Ecmo shirt notes
Reading File
Finding Sources
Searching the Web
ECMO extracorporeal membrane oxygenation short notes clinical indications types management
Reading File
Reading File
Reading File
Reading File
Loading Image
Here are concise short notes on ECMO:
ECMO (Extracorporeal Membrane Oxygenation) - Short Notes
Definition
ECMO (also called Extracorporeal Life Support - ECLS) is a form of prolonged cardiopulmonary bypass that provides temporary support for patients with severe, refractory cardiac and/or respiratory failure. It allows time for intrinsic recovery of the heart and lungs, or serves as a bridge to transplantation or a durable mechanical device.
Basic Circuit
The ECMO circuit consists of 4 key components:
- Inflow cannula - drains venous blood from the patient into the circuit
- Centrifugal pump - maintains blood flow through the circuit
- Membrane oxygenator - adds O₂ and removes CO₂
- Outflow cannula - returns oxygenated blood to the patient
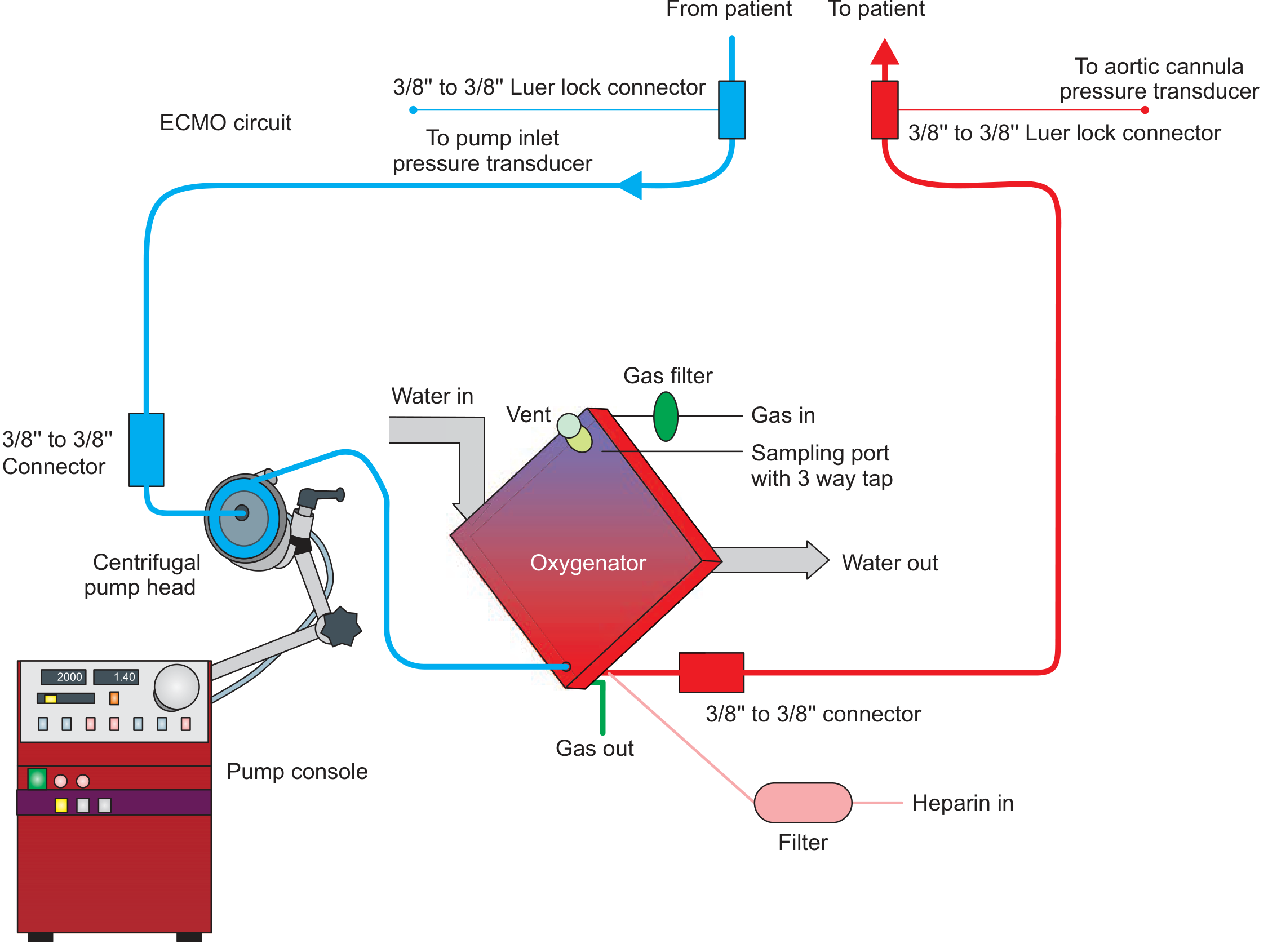
Blood is drained (blue) from patient → pump → oxygenator → returned (red) to patient. Heparin is infused continuously to prevent clotting.
