Explain me complete prism cover test
Reading File
Finding Sources
Finding Sources
Searching Images
prism cover test strabismus measurement
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Reading File
Reading File
I now have comprehensive material. Let me compile the complete answer:
Prism Cover Test — Complete Explanation

Overview
The prism cover test (PCT) is the gold standard for measuring the angle of ocular deviation (both manifest and latent). It quantifies deviation in prism diopters (Δ) and is performed for both horizontal and vertical deviations at distance and near.
It combines two components:
- Cover tests (to detect and dissociate the deviation)
- Prism neutralization (to measure its magnitude)
Prerequisite Tests — Understanding the Cover Test Sequence
Before performing PCT, the examiner must complete the cover test sequence in order:
A. Cover-Uncover Test (Detects Phoria vs. Tropia)
Purpose: Detect heterotropia (manifest deviation) by watching the uncovered eye.
Method:
- Patient fixates a distant accommodative target straight ahead.
- The examiner covers one eye.
- Watch the uncovered (fellow) eye for any movement:
- No movement → that eye is fixing (may be orthophoric or a tropia of the covered eye)
- Movement to pick up fixation → the uncovered eye was deviated = heterotropia of that eye
Interpretation of the uncovered eye movement:
| Movement | Type |
|---|---|
| Inward (adduction) | Exotropia of that eye |
| Outward (abduction) | Esotropia of that eye |
| Upward | Hypotropia |
| Downward | Hypertropia |
Repeat for the other eye.
B. Uncover Test (Detects Heterophoria)
Purpose: Detect heterophoria (latent deviation — only present when fusion is disrupted).
Method:
- Cover one eye for 2–3 seconds.
- Remove the cover and watch that eye:
- No movement → orthophoria
- Nasal recovery (adduction) → exophoria
- Temporal recovery (abduction) → esophoria
- Vertical recovery → vertical phoria
The speed and smoothness of recovery indicates the strength of motor fusion.
Most examiners perform the cover test and uncover test together — hence the term cover-uncover test.
C. Alternate Cover Test (Dissociates Fusion, Reveals Total Deviation)
Purpose: Break down all fusion and reveal the total deviation (phoria + tropia combined). This maximally dissociates the eyes.
Method:
- Cover the right eye for several seconds.
- Quickly shift the occluder to the left eye for 2 seconds, then alternate repeatedly.
- Note movement of the eye being uncovered on each shift.
Key rule: Always perform the cover-uncover test before the alternate cover test, as the alternate cover test dissociates fusion completely and may cause a phoria to break down into a tropia.
The Prism Cover Test (Quantification)
Purpose: Measures the exact angle of deviation in prism diopters.
Equipment:
- Occluder
- Prism bar (a column of prisms of progressive strength, e.g., 1Δ to 45Δ or more)
- Fixation targets (distance: 6 m; near: 33 cm)
Step-by-Step Technique
Step 1 — Perform the alternate cover test first to establish the direction and approximate magnitude of deviation.
Step 2 — Position the prism:
- Place prisms in front of one eye (usually the deviating eye or the eye with less vision).
- The base of the prism is placed opposite to the direction of deviation (i.e., the apex points in the direction of the deviation):
| Type of Deviation | Prism Orientation |
|---|---|
| Esotropia (convergent) | Base-out (BO) |
| Exotropia (divergent) | Base-in (BI) |
| Right hypertropia | Base-down before right eye (or base-up before left eye) |
| Right hypotropia | Base-up before right eye |
Step 3 — Continue alternate cover test while increasing prism strength:
- While alternately covering, introduce progressively stronger prisms from the prism bar.
- The refixation movement seen during alternate cover testing gradually decreases as the prism strength approaches the true angle of deviation.
Step 4 — Find the endpoint:
- The endpoint is the prism strength at which no movement is observed during alternate covering.
- To confirm the maximum angle, increase the prism slightly further until a movement in the opposite direction is observed (the point of reversal).
