detailed notes on the nasal septum
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Finding Sources
Finding Sources
I now have comprehensive material from multiple authoritative sources. Let me compile the detailed notes.
The Nasal Septum - Detailed Notes
Sources: Scott-Brown's Otorhinolaryngology Head & Neck Surgery (Vol. 1), Cummings Otolaryngology Head and Neck Surgery, Color Atlas of Human Anatomy Vol. 2, Bailey and Love's Surgery
1. Functions
The nasal septum serves multiple important roles:
- Divides the nasal airway into two distinct nasal cavities
- Supports the nasal dorsum and maintains its shape
- Maintains the shape of the columella and nasal tip
- Forms part of the internal and external nasal valves
- Contributes to laminar airflow, humidification, and filtering of inspired air
- Supports olfaction by directing airflow
Poor airflow secondary to septal pathology can impair olfaction, impair humidification and filtering, reduce oxygen delivery, and may contribute to chronic sinus disease.
2. Structural Composition
The nasal septum has three parts: bony, cartilaginous, and membranous.
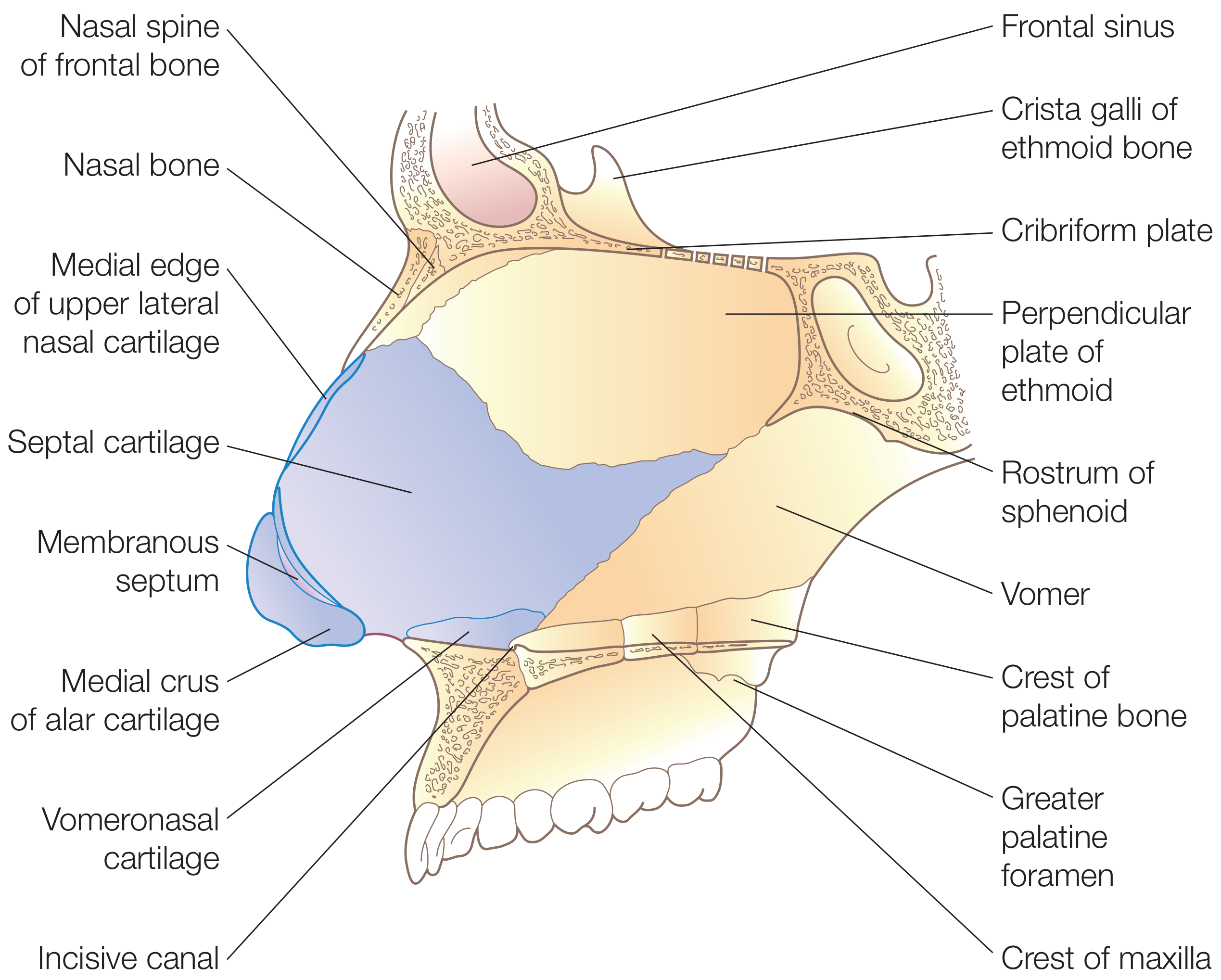
2.1 Bony Portion
| Component | Location / Articulations |
|---|---|
| Perpendicular plate of ethmoid | Forms upper one-third of septum; continuous superiorly with cribriform plate and crista galli; abuts nasal and frontal bones; articulates posteriorly with sphenoid crest, posteroinferiorly with vomer, anteroinferiorly with septal cartilage |
| Vomer | Posterior and inferior septum; two alae articulate with the sphenoid rostrum, creating vomerovaginal canals (through which pharyngeal branches of the maxillary artery travel); inferior border articulates with nasal crest of maxilla and palatine bones; anterior border articulates with septal cartilage; free posterior edge forms the posterior free margin of the septum |
| Maxillary crest | Part of the nasal crest at the floor of the nasal cavity |
| Palatine bone | Contributes to the nasal crest (horizontal plate) |
The perpendicular plate of ethmoid and nasal bones do not completely ossify until puberty - a clinically relevant point in pediatric nasal trauma.