Types of ECMO
| Feature | VV ECMO (Veno-Venous) | VA ECMO (Veno-Arterial) |
|---|---|---|
| Support provided | Lungs only | Heart + Lungs |
| Indications | Severe respiratory failure (ARDS, pneumonia) | Cardiogenic shock, cardiac arrest, biventricular failure |
| Cannulation | Femoral vein (inflow) + Right IJV (outflow) | Femoral/jugular vein (inflow) + Femoral/subclavian artery (outflow) |
| Cardiac output | Dependent on native cardiac output | Augments cardiac output |
| Recirculation | Can occur | Less of an issue |
Hybrid Configurations
- V-AV (Veno-Arteriovenous): Combined respiratory and partial cardiac support; used when standard VV fails to maintain oxygenation in a patient with mild cardiac dysfunction
Indications
VV ECMO (Respiratory)
- Severe ARDS (PaO₂/FiO₂ < 80 despite optimal ventilation)
- Murray Lung Injury Score > 3.0 or pH < 7.20
- Refractory hypoxemia or hypercapnia
- Bridge to lung transplantation
- COVID-19-related severe ARDS
VA ECMO (Cardiac)
- Cardiogenic shock refractory to medical therapy
- Cardiac arrest (ECPR - extracorporeal CPR)
- Acute myocarditis or myocardial stunning
- Refractory arrhythmias
- Bridge to VAD (Ventricular Assist Device) or cardiac transplant
- Post-cardiotomy shock (failure to wean from bypass)
Cannulation
Central Cannulation
- Direct cannulation of large central vessels (usually via sternotomy)
- Reserved for patients already on cardiopulmonary bypass for cardiac surgery
- Allows higher flows but carries higher bleeding and infection rates
Peripheral Cannulation
- Preferred and most common approach
- Can be performed by non-surgeons (even at bedside)
- Uses peripheral vessels (femoral, jugular)
- Preferred VV cannulation sites: Right common femoral vein (inflow) + Right IJV (outflow)
ECMO vs. Cardiopulmonary Bypass
| ECMO | CPB | |
|---|---|---|
| Duration | Days to weeks (3-10 days typical) | Hours |
| Cannulation | Often cervical (local anaesthesia) | Transthoracic (general anaesthesia) |
| Purpose | Allow intrinsic recovery | Support during cardiac surgery |
| Setting | ICU | Operating theatre |
Management on ECMO
Ventilator settings (Lung-Rest Strategy)
- Reduce ventilator support to allow injured lungs to rest
- Low tidal volumes, low PEEP, low FiO₂
Anticoagulation
- Continuous heparin infusion (circuit thrombosis prevention)
- Target ACT 180-220 seconds or anti-Xa levels per institutional protocol
- Risk of bleeding vs. thrombosis must be balanced
Cardiovascular
- Maintain systemic perfusion with inotropes/vasopressors as needed
- Echocardiography to monitor LV function and volume status
- VA ECMO can cause LV afterload increase, pulmonary oedema - may need LV unloading (IABP, Impella)
Neurological
- Avoid paralytic agents; perform regular neurological exams
- Sedation vacations to assess CNS
- Serial head ultrasounds in neonates (screen for IVH)
- Aggressive treatment of seizures (phenobarbital)
Renal
- ~60% of ECMO patients require CRRT (Continuous Renal Replacement Therapy)
- Need for CRRT is associated with significantly increased mortality (17% vs 53% 3-month survival)
Contraindications
Absolute:
- Irreversible organ failure (when ECMO cannot serve as a bridge)
- Aortic dissection (VA ECMO)
- Severe aortic regurgitation (VA ECMO)
Relative:
- Prolonged pre-ECMO CPR without adequate perfusion
- Uncontrolled bleeding or coagulopathy
- Advanced age with poor baseline functional status
Complications
| System | Complication |
|---|---|
| Hemorrhagic | Intracranial hemorrhage (most serious), cannula site bleeding, GI bleed |
| Thrombotic | Circuit thrombosis, limb ischemia, stroke |
| Cardiac | LV distension, pulmonary oedema (VA ECMO) |
| Renal | AKI requiring CRRT |
| Infectious | Line infection, sepsis |
| Circuit | Air embolism, oxygenator failure, pump failure |
Key Trials
- CESAR Trial (Peek et al., 2009): 180 adults with severe ARF. Referral to ECMO centre improved 6-month survival without severe disability (63% vs 47%) compared to conventional management.
- EOLIA Trial: RCT of VV ECMO vs conventional management in severe ARDS. Did not meet primary endpoint (60-day mortality), but high crossover rate (28%) confounded results. Bayesian reanalysis favoured ECMO.
Weaning from ECMO
- VV ECMO: Gradually reduce sweep gas flow; trial of "ECMO holiday" (clamping sweep gas while maintaining blood flow)
- VA ECMO: Gradual reduction in pump flow while monitoring haemodynamics and echo
- Decannulate when patient demonstrates ability to sustain adequate gas exchange and/or cardiac output independently
Sources: Fishman's Pulmonary Diseases and Disorders, 2-Vol Set (Ch. 149); Fischer's Mastery of Surgery, 8th ed. (p. 346)
This is a shared conversation. Sign in to Orris to start your own chat.