- Reduce back to the neutral value.
- The angle of deviation = strength of prism at which no movement occurs.
Measurement Positions
Measurements are routinely taken in:
| Position | Notes |
|---|---|
| Primary position at distance (6 m) | Standard; both with and without glasses |
| Primary position at near (33 cm) | Accommodative component assessed |
| Far distance | Especially important for intermittent exotropia |
| Right gaze | Head turned left, patient fixates target |
| Left gaze | Head turned right |
| Upgaze | Head tilted down |
| Downgaze | Head tilted up |
| Head tilt right / head tilt left | Used in vertical deviation workup (3-step test) |
Practical Tips
- Always use an accommodative target (letters/pictures), not a light source — using a light causes the patient to relax accommodation and may give false readings.
- The test must be done before the patient becomes fatigued from prolonged dissociation.
- In intermittent exotropia, measure at far distance (>6 m) as the deviation may only manifest at distance.
- In incomitant strabismus (e.g., cranial nerve palsies), PCT is also useful, performed in multiple gaze positions to map the field of deviation.
- When measuring a vertical and horizontal deviation simultaneously, use a compound prism or measure one component at a time.
What the PCT Measures vs. Does Not Measure
| Measures | Does Not Measure |
|---|---|
| Total angle of deviation (manifest + latent) | Cyclodeviations (need Maddox rod) |
| Deviation in different gaze positions | Near point of convergence |
| Distance vs. near deviation | Sensory status (stereopsis, suppression) |
Clinical Significance
- Preoperative planning: The PCT angle directly determines the amount of surgical correction (muscle recession/resection).
- AC/A ratio: Comparing distance vs. near PCT measurements allows calculation of the accommodation-convergence to accommodation ratio.
- Monitoring: Serial PCT measurements track progression or response to treatment (glasses, patching, surgery).
- Incomitant squint: Measurements in all nine positions of gaze are plotted on a synoptophore chart or Hess chart for full assessment.
Summary
Cover-uncover test → detects tropia (manifest)
Uncover test → detects phoria (latent)
Alternate cover → reveals total deviation (tropia + phoria)
Prism cover test → QUANTIFIES the total deviation in prism diopters
Sources:
- Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed., pp. 742–743
- The Wills Eye Manual, p. 1112
Krimsky test
Finding Sources
Finding Sources
Reading File
Loading Image
Finding Sources
I have all the information needed. Here is the complete explanation:
Krimsky Test
Definition
The Krimsky test is a modified Hirschberg test that combines corneal light reflexes with prism neutralization to give a more accurate, objective measurement of the angle of manifest deviation (heterotropia). It is especially useful when the prism cover test cannot be performed — for example, in young, uncooperative, or poorly fixating patients, or when one eye has very poor or eccentric fixation.
Background — Hirschberg Test (Foundation)
The Krimsky test builds on the Hirschberg test, so understanding it is essential.
Hirschberg test:
- A penlight is shone at both eyes simultaneously while the patient looks straight ahead.
- In the fixing eye, the corneal light reflex is approximately centred in the pupil.
- In the deviating eye, the reflex is displaced in the direction opposite to the deviation:
- Reflex displaced nasally → exotropia
- Reflex displaced temporally → esotropia
- Reflex displaced inferiorly → hypertropia
- Each 1 mm of displacement ≈ 7° ≈ 14 prism diopters (Δ):
- Reflex at pupil border (2 mm off center) ≈ 15°
- Reflex at limbus ≈ 45°
Limitation of Hirschberg alone: It only gives a rough estimate because pupil size varies and the assessment is subjective.
Krimsky Test — Principle
The Krimsky test corrects for the main limitation of the Hirschberg test by using prisms to shift the corneal light reflex of the fixating eye until both reflexes are symmetrical, thereby neutralizing the deviation objectively.