2.2 Cartilaginous Portion - The Quadrilateral (Septal) Cartilage
- Also called the quadrilateral cartilage
- Bound firmly by collagenous fibers to the nasal bones, perpendicular plate of ethmoid, and vomer
- Continuous with the upper lateral cartilages (ULCs) toward the bridge of the nose, forming a T-shaped structure at the dorsum
- A posterior projection called the sphenoidal process (or septal tail) extends posteriorly between the vomer and perpendicular plate of ethmoid; this can serve as a source of cartilage for revision rhinoplasty
- Inferior attachment: sits within the nasal crest of the maxilla, bound by looser connective tissue creating a pseudoarthrosis - this joint allows mobility during flexion, reducing fracture or dislocation risk with trauma
2.3 Membranous Septum
- A segment of connective tissue between the caudal portion of the septal cartilage and the columella
- Not cartilaginous or bony
2.4 Vomeronasal Cartilages (Jacobson's)
- Narrow strips of cartilage located between the inferior edge of the septal cartilage and the vomer
- Remnants of the vomeronasal organs from fetal development
- Often found in conjunction with a septal spur
- Can be used as cartilage grafting material when other sources are unavailable
3. Nasal Septal Swell Body
- A widened region of the anterior nasal septum located anterior to the middle turbinate at the internal nasal valve
- Histology: increased venous sinusoids and fewer glandular elements compared to adjacent mucosa
- The high proportion of venous sinusoids suggests it can alter nasal airflow in a similar manner to the inferior turbinates
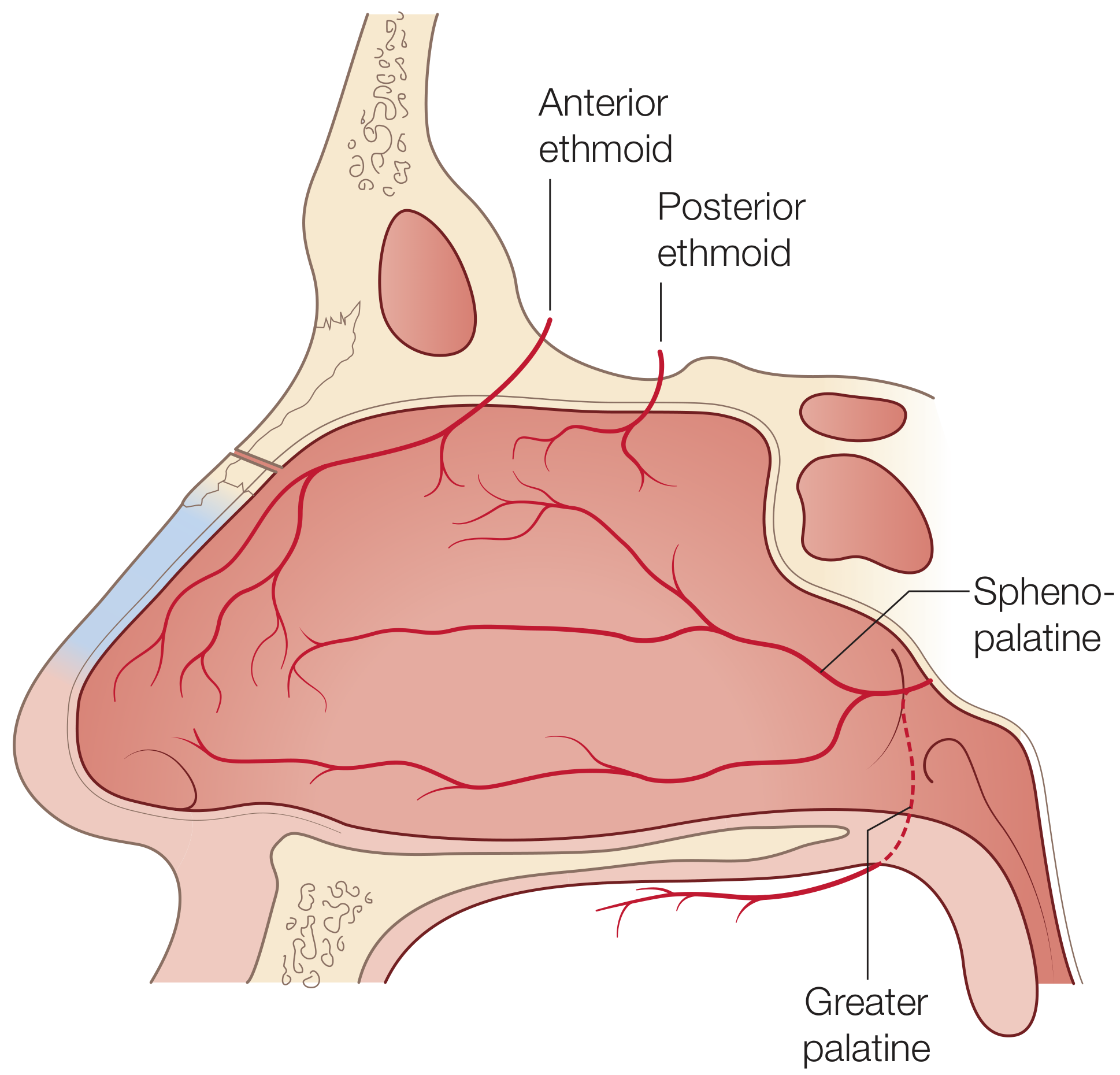
4. Blood Supply
Both the internal and external carotid arteries contribute to the septal blood supply.
