Now I have everything needed. Here is the complete, detailed clinical answer.
Diagnosis: Mallory-Weiss Syndrome (Mallory-Weiss Tear)
This is the most fitting diagnosis given the clinical picture: a young patient (23 years), multiple forceful vomiting episodes followed by blood in vomit (hematemesis), mild vertigo (from transient blood loss or vagal response), stable vitals (BP 130/80, SpO2 98%, PR 84) - and critically, NO history of alcoholism, drug-induced causes, blood thinners, or liver disease.
What Is It?
Mallory-Weiss syndrome is a longitudinal mucosal or submucosal laceration at the gastroesophageal junction (GEJ), caused by the shearing forces generated during forceful or repeated vomiting. The sequence is classic:
Repeated forceful vomiting → rise in intra-abdominal pressure → gastric contents reflux against the GEJ → the mucosa tears longitudinally → bright red hematemesis appears.
A common misconception is that retching must precede the bleed - in fact, a history of retching before hematemesis is present in only about one-third of cases (Symptom to Diagnosis, 4th ed.). In this patient's case, the non-bloody vomiting episodes (5-6 episodes) followed by hematemesis is the textbook sequence.
The absence of alcohol use, NSAIDs, liver disease, or coagulopathy makes varices, peptic ulcer disease, and erosive gastritis less likely, pointing strongly to a mechanical cause - the Mallory-Weiss tear.
Endoscopic Appearance
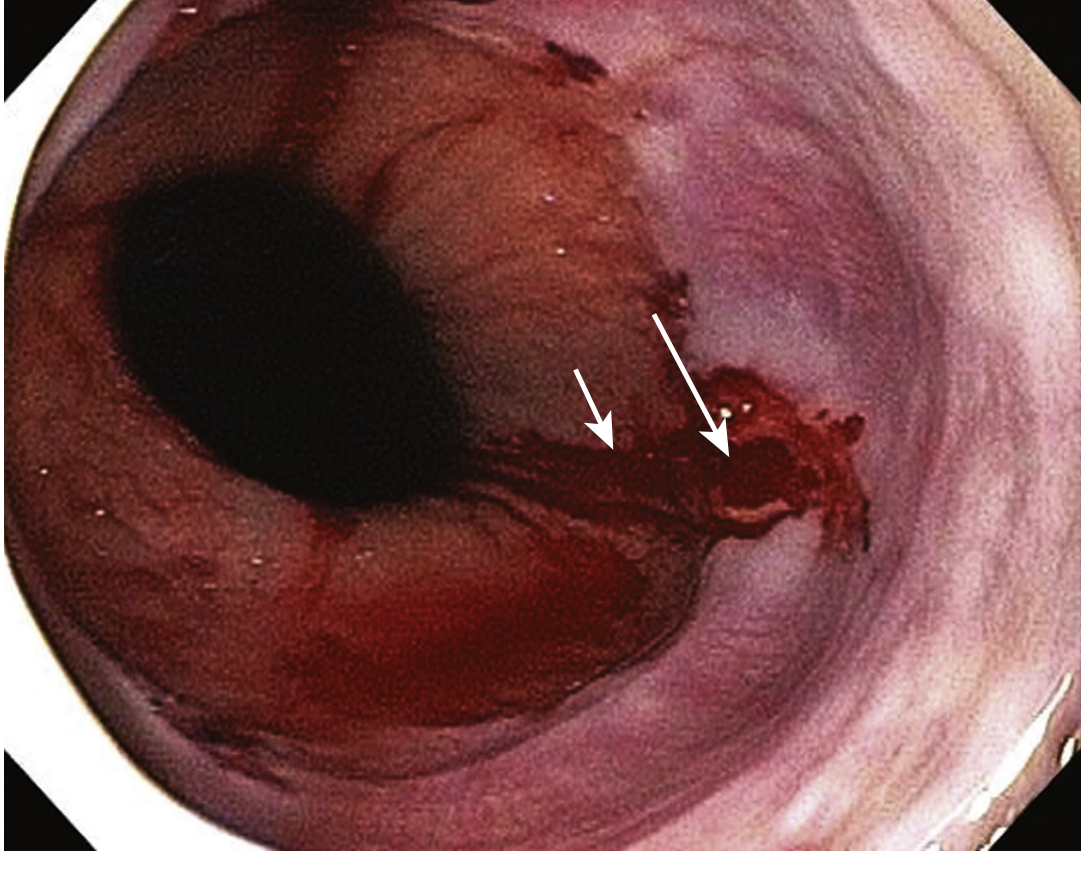
Endoscopic image showing a Mallory-Weiss tear - the tear starts at the GEJ (long arrow) and extends distally into the hiatal hernia sac (short arrow). (Sleisenger & Fordtran's Gastrointestinal and Liver Disease)
Pathophysiology
The tear results from the combination of:
- Increased intra-abdominal pressure during forceful vomiting
- Negative intrathoracic pressure above the diaphragm simultaneously
- This pressure differential shears the mucosa at the GEJ
The tear is typically single, located along the lesser curvature of the cardia, and extends a few millimeters distally. Superficial (mucosal-only) tears can begin healing within hours and heal completely within 48 hours.