"The Krimsky test involves placement of prisms in front of the fixating eye until the corneal light reflections are symmetrical." — Kanski's Clinical Ophthalmology, 10th ed.
The prism is placed in front of the fixing eye (not the deviating eye), which reduces the problem of parallax — this is why it is more commonly used than the related prism reflection test.
Technique
- Shine a penlight (or use a muscle light) equidistant from both eyes so the patient can fixate on it.
- Observe both corneal reflexes — note which eye is deviating and in which direction.
- Place a prism in front of the fixating eye with the base in the direction opposite to the deviation:
| Deviation | Prism placement before fixing eye |
|---|---|
| Esotropia (convergent) | Base-out (BO) |
| Exotropia (divergent) | Base-in (BI) |
| Hypertropia | Base-down |
| Hypotropia | Base-up |
- Increase prism strength until the corneal light reflex of the fixing eye is displaced to a position symmetrical with the reflex of the deviating eye.
- The prism strength that achieves symmetry = angle of deviation in prism diopters.
Krimsky vs. Prism Reflection Test
| Feature | Krimsky Test | Prism Reflection Test |
|---|---|---|
| Prism placed before | Fixating eye | Deviating eye |
| Parallax problem | Reduced (preferred) | More problematic |
| Clinical use | More common | Less commonly used |
Krimsky vs. Prism Cover Test
| Feature | Krimsky Test | Prism Cover Test |
|---|---|---|
| Requires cooperation | Minimal | Moderate |
| Requires fixation | Light fixation only | Good accommodative fixation required |
| Useful in poor fixators | ✅ Yes | ❌ No |
| Accuracy | Approximate | Gold standard |
| Measures | Manifest deviation only | Total deviation (manifest + latent) |
| Dissociation of fusion | Not required | Required |
Indications (When to Use Krimsky Instead of PCT)
- Infants and very young children who cannot cooperate with cover testing
- Patients with very poor vision in one eye (cannot fix on a target)
- Patients with eccentric fixation — the deviating eye fixes off the fovea, making cover test results unreliable
- Nystagmus patients — where the cover test is difficult to interpret
- Quick bedside estimation when full orthoptic assessment is not possible
Limitations
- Less accurate than the prism cover test (no dissociation of fusion, no assessment of phoria)
- Does not reveal latent deviations (heterophoria)
- Angle kappa (the angle between the visual axis and the pupillary axis) can cause errors — a positive angle kappa can simulate exotropia and a negative angle kappa can simulate esotropia on corneal reflex tests
Summary
The Krimsky test = Hirschberg test + prism neutralization before the fixing eye. It is the go-to objective method for estimating deviation angle when the prism cover test is not feasible, particularly in uncooperative or poorly fixating patients.
Source: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed., p. 742
Prism reflection test
Finding Sources
Finding Sources
Reading File
The textbook entry for the prism reflection test is brief (one sentence), as it is typically discussed together with the Krimsky test. Here is the complete explanation drawing on that content plus the surrounding context:
Prism Reflection Test
Definition
The prism reflection test is a modified Hirschberg test that measures the angle of manifest strabismus by placing prisms in front of the deviating eye until the corneal light reflections of both eyes become symmetrical.
"The prism reflection test involves the placement of prisms in front of the deviating eye until the corneal light reflections are symmetrical." — Kanski's Clinical Ophthalmology, 10th ed.
Principle
Like the Krimsky test, it is built on the Hirschberg corneal reflex method:
- A penlight is shone equidistant from both eyes.
- In a normal (fixing) eye, the corneal light reflex sits near the centre of the pupil.
- In the deviating eye, the reflex is displaced opposite to the direction of the deviation.
The prism is then used to optically redirect the light entering the deviating eye, shifting its corneal reflex until it matches the position of the reflex in the fixing eye — at which point the prism strength equals the angle of deviation.
Technique
- Shine a penlight equidistant from both eyes.
- Identify the deviating eye and note the direction of reflex displacement.