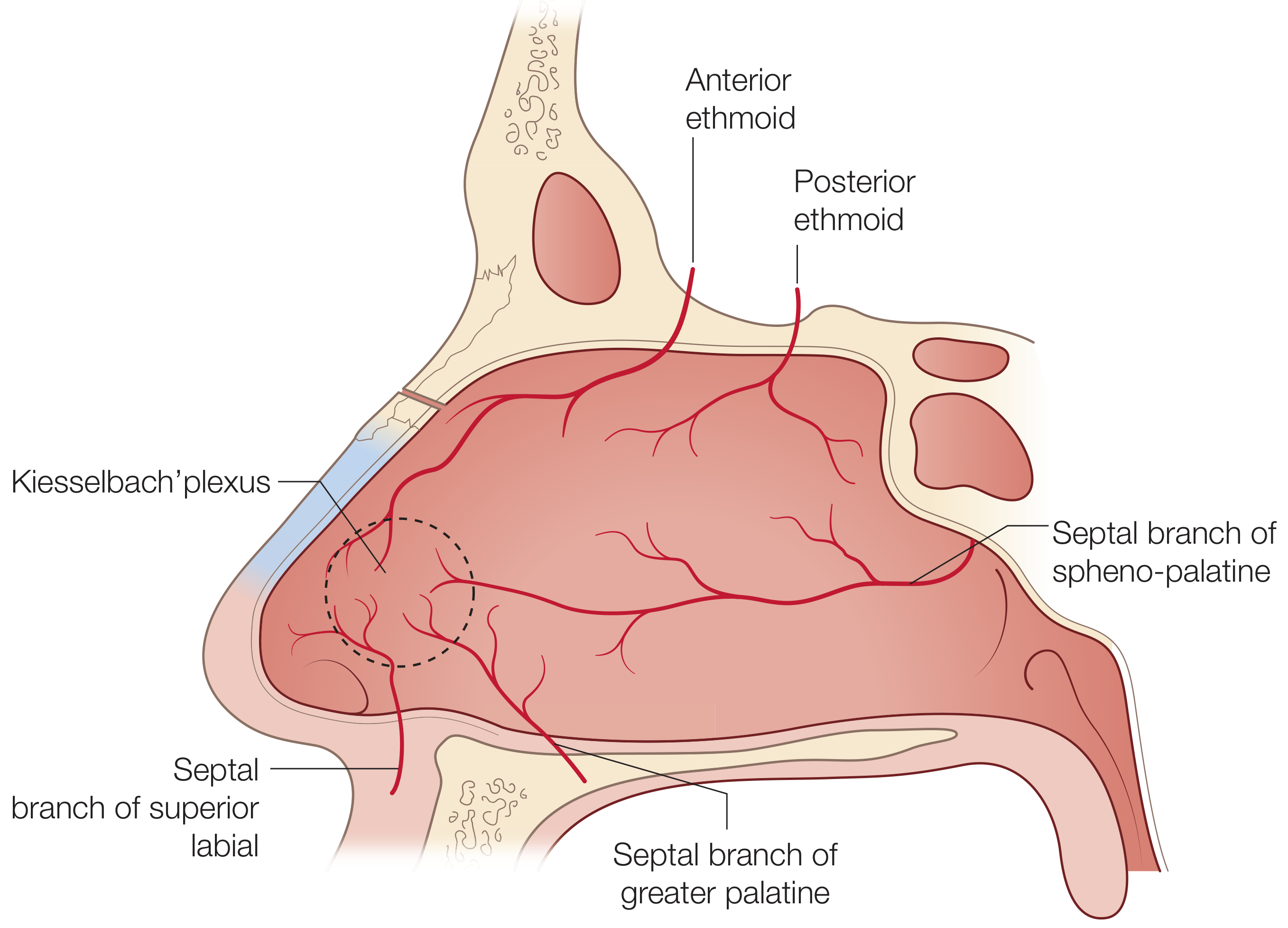
External Carotid Artery Branches (via maxillary artery)
| Artery | Region supplied |
|---|---|
| Sphenopalatine artery (posterior septal artery) | Posteroinferior septum; basis of the nasoseptal mucosal flap used in endoscopic skull base reconstruction |
| Greater palatine artery | Enters nasal cavity via the incisive canal; supplies anteroinferior septum |
| Septal branch of superior labial artery (from facial artery) | Caudal septum and columella |
Internal Carotid Artery Branches (via ophthalmic artery)
| Artery | Region supplied |
|---|---|
| Anterior ethmoid artery | Anterosuperior septum |
| Posterior ethmoid artery | Posterosuperior septum |
Kiesselbach's Plexus (Little's Area)
- Located on the anterior nasal septum
- Formed by anastomosis of the anterior ethmoid artery, posterior septal artery, and septal branch of the superior labial artery
- Rich vascular bed of long capillary loops
- Most common site of epistaxis (~90% of anterior nosebleeds) due to:
- Rich vascular supply
- Thin overlying mucosa
- Susceptibility to injury from turbulent airflow and digital trauma
Venous Drainage
- Posteriorly: via sphenopalatine vessels into the pterygoid plexus
- Anteriorly: via facial veins
- Superiorly: ethmoidal veins communicate with the superior ophthalmic system; there may be direct intracranial connections through the foramen caecum into the superior sagittal sinus (clinically important for spread of nasal sepsis)
5. Innervation
Blood supply and innervation of the septum are carried within the mucoperiosteal (over bone) and mucoperichondrial (over cartilage) linings.
Sensory Innervation (Trigeminal Nerve)
- V1 (Ophthalmic): anterior and superior septum via branches of the nasociliary nerve (nasal branches)
- V2 (Maxillary): posterior septum via the nasopalatine nerve (CN V2), which runs through the incisive canal to the palate; provides sensation to the posteroinferior septum
Autonomic Innervation
- Parasympathetic: preganglionic fibers travel via CN VII → greater superficial petrosal nerve → joins deep petrosal nerve → vidian nerve → synapse in the sphenopalatine ganglion → postganglionic fibers innervate nasal mucosa (regulate secretions and vasodilation)
- Sympathetic: postsynaptic fibers pass through the sphenopalatine ganglion → nasal mucosa (regulate vasoconstriction, turbinate tone)
- The autonomic system regulates vascular tone, turbinate congestion, and nasal secretions
6. Mucosa
The nasal septal mucosa has two distinct regions:
| Region | Location | Lining | Function |
|---|---|---|---|
| Respiratory region | Opposite inferior and middle conchae | Pseudostratified ciliated (respiratory) epithelium | Humidification, filtration; cilia beat toward pharynx; well-developed cavernous plexus (erectile tissue) |
| Olfactory region | Upper nasal septum where it meets cribriform plate | Olfactory epithelium | Olfaction |
The anterior cavernous plexus is usually identifiable as mucosal thickening and is the most frequent site of epistaxis.
