: funnel-shaped channel at the anterior end of the semilunar hiatus, leading upward as the frontonasal duct into the frontal sinus
Openings onto the Lateral Wall
| Structure Opening | Location |
|---|---|
| Nasolacrimal duct | Inferior meatus (under anterior lip of inferior concha) |
| Frontal sinus | Anterior end of semilunar hiatus (via frontonasal duct/infundibulum) |
| Anterior ethmoidal cells | Frontonasal duct or ethmoidal infundibulum |
| Middle ethmoidal cells | Onto or just above ethmoidal bulla |
| Maxillary sinus | Floor of semilunar hiatus (near roof of maxillary sinus) |
| Posterior ethmoidal cells | Lateral wall of superior meatus |
| Sphenoidal sinus | Spheno-ethmoidal recess (on posterior roof - NOT lateral wall) |
Key exam point: The sphenoidal sinus is the only paranasal sinus that does NOT open onto the lateral wall - it opens into the spheno-ethmoidal recess on the sloping posterior roof.
Diagrams
Quick Memory Aid for Bones (ELPSMI)
Ethmoid - Lacrimal - Palatine (perpendicular plate) - Sphenoid (medial pterygoid plate) - Maxilla - Inferior concha
Source: Gray's Anatomy for Students, p. 1217-1219
Epistaxis short answer mbbs book
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading File
I now have comprehensive textbook content from both Bailey & Love's Short Practice of Surgery and Cummings Otolaryngology. Here is the complete short answer:
Epistaxis (Nosebleed) - Short Answer
(Bailey & Love's Short Practice of Surgery, 28th ed. | Cummings Otolaryngology Head & Neck Surgery)
Definition
Epistaxis is bleeding from the nasal mucosa. It is the most common otorhinolaryngologic emergency, affecting >60% of the population at some point, with 6% requiring medical attention.
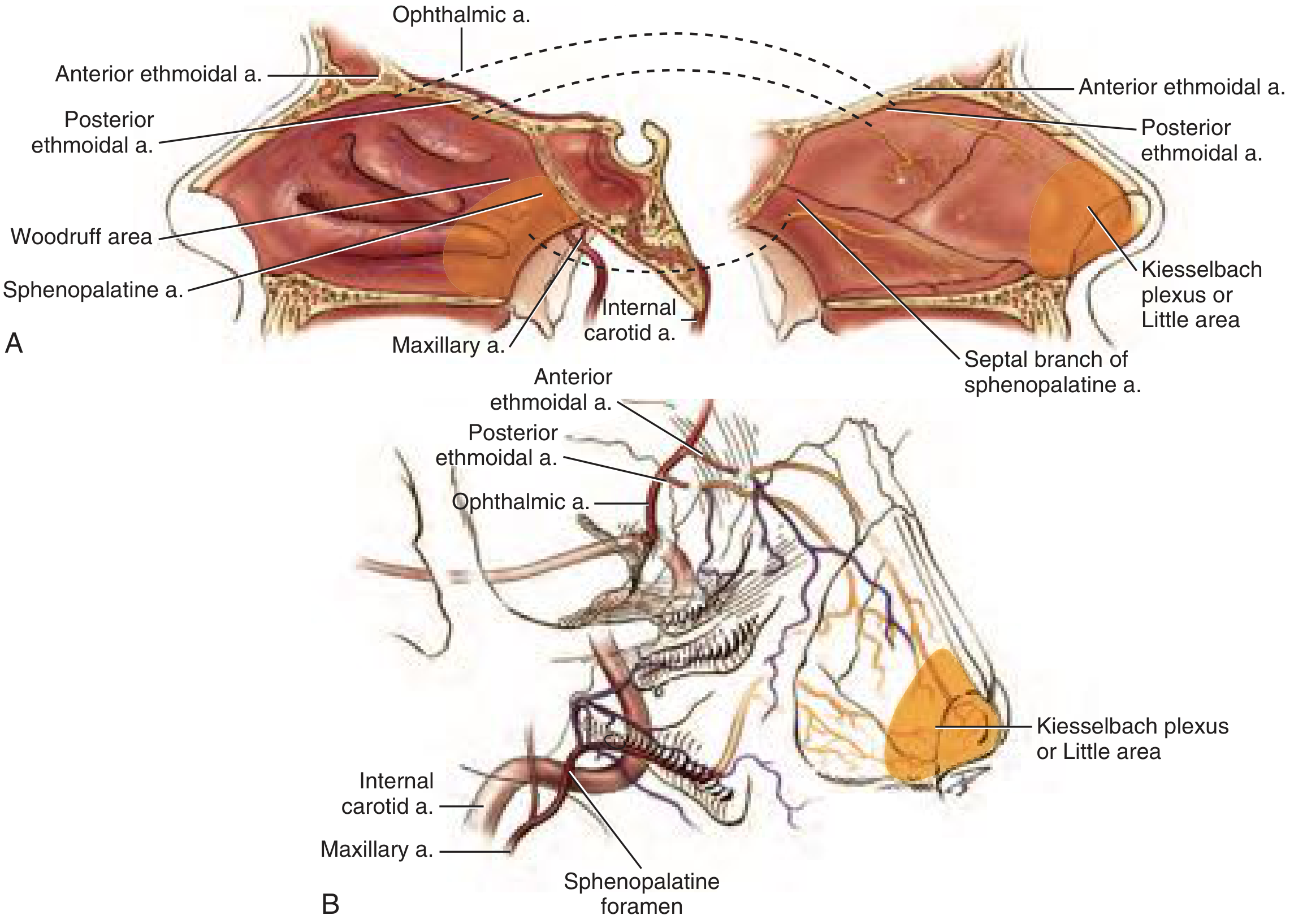
Anatomy - Sites of Bleeding
1. Anterior Epistaxis (>90% of cases)
- Bleeds from Kiesselbach's plexus (Little's area) on the anteroinferior nasal septum
- This is a vascular confluence of four arteries:
- Anterior ethmoidal artery (from internal carotid via ophthalmic)
- Sphenopalatine artery (from external carotid via maxillary)
- Greater palatine artery
- Superior labial artery
2. Posterior Epistaxis
- Bleeds from Woodruff's plexus - posterior to the inferior turbinate root
- Fed by branches of the sphenopalatine artery and ascending pharyngeal artery
- Seen in elderly patients; more severe, harder to control
Causes
Local Causes
- Nose picking (digital trauma) - most common
- Nasal trauma / fracture
- Foreign bodies
- Infection / rhinitis
- Granulomatous disorders (Wegener's, sarcoidosis)
- Tumours - Juvenile angiofibroma (adolescent boys; can cause massive bleeding)
- Hereditary haemorrhagic telangiectasia (HHT/Osler's disease)
- Septal perforation / septal deviation
Systemic Causes
- Hypertension (posterior epistaxis in elderly)
- Anticoagulants - warfarin, rivaroxaban, heparin
- Antiplatelet drugs - aspirin, clopidogrel, NSAIDs
- Bleeding disorders - haemophilia, von Willebrand disease, thrombocytopenia
- Leukaemia / lymphoma
- Liver cirrhosis, chronic kidney disease