- Place a prism in front of the deviating eye, with the base in the direction opposite to the deviation:
| Deviation | Prism base before deviating eye |
|---|---|
| Esotropia | Base-out (BO) |
| Exotropia | Base-in (BI) |
| Hypertropia | Base-down |
| Hypotropia | Base-up |
- Increase prism strength until the corneal light reflex of the deviating eye aligns symmetrically with the reflex of the fixing eye.
- The neutralizing prism strength = angle of deviation in prism diopters.
Prism Reflection Test vs. Krimsky Test
Both tests use the same endpoint (symmetrical corneal reflexes) but differ in which eye the prism is placed before:
| Feature | Prism Reflection Test | Krimsky Test |
|---|---|---|
| Prism placed before | Deviating eye | Fixing eye |
| Parallax problem | More — deviating eye may not fix the light properly | Less — fixing eye maintains stable fixation |
| Clinical preference | Less commonly used | More commonly used |
| Accuracy | Slightly less reliable | More reliable |
The key disadvantage of the prism reflection test is parallax error: because the deviating eye is not fixing on the light, the examiner cannot be certain the reflex displacement is being correctly assessed. When the prism is placed before the fixing eye (Krimsky), the fixing eye maintains reliable fixation throughout, making reflex symmetry easier and more accurate to judge.
Indications
Both the prism reflection test and Krimsky test are used when the prism cover test cannot be performed, typically:
- Uncooperative or pre-verbal children
- Patients with very poor vision or eccentric fixation
- Patients with nystagmus
- Bedside or rapid estimation of deviation angle
Limitations
- Does not measure latent deviations (heterophoria) — only manifest deviations (heterotropia)
- Less accurate than the prism cover test
- Susceptible to angle kappa errors:
- Positive angle kappa (visual axis nasal to pupillary axis) → simulates exotropia
- Negative angle kappa (visual axis temporal to pupillary axis) → simulates esotropia
- Parallax is a greater issue here than with the Krimsky test
Summary
The prism reflection test = Hirschberg + prism before the deviating eye. It is the less-preferred counterpart to the Krimsky test. Both give an approximate objective measurement of manifest deviation angle, but the Krimsky test (prism before the fixing eye) is more commonly used because it reduces parallax error.
Source: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed., p. 742
What is angle Kappa
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
I have all the content needed. Here is the complete explanation:
Angle Kappa
Definition
Angle kappa is the angle subtended between the visual axis and the anatomical (pupillary) axis of the eye.
"Angle kappa is the angle, usually about 5°, subtended by the visual and anatomical axes." — Kanski's Clinical Ophthalmology, 10th ed.
Understanding the Two Axes
To grasp angle kappa, the two axes must be distinguished:
| Axis | Definition |
|---|---|
| Anatomical (pupillary) axis | A line passing through the centre of the cornea to the posterior pole of the eye |
| Visual axis | A line from the fixation point through the nodal point of the eye to the fovea |
In a perfectly symmetrical eye, these two axes would coincide. However, the fovea is normally situated slightly temporal to the anatomical centre of the posterior pole. To direct the visual axis at an object straight ahead, the eye must be very slightly abducted. This creates a small angular difference between the two axes — this is the angle kappa.