7. Embryology
- Nasal airway development begins at week 4 of gestation from neural crest cell proliferation forming nasal placodes
- The nasal septum develops as a downgrowth from the merged medial nasal processes and nasofrontal process
- Nasal septum and palatine processes begin fusing anteriorly at week 9; fusion is completed posteriorly by week 12
- The vomeronasal (Jacobson's) organs form as epithelial invaginations on either side of the septum; they begin to regress shortly before birth, leaving the vomeronasal cartilages as adult remnants
- Injury in young children can cause asymmetric growth of the entire nasal structure due to chondrocyte growth interruption
8. Deviated Nasal Septum
- Extremely common - in adults the septum very frequently deviates from the midline, particularly at the junction of the cartilaginous and bony portions (where the vomeronasal cartilage lies)
- Most common cause of unilateral nasal airway obstruction
Causes
- Birth trauma (forceps delivery, passage through narrow pelvic canal)
- Nasal/midfacial trauma at any age
- Microfractures early in life heal with bending of cartilage away from the side of injury
- Developmental abnormalities
Clinical Features
- Nasal obstruction (unilateral or bilateral)
- Paradoxical nasal obstruction: some patients feel obstruction on the contralateral (more open) side, because the turbinate there may be hypertrophied as compensation
- Compensatory turbinate hypertrophy on the side contralateral to the deviation
- Impaired olfaction
- Chronic sinusitis
- Possible external nasal deformity
- Epistaxis (from secondary turbulent airflow causing mucosal drying and septal varices)
Nasal Cycle Interaction
- The nasal cycle is a normal alternating congestion of the two sides, cycling every 0.5-3 hours under sympathetic control
- In patients with a fixed septal deviation, the sensation of obstruction frequently mirrors the congestion phase of the cycle
9. Clinical Relevance - Key Surgical Points
L-Strut Principle
In septoplasty, the surgeon classically preserves at least a 1 cm dorsal and 1 cm caudal segment of septal cartilage (the "L-strut") to prevent loss of dorsal and tip support.
Septal Perforation
- Recognized complication of septoplasty
- Prevention requires meticulous mucoperichondrial dissection; any bilateral membrane tears should be repaired with an interposition graft of crushed cartilage placed between flaps
- Causes include: iatrogenic, cocaine abuse, granulomatous disease (e.g., Wegener's/GPA, sarcoidosis), syphilis, trauma
Incisive Neurovascular Bundle
- A variably located incisive artery and its neural fibers are found at the inferior border of the vomer
- Relevant when trimming a badly deviated maxillary crest - injury may cause temporary numbness or pain of the central incisors or hard palate mucosa
Cottle Maneuver
- Gently pulling the cheek laterally to open the nasal valve; a positive test suggests nasal valve compromise, though it has many false positives
- More specific: gentle lateralization of the ULC with a cotton-tipped applicator or cerumen curette
Nasoseptal Flap
- Based on the posterior septal artery (branch of sphenopalatine artery)
- The workhorse pedicled flap for endoscopic anterior skull base reconstruction
10. Summary Diagram of Arterial Supply
| Artery | Origin | Region of Septum |
|---|---|---|
| Anterior ethmoid a. | Ophthalmic a. (ICA) | Anterosuperior |
| Posterior ethmoid a. | Ophthalmic a. (ICA) | Posterosuperior |
| Posterior septal a. (sphenopalatine) | Internal maxillary a. (ECA) | Posteroinferior |
| Greater palatine a. | Internal maxillary a. (ECA) | Anteroinferior (via incisive canal) |
| Septal br. of superior labial a. | Facial a. (ECA) | Caudal septum / columella |
| Kiesselbach's plexus | Anastomosis of anterior ethmoid + posterior septal + superior labial | Anterior septum (Little's area) |
Sources: Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 1 (p. 1014-1015), Cummings Otolaryngology Head and Neck Surgery (pp. 564-568), Color Atlas of Human Anatomy Vol. 2 (p. 178), Bailey and Love's Short Practice of Surgery 28th ed.
detailed notes on lateral wall of nose
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
I now have comprehensive data from all major sources. Let me compile the full detailed notes.
Lateral Wall of the Nose - Detailed Notes
Sources: K.J. Lee's Essential Otolaryngology, Scott-Brown's Otorhinolaryngology Head & Neck Surgery (Vol. 1), Cummings Otolaryngology Head and Neck Surgery
1. Osteology (Bones Forming the Lateral Nasal Wall)
Listed from anterior to posterior:
| Bone | Notes |
|---|---|
| Frontal process of maxilla | Forms the anterior part; site of anterior lacrimal crest |
| Lacrimal bone | Small, thin bone; posterior lacrimal crest formed here; articulates with frontal process of maxilla at the lacrimal (maxillary) line |
| Medial wall of maxilla (inferiorly) | Forms the inferior half of the lateral wall; also forms the medial wall of the maxillary sinus |
| Lamina papyracea (superiorly) | The "paper-thin" orbital plate of the ethmoid; forms the lateral wall of the ethmoid labyrinth |
| Perpendicular plate of palatine bone | Posterior part; contributes to the sphenopalatine foramen |
| Medial pterygoid plate of sphenoid | Most posterior; also contributes to sphenopalatine foramen |
The sphenopalatine foramen is formed by the perpendicular plate of the palatine bone together with the sphenoid bone - it is the principal neurovascular gateway to the nasal cavity.
2. The Five Lamellae of the Lateral Nasal Wall
From anterior to posterior, the lateral wall is organised into five bony lamellae (vertical sheets):
| Lamella | Structure |
|---|---|
| 1st | Uncinate process (UP) |
| 2nd | Ethmoid bulla (EB) |
| 3rd | Basal (ground) lamella of middle turbinate (MT) |
| 4th | Basal lamella of superior turbinate |
| 5th | Basal lamella of supreme turbinate (when present) |
The basal lamella of the middle turbinate is the key surgical landmark dividing the anterior from the posterior ethmoid sinuses.