Treatment
Step 1 - Stabilize and Monitor
- IV access, blood typing and crossmatch
- Vitals monitoring (this patient is currently stable)
- NPO (nil by mouth)
- Fluid resuscitation if needed
Step 2 - Pharmacological
| Drug | Role |
|---|
| IV/Oral Proton Pump Inhibitor (omeprazole, pantoprazole, esomeprazole) | Accelerates mucosal healing; suppress acid to allow clot stabilization |
| Antiemetics (ondansetron, metoclopramide) | Stop ongoing vomiting - this is critical to prevent further tearing |
| Tranexamic acid | May be considered if bleeding is significant (antifibrinolytic) |
| IV fluids / Blood transfusion | If significant blood loss (Hb monitoring needed) |
Step 3 - Endoscopy (Upper GI Endoscopy)
This is the gold standard - both diagnostic and therapeutic:
- Confirms the tear and its location
- Rules out other co-existing lesions (peptic ulcer, varices, gastritis - found in >1/3 of cases)
- If active bleeding is seen at endoscopy, endoscopic therapy is performed:
- Endoscopic hemoclip placement (preferred method)
- Epinephrine injection (1:10,000 solution)
- Multipolar electrocoagulation (MPEC)
- Band ligation
- Injection of polidocanol (sclerosant)
Important: Most Mallory-Weiss tears are self-limited (bleeding stops spontaneously in the majority). The rebleeding rate is approximately 10%, and risk factors for rebleeding include shock at presentation and active bleeding seen at endoscopy.
Step 4 - If Endoscopy Fails
- Angiographic embolization through the left gastric artery
- Surgical intervention (very rare - last resort)
(Source: Sleisenger and Fordtran's Gastrointestinal and Liver Disease; Tintinalli's Emergency Medicine)
Drugs That Are CONTRAINDICATED or Must Be AVOIDED in This Patient
These drugs must not be given to any patient with active upper GI bleeding / hematemesis:
| Drug / Drug Class | Why Contraindicated |
|---|
| NSAIDs (ibuprofen, diclofenac, naproxen, ketorolac) | Inhibit COX-1 → reduce prostaglandin-mediated mucosal protection → worsen mucosal injury and impair platelet aggregation → increase and worsen GI bleeding |
| Aspirin (all doses) | Irreversibly inhibits platelet thromboxane A2 → impairs platelet plug formation at the tear site → prolongs bleeding |
| Anticoagulants (warfarin, heparin, enoxaparin, rivaroxaban, apixaban, dabigatran) | Directly impair the coagulation cascade → prevent clot formation at the tear → uncontrollable bleeding |
| Antiplatelet agents (clopidogrel, ticagrelor, prasugrel) | Block platelet aggregation → bleeding cannot be controlled |
| Thrombolytics (streptokinase, alteplase, tenecteplase) | Lyse existing clots actively → catastrophic re-bleeding |
| Glucocorticoids (prednisolone, dexamethasone, methylprednisolone) | Reduce mucosal prostaglandin synthesis → impair mucosal repair; increase risk of GI ulceration |
| SSRIs / SNRIs (fluoxetine, sertraline, venlafaxine) | Inhibit serotonin reuptake in platelets → reduce platelet activation and aggregation → increased bleeding risk |
| Alcohol (ethanol) | Direct mucosal toxin; induces vasodilation; impairs clotting factor synthesis - if patient ever consumes it during recovery, must be stopped |
| Iron / Bismuth (these are not contraindicated for bleeding, but can mask assessment - stools turn dark, mimicking melena) | Note: these are diagnostic confounders, not causes of more bleeding |
Why NOT Peptic Ulcer Disease?
PUD is still on the differential for any young patient with hematemesis. However, PUD:
- Usually presents with epigastric pain preceding the bleed
- Is strongly associated with H. pylori or NSAID use (both absent here)
- Does not typically follow a pattern of multiple vomiting episodes followed by blood
Still, if endoscopy is done and a peptic ulcer is found, management changes (H. pylori testing, longer PPI course, biopsy).
Summary
Primary Diagnosis: Mallory-Weiss Syndrome
Confirm with: Urgent upper GI endoscopy (EGD)
Immediate Treatment: IV PPI (pantoprazole 40 mg IV) + antiemetic (ondansetron 4 mg IV) + NPO + IV access + endoscopy
Endoscopic Hemostasis: Hemoclip or epinephrine injection if active bleeding seen
Strictly Contraindicated: NSAIDs, aspirin, anticoagulants, antiplatelet drugs, thrombolytics, glucocorticoids, SSRIs/SNRIs
The prognosis in this young, hemodynamically stable patient (vitals are good: BP 130/80, SpO2 98%, PR 84) is excellent. Most tears heal within 48 hours with conservative management and a single endoscopic session.
References: Sleisenger and Fordtran's Gastrointestinal and Liver Disease; Tintinalli's Emergency Medicine: A Comprehensive Study; Symptom to Diagnosis: An Evidence-Based Guide, 4th ed.; Robbins & Cotran Pathologic Basis of Disease