Normal Angle Kappa
- Normally ~5° and positive
- Because the fovea is temporal to the posterior pole, the visual axis is directed slightly nasally relative to the anatomical axis
- When a penlight is shone at the eye, the corneal light reflex falls just nasal to the centre of the pupil in both eyes — this is the normal, positive angle kappa appearance
Positive vs. Negative Angle Kappa
| Type | Fovea position | Corneal reflex position | Clinical appearance |
|---|---|---|---|
| Positive (normal) | Temporal to posterior pole | Nasal to pupil centre | Normal; or if large → pseudoexotropia |
| Negative | Nasal to posterior pole (rare) | Temporal to pupil centre | Pseudoesotropia |
Large Positive Angle Kappa → Pseudoexotropia
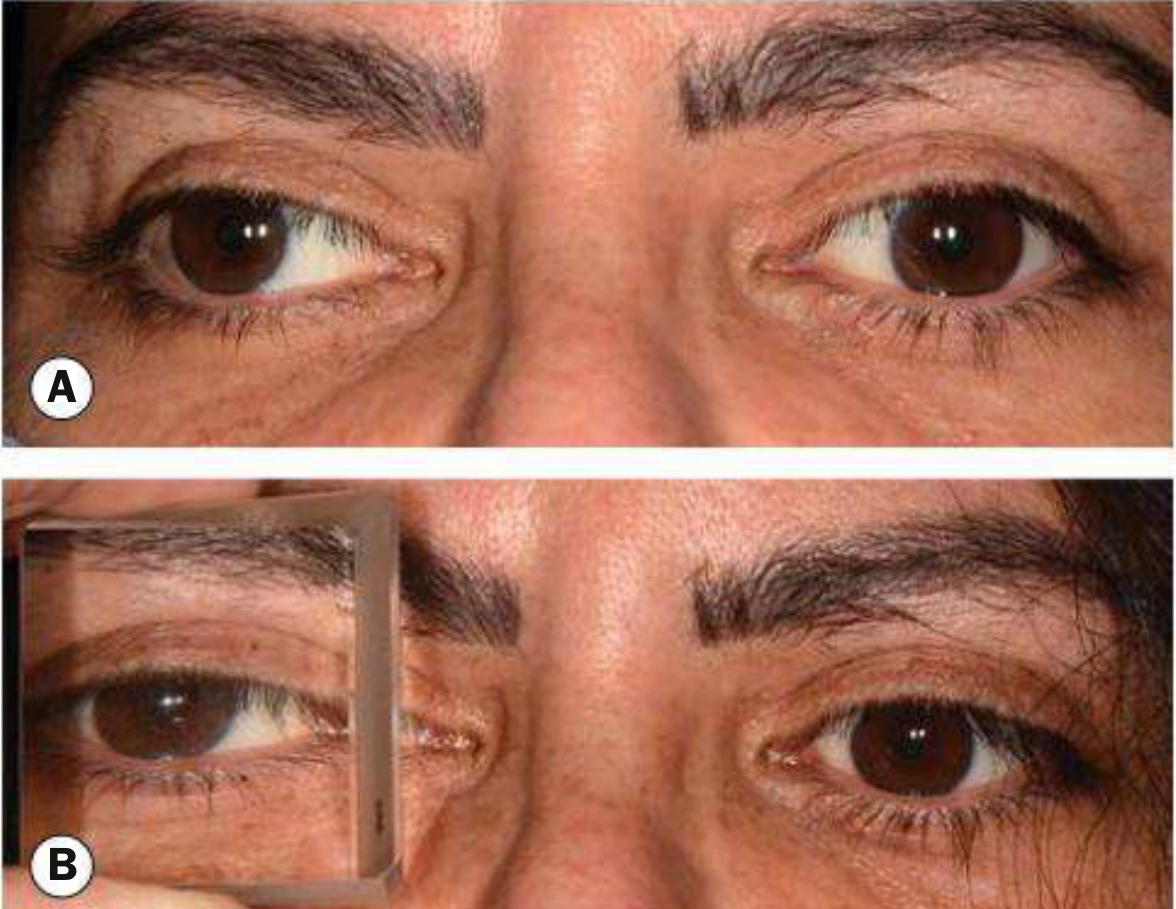
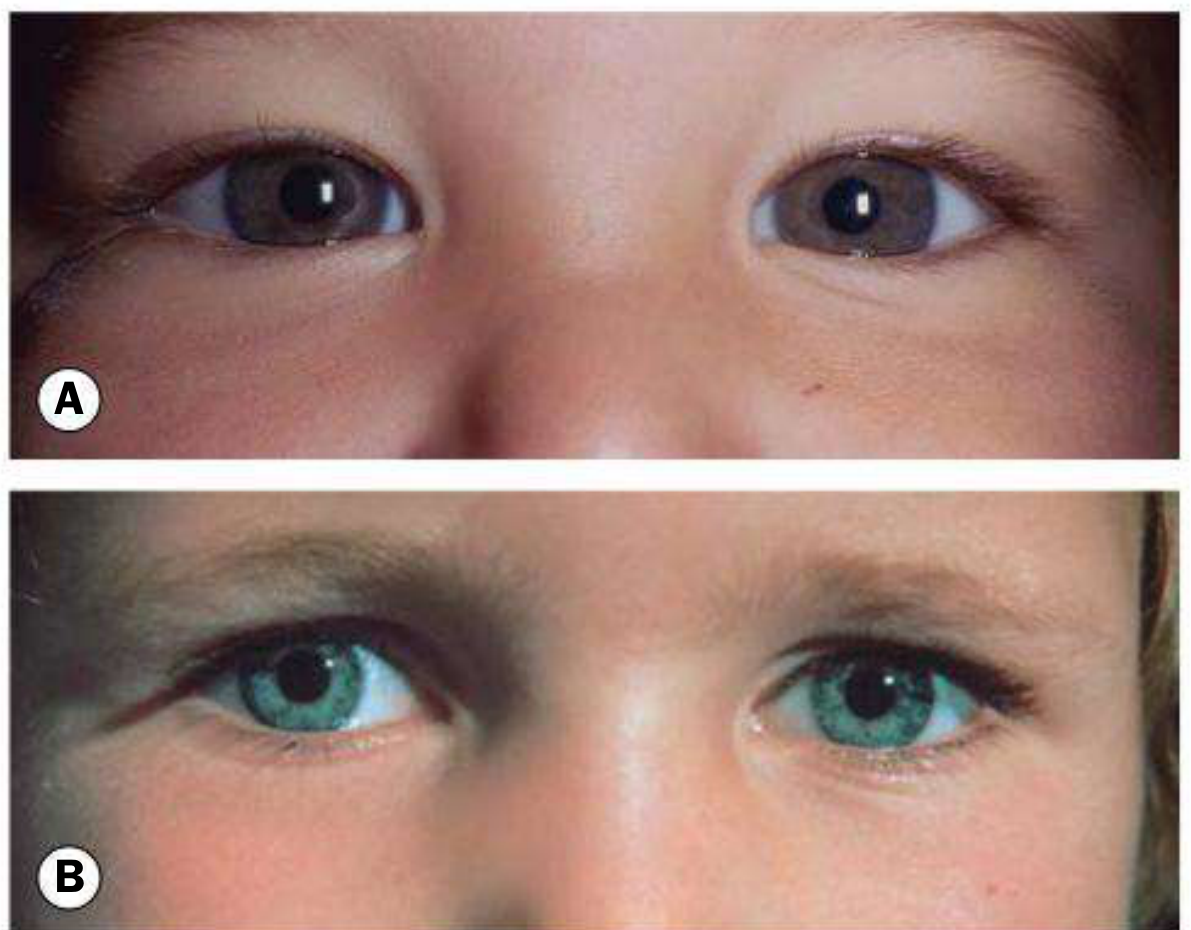
A large positive angle kappa occurs when the macula is displaced temporally (e.g. in retinopathy of prematurity with temporal dragging of the macula). The corneal reflex shifts well nasal to the pupil centre, mimicking the reflex pattern seen in exotropia — even though the eyes are perfectly aligned (Fig. A below: epicanthic folds simulating esotropia; Fig. B: wide IPD simulating exotropia in the same pseudostrabismus context).
Causes of large positive angle kappa (pseudoexotropia):
- Retinopathy of prematurity (temporal macular dragging)