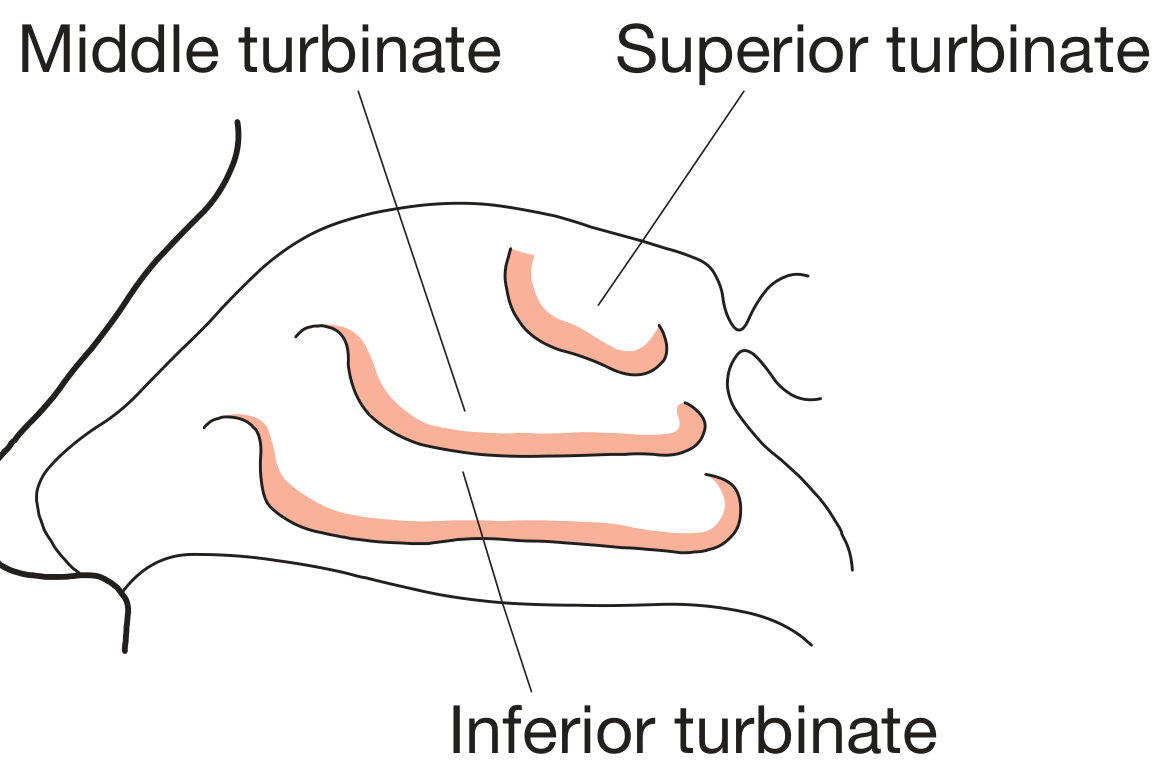
3. Turbinates (Conchae)
Turbinates are shelves of bone encased in erectile (vascular) mucosa capable of altering the nasal airway cross-sectional area.
3.1 Overview
- Inferior, middle, superior, and occasionally supreme turbinate
- All turbinates originate from the ethmoid bone - except the inferior turbinate, which is an embryologically independent osseous structure (its own bone)
- Each turbinate creates a corresponding meatus (air space below and lateral to it)
3.2 Inferior Turbinate
- Largest turbinate; the most important for airflow resistance
- An independent bone (not part of the ethmoid)
- Lies along the inferior lateral wall; head is ~1 cm posterior to the nasal vestibule
- The nasolacrimal duct opens into the inferior meatus approximately 1 cm posterior to the anterior face of the inferior turbinate (at Hasner's valve)
- Contains a rich venous sinusoidal network (erectile tissue)
- Participates in the nasal cycle
- Compensatory hypertrophy occurs contralateral to a deviated nasal septum
3.3 Middle Turbinate (MT)
The middle turbinate has three sites of attachment in three different planes - a key surgical concept:
| Part | Plane | Attachment |
|---|---|---|
| Anterior | Sagittal | Junction of cribriform plate and lateral lamella - delimits the fovea ethmoidalis (roof of ethmoid) from the cribriform plate |
| Middle (basal/ground lamella) | Coronal (vertical) | Lateral attachment to lamina papyracea - divides anterior from posterior ethmoid sinuses |
| Posterior | Axial (horizontal) | Crista ethmoidalis of the perpendicular plate of palatine bone, just anterior to the sphenopalatine foramen |
- Anterior end attaches to the frontal process of maxilla, forming the axilla of the MT
- The posterior horizontal attachment is a potential site of postoperative epistaxis if the MT is resected; its preservation reduces risk of postoperative MT lateralization
Variants of the middle turbinate:
| Variant | Description |
|---|---|
| Concha bullosa | Pneumatization of the MT; present in ~1/3 of the population; can narrow the middle meatus and contribute to recurrent sinusitis |
| Paradoxical MT | The lateral surface of the MT is convex rather than concave (reversed curvature) |
3.4 Superior (and Supreme) Turbinate
- Arises from the ethmoid bone
- The superior turbinate forms the lateral wall of the sphenoethmoidal recess (SER)
- A supreme turbinate may be present (5th lamella)
4. Meatuses and Their Drainage
The meatus is the air space located beneath and lateral to the turbinate of the same name.
| Meatus | Location | Drains |
|---|---|---|
| Inferior meatus | Below inferior turbinate | Nasolacrimal duct (via Hasner's valve, ~1 cm posterior to anterior face of inferior turbinate) |
| Middle meatus | Below middle turbinate | Frontal sinus, anterior ethmoid cells, maxillary sinus |
| Superior meatus | Below superior turbinate | Posterior ethmoid cells |
| Sphenoethmoidal recess (SER) | Posterosuperior, between superior turbinate and nasal septum | Sphenoid sinus |
5. Key Endoscopic Landmarks
5.1 Uncinate Process (UP)
- Crescent-shaped, mucosa-lined bone of ethmoid origin
- Shields the natural ostium of the maxillary sinus
- Vertical portion attaches anteriorly to the lacrimal (maxillary) line
- Horizontal portion attaches inferiorly to the inferior turbinate
- May narrow the ethmoid infundibulum if pneumatized
Site of superior attachment of the UP determines frontal sinus drainage:
| Superior attachment | Drainage path | Frequency |
|---|---|---|
| To lamina papyracea | Frontal sinus drains medial to UP, directly into middle meatus; forms a blind superior pouch = Recessus Terminalis | ~80% (most common) |
| To fovea ethmoidalis or MT | Frontal sinus drains lateral to UP, into the ethmoid infundibulum | ~20% |
5.2 Ethmoid Infundibulum
- A three-dimensional trough/channel
- Bounded by: UP medially, lamina papyracea laterally, ethmoid bulla posterosuperiorly
- Opens inferiorly at the maxillary sinus ostium
5.3 Hiatus Semilunaris
- A two-dimensional crescentic window (slit) opening into the ethmoid infundibulum
- Bounded anteriorly by the UP and posteriorly by the ethmoid bulla
5.4 Ethmoid Bulla (EB)
- Second lamella; the largest and most consistent anterior ethmoid cell
- Forms the posterior boundary of the hiatus semilunaris
5.5 Lacrimal (Maxillary) Line
- Endoscopic landmark: the suture line along the medial orbital wall at the junction of the frontal process of maxilla and the lacrimal bone
- Site of attachment of the UP to the lateral nasal wall
- Divides the anterior lacrimal crest (maxilla) from the posterior lacrimal crest (lacrimal bone)
5.6 Nasal Fontanelles
- Areas of bony dehiscence of the lateral nasal wall covered only by mucosa and connective tissue (no bone)
- Posterior fontanelle: located posterior to the horizontal process of the UP, posterior to the natural maxillary ostium (oriented sagittally vs. the oblique natural ostium) - site of accessory ostia in up to 30% of people
- Anterior fontanelle: located anterior to the UP articulation with the inferior turbinate
6. Osteomeatal Complex (OMC)
A functionally important region within the middle meatus - the final common drainage pathway for the majority of the paranasal sinuses.