- Cold, dry climate (mucosal drying)
Key point: Anterior epistaxis = children and young adults (nose picking). Posterior epistaxis = elderly (hypertension, anticoagulants).
Clinical Features
- Bleeding from one or both nostrils
- Blood may flow posteriorly down the throat (posterior epistaxis)
- Signs of hypovolaemia in severe cases: tachycardia, orthostatic hypotension, pallor
- First sign of acute blood loss = tachycardia
Management
Step 1 - First Aid (Conservative)
- Patient sits upright, leaning forward ("chin-to-chest" position) - prevents aspiration/swallowing of blood
- Pinch the soft cartilaginous part of the nose for 10-15 minutes
- Ice pack over forehead/face
- Topical vasoconstrictor: oxymetazoline (α1-agonist) or traditional cocaine
Step 2 - Cautery
- Silver nitrate cautery for anterior bleeding (Kiesselbach's plexus) under local anaesthesia
- Electrocautery under rigid nasendoscopy for identified posterior bleeding points
- Important: Never cauterise both sides of septum simultaneously (risk of perforation)
Step 3 - Nasal Packing
| Type | Indication | Method |
|---|---|---|
| Anterior pack | Moderate posterior bleeding | Vaseline-impregnated ribbon gauze / non-absorbable sponge / inflatable epistaxis balloon catheter |
| Posterior pack | Refractory severe bleeding | Gauze pack in nasopharynx under GA |
- Absorbable haemostatic materials (e.g., Floseal) can also be used
Step 4 - Surgical / Interventional
| Procedure | Indication |
|---|---|
| Endoscopic sphenopalatine artery ligation/clipping | Significant epistaxis not responding to cautery/packing (success rate ~97%) |
| Internal maxillary artery ligation (in pterygopalatine fossa) | Life-threatening, uncontrolled bleeding |
| Anterior & posterior ethmoidal artery ligation | If ethmoidal source identified |
| External carotid artery ligation | Above origin of lingual artery, as last resort |
| Embolisation (interventional radiology) | Alternative to surgical ligation in specific cases |
Treatment of Underlying/Predisposing Causes
| Condition | Management |
|---|---|
| Warfarin | Hold drug; give Vitamin K + FFP |
| Thrombocytopenia | Platelet transfusion (target >50,000/μL) |
| Von Willebrand disease | Desmopressin (types 1 & 2A); Factor VIII |
| Haemophilia | Factor replacement |
| Renal failure/uremia | Desmopressin; haemodialysis |
| Liver cirrhosis | FFP; monitor PT/INR |
Summary Box (Bailey & Love's Key Points)
- Most common causes: nose picking, hypertension, anticoagulant therapy
- Young people bleed from anterior septum - Kiesselbach's plexus
- Elderly bleed from posterior part of nose
- Ideally treated with direct cautery under endoscopic guidance
- Silver nitrate for anterior; packing for moderate; bilateral packing for severe
- Persistent bleeding requires endoscopic sphenopalatine artery ligation
Sources: Bailey & Love's Short Practice of Surgery 28th Ed., pp. 788-789 | Cummings Otolaryngology Head & Neck Surgery, Ch. 47
This is a shared conversation. Sign in to Orris to start your own chat.