Boundaries:
| Wall | Structure |
|---|---|
| Posterior | Basal lamella of middle turbinate |
| Medial | Middle turbinate |
| Lateral | Lamina papyracea |
| Superior | Fovea ethmoidalis |
Clinical significance: The OMC is central to the pathophysiology of acute bacterial rhinosinusitis. Obstruction of the OMC (by mucosal edema, polyps, anatomical variants) impairs drainage and ventilation of the frontal, anterior ethmoid, and maxillary sinuses, predisposing to infection.
7. Nasolacrimal System
Intimately related to the lateral nasal wall. Tear drainage pathway:
Upper/lower lacrimal punctum → Upper/lower canaliculus → Common canaliculus (present in 90%) → Valve of Rosenmuller (one-way, prevents reflux) → Lacrimal sac → Nasolacrimal duct → Valve of Hasner → Inferior meatus
Lacrimal fossa (bony recess containing lacrimal sac):
- Anterior wall: anterior lacrimal crest (frontal process of maxilla)
- Posterior wall: posterior lacrimal crest (lacrimal bone)
- The suture between these corresponds to the lacrimal line
Lacrimal sac: ~0.9 cm above the axilla of the MT and ~0.5 cm above the common canaliculus - important for adequate exposure during dacryocystorhinostomy (DCR).
8. Blood Supply of the Lateral Nasal Wall
Both the internal and external carotid arteries contribute.
External Carotid Artery (via Internal Maxillary Artery)
| Artery | Route/Region |
|---|---|
| Sphenopalatine artery (SPA) | Enters via sphenopalatine foramen (SPF); major supply to turbinates and lateral wall |
| - Posterior lateral nasal branch | Runs along middle and inferior turbinates |
| - Posterior septal branch | Courses along sphenoid rostrum; supplies nasal septum (basis of nasoseptal flap) |
| Greater palatine artery | Via greater palatine canal → incisive foramen; supplies anteroinferior nasal cavity |
| Pharyngeal branch (palatovaginal a.) | Via pharyngeal canal; supplies posterosuperior nasal cavity and nasopharynx |
| Facial artery branch | Small area along anterior lateral nasal wall |
Sphenopalatine foramen (SPF) details:
- Located within the superior meatus, between the basal lamella of the MT and superior turbinate
- Lies just inferior to the horizontal attachment of the middle turbinate
- The crista ethmoidalis (a crest on the perpendicular plate of the palatine bone) lies just anterior to the SPF - a consistent, reliable endoscopic landmark for identifying and ligating the SPA
- In one cadaver study, 97% of specimens had two or more branches of the SPA medial to the crista ethmoidalis - surgeons must control all branches for successful endoscopic ligation
Internal Carotid Artery (via Ophthalmic Artery)
| Artery | Key details |
|---|---|
| Anterior ethmoid artery (AEA) | Larger than PEA; exits orbit via anterior ethmoid foramen (~24 mm posterior to anterior rim of lacrimal fossa, within frontoethmoid suture); courses anteromedially along skull base in a bony canal (dehiscent in ~40%) or mucosal mesentery; delineates the posterior limit of the frontal recess; enters anterior cranial fossa via lateral lamella (weakest part of skull base); supplies anterior 1/3 of nasal cavity |
| Posterior ethmoid artery (PEA) | Exits orbit via posterior ethmoid foramen (~12 mm posterior to AEA, 6 mm anterior to optic ring); supplies posterior nasal cavity |
Surgical access to ethmoid arteries:
- The AEA is difficult to access endoscopically - only ~20% lie in a mesentery that can be clipped transnasally
- Endoscopic removal of the lamina papyracea allows identification of both arteries between the periorbita and skull base
- Alternatively, an external approach via a modified Lynch incision is used
There is considerable overlap between internal and external carotid arterial systems on each side - this can complicate arterial ligation for epistaxis management.
9. Innervation of the Lateral Nasal Wall
Sensory (Trigeminal Nerve)
| Nerve | Division | Region supplied |
|---|---|---|
| Internal nasal branch of anterior ethmoid nerve | V1 | Anterior and superior nasal cavity (lateral wall and septum) |
| Posterior ethmoid nerve | V1 | Posterior nasal cavity |
| Posterolateral nasal nerves (from sphenopalatine foramen) | V2 | Lateral wall and turbinates |
| Nasopalatine nerve | V2 | Posterior septum → incisive canal → palate |
| Anterior superior alveolar nerve | V2 | Anterior nasal floor |
The lateral wall of the nose and turbinates are specifically supplied by posterolateral nasal nerves from V2 arising from the sphenopalatine foramen and ethmoidal nerves from V1.
Autonomic Innervation
| System | Function | Pathway |
|---|---|---|
| Sympathetic | Vasoconstriction; regulates vascular tone and turbinate congestion | Sympathetic chain → superior cervical ganglion → deep petrosal nerve → joins GSPN → vidian nerve → passes through sphenopalatine ganglion without synapsing → nasal mucosa |
| Parasympathetic | Vasodilation; mediates nasal secretions | Superior salivary nucleus (CN VII) → nervus intermedius → GSPN → geniculate ganglion → vidian nerve → synapse in sphenopalatine ganglion → postganglionic fibers with V2 branches → nasal mucosa |
Key distinction: Parasympathetic fibers synapse in the sphenopalatine ganglion; sympathetic fibers pass through without synapsing.
10. Mucosa and Epithelium
Three types of epithelium are found in the nasal cavity:
| Type | Location |
|---|---|
| Squamous epithelium | Nasal vestibule |
| Olfactory epithelium | Superior septum, superior turbinate, upper aspect of middle turbinate |
| Respiratory (pseudostratified ciliated) epithelium | Remainder of nasal cavity (most of the lateral wall) |
11. Nasal Cycle
- A normal physiological alternating congestion of the two sides of the nasal cavity
- Cycle repeats every 0.5-3 hours under sympathetic nervous system control
- Total nasal resistance remains approximately constant as one side congests and the other decongests
- Turbinates are the primary structures involved (via their venous sinusoidal erectile tissue)
- Clinically relevant: in patients with a fixed septal deviation, nasal obstruction symptoms frequently fluctuate with the nasal cycle
12. Clinical Summary Table
| Structure | Key Clinical Point |
|---|---|
| Middle meatus | Common drainage pathway for frontal, anterior ethmoid, maxillary sinuses - obstruction causes sinusitis |
| Osteomeatal complex | Pathophysiological hub in acute bacterial rhinosinusitis |
| Concha bullosa | Present in ~1/3 of people; can obstruct middle meatus and cause recurrent sinusitis |
| Sphenopalatine artery | Major blood supply; crista ethmoidalis = endoscopic landmark for ligation in posterior epistaxis |
| Anterior ethmoid artery | Only ~20% accessible endoscopically in a mesentery; external (Lynch) approach often preferred for ligation |
| Hasner's valve | Nasolacrimal duct opens here in inferior meatus; may cause epiphora if blocked |
| Lamina papyracea | Thin orbital plate; breach during FESS risks orbital injury/fat herniation |
| Nasal fontanelles | Areas of bony dehiscence in lateral wall; site of accessory maxillary ostia (~30% of people have posterior fontanelle accessory ostium) |
Sources: K.J. Lee's Essential Otolaryngology (pp. 511-518), Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 1 (pp. 1015-1016), Cummings Otolaryngology Head and Neck Surgery
structres opening into the lateral wall of the nasal cavity
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Loading Image
Finding Sources
I now have all the information needed. Let me compile thorough, well-organised notes.
Structures Opening into the Lateral Wall of the Nasal Cavity
Sources: Cummings Otolaryngology, Scott-Brown's Otorhinolaryngology (Vol. 1), Bailey and Love's Surgery, K.J. Lee's Essential Otolaryngology
Overview Diagram
Quick Reference Table
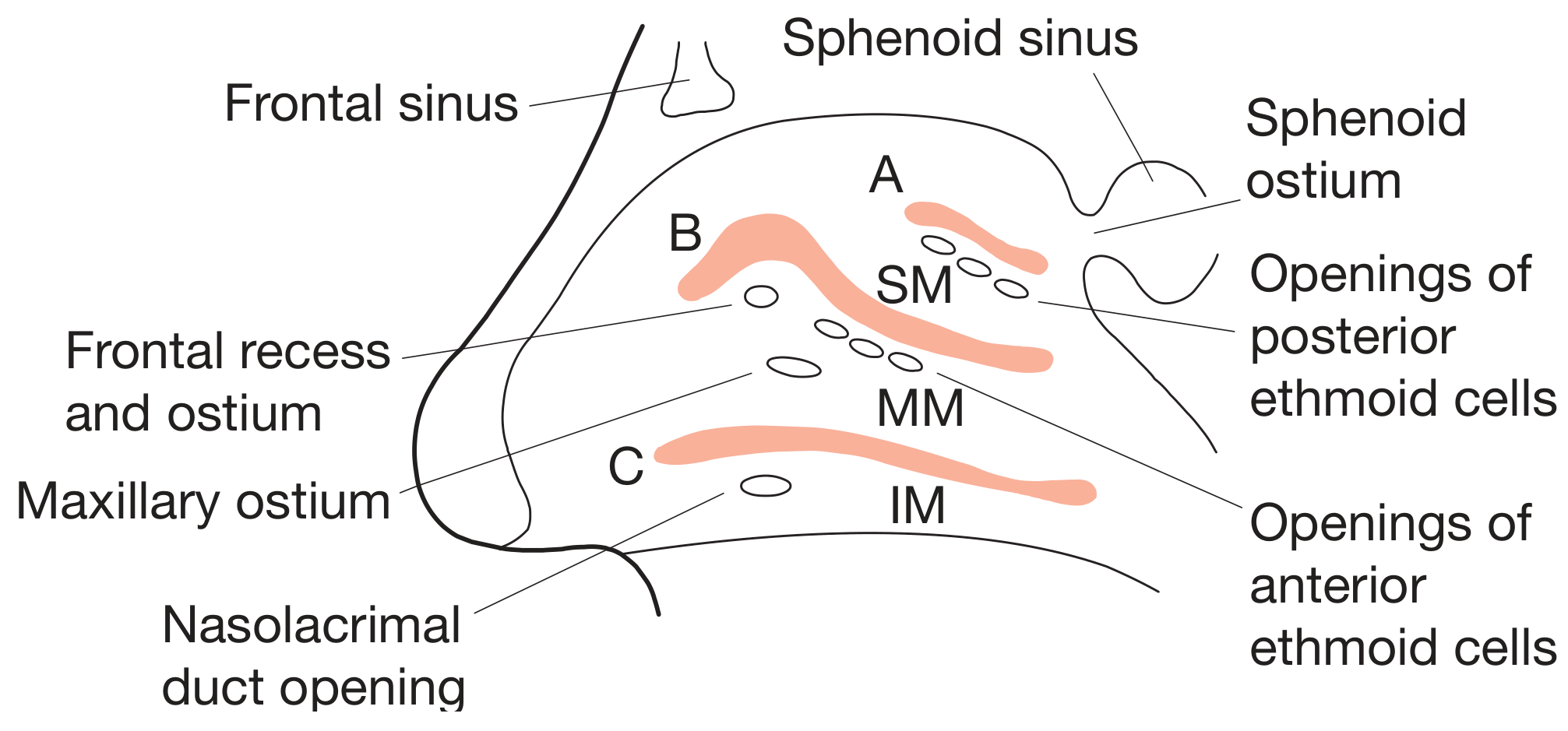
| Meatus / Region | Structure Opening Into It |
|---|---|
| Inferior meatus | Nasolacrimal duct (via valve of Hasner) |
| Middle meatus | Maxillary sinus (via maxillary ostium → ethmoid infundibulum → hiatus semilunaris); Frontal sinus (via frontal recess); Anterior ethmoid cells (via their ostia) |
| Superior meatus | Posterior ethmoid cells |
| Sphenoethmoidal recess | Sphenoid sinus (via sphenoid ostium) |
1. Inferior Meatus
The air space below and lateral to the inferior turbinate.
Nasolacrimal Duct (NLD)
- Opens into the anterior part of the inferior meatus
- Located approximately 1 cm posterior to the anterior face of the inferior turbinate
- The opening is guarded by the Valve of Hasner - a mucosal fold that acts as a one-way valve preventing air reflux into the lacrimal system (not a true valve anatomically)
- The full tear drainage pathway is: upper/lower punctum → canaliculus → common canaliculus → Valve of Rosenmuller → lacrimal sac → nasolacrimal duct → Valve of Hasner → inferior meatus
- Clinical note: Congenital obstruction of the NLD most commonly occurs at the Valve of Hasner; presents as epiphora and mucopurulent discharge in neonates. Nasolacrimal duct cysts (dacryocystoceles) may appear in the inferior meatus as a bluish cystic mass, causing nasal obstruction.
Nothing else drains into the inferior meatus - this is a frequently tested fact.
2. Middle Meatus
The most important and complex meatus - the air space below and lateral to the middle turbinate. It is the final common drainage pathway for three major paranasal sinuses.
2.1 Frontal Sinus
Drains into the superior part of the middle meatus via the frontal recess - the most complex of the drainage pathways.
The frontal sinus outflow tract (FSOT) follows an hourglass-shaped pathway:
Frontal sinus
↓
Funnel-shaped infundibulum (within the frontal sinus)
↓
Frontal ostium (the waist of the hourglass)
↓
Frontal recess (the "1st tight spot" - narrowest part)
↓
Superior portion of middle meatus
Frontal recess boundaries:
- Anterior: agger nasi cell (most anterior ethmoid cell, present in most individuals)
- Posterior: ethmoid bulla
- Inferior: uncinate process (and its superior attachment determines whether drainage is medial or lateral to it)
- Medial: middle turbinate
Note: If the agger nasi is large, it may directly impair patency of the frontal recess and block frontal sinus drainage.
2.2 Maxillary Sinus
Drains into the middle meatus via the following sequential path:
Maxillary sinus
↓
Maxillary sinus ostium (natural ostium - located in superior medial wall of sinus)
↓
Ethmoidal infundibulum (3D trough; bounded by UP medially, lamina papyracea laterally, ethmoid bulla posterosuperiorly) - the "2nd tight spot"
↓
Hiatus semilunaris (2D crescentic window between UP anteriorly and ethmoid bulla posteriorly)
↓
Middle meatus
Key surgical point: Not incorporating the true (natural) maxillary sinus ostium into a surgical antrostomy is the most common cause of failure of a maxillary antrostomy. Accessory ostia (present in the posterior fontanelle in ~20-25% of patients) must be identified and connected to the natural ostium to prevent mucus recirculation - where mucus swept out of the natural ostium by cilia re-enters through the accessory ostium.
2.3 Anterior Ethmoid Cells
- The anterior ethmoid air cells drain into the middle meatus via their individual ostia, which open into the ethmoid infundibulum
- The ethmoid bulla (the largest and most consistent anterior ethmoid cell) drains superiorly into the suprabullar recess or directly into the middle meatus
The two ostiomeatal channels (Cummings classification):
| Channel | Components | Sinuses Served |
|---|---|---|
| Anterior ostiomeatal unit | Frontal sinus ostium + frontal recess + maxillary ostium + infundibulum + middle meatus | Frontal, anterior ethmoid, maxillary |
| Posterior ostiomeatal unit | Sphenoid ostium + sphenoethmoidal recess + superior meatus | Sphenoid, posterior ethmoid |
3. Superior Meatus
The air space below and lateral to the superior turbinate.
Posterior Ethmoid Cells
- All posterior ethmoid air cells drain into the superior meatus
- The superior turbinate forms the lateral wall of the sphenoethmoidal recess (SER)
4. Sphenoethmoidal Recess (SER)
A narrow recess located posterosuperiorly, between the superior turbinate laterally and the nasal septum medially. It is above and posterior to the superior meatus.
Sphenoid Sinus
- The sphenoid ostium opens into the sphenoethmoidal recess, behind (not medial or lateral to) the superior turbinate
- Located in the anterosuperior portion of the anterior sphenoid sinus wall, situated medially
- This constitutes the "3rd tight spot" of sinonasal drainage
- The sphenoethmoidal recess in turn leads to the posterior aspect of the superior meatus
- A supreme turbinate, when present, may also be visible here
Sphenoid sinus ostium - precise location:
- Approximately 30 mm from the anterior nasal spine
- Approximately 1.5 cm above the posterior choana
- Can also be found ~7 mm above the choanal arch, 1 cm from the nasal septum
5. Summary by Sinus
| Sinus | Ostium Location | Drainage Route | Ultimate Opening |
|---|---|---|---|
| Frontal | Medial floor of frontal sinus | Frontal ostium → frontal recess | Middle meatus (superior part) |
| Maxillary | Superior medial wall of sinus | Maxillary ostium → ethmoidal infundibulum → hiatus semilunaris | Middle meatus |
| Anterior ethmoid | Variable, via cell ostia | Ethmoidal infundibulum | Middle meatus |
| Posterior ethmoid | Via cell ostia | Directly | Superior meatus |
| Sphenoid | Anterosuperior face of sinus | Via sphenoid ostium | Sphenoethmoidal recess (→ superior meatus) |
| Nasolacrimal duct | Via Valve of Hasner | Directly | Inferior meatus |
6. Clinical Correlates
| Condition | Mechanism | Structure involved |
|---|---|---|
| Epiphora | Obstruction of nasolacrimal duct at Valve of Hasner | Inferior meatus |
| Chronic rhinosinusitis | OMC obstruction impairs frontal, anterior ethmoid, and maxillary drainage | Middle meatus / OMC |
| Recurrent sinusitis after FESS | Missed accessory maxillary ostia causing mucus recirculation | Middle meatus |
| Frontal sinusitis | Obstruction of frontal recess (by agger nasi, frontal cells, or scarring) | Frontal recess → middle meatus |
| Sphenoid sinusitis | Obstruction of sphenoid ostium or sphenoethmoidal recess | Sphenoethmoidal recess |
| Epiphora after FESS/nasal surgery | Injury to nasolacrimal duct (especially during uncinectomy) | Inferior meatus / NLD |
Sources: Cummings Otolaryngology Head and Neck Surgery (pp. 783-784), Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 1 (pp. 1015-1023), Bailey and Love's Short Practice of Surgery 28th Ed. (p. 785), K.J. Lee's Essential Otolaryngology (pp. 511-514)
This is a shared conversation. Sign in to Orris to start your own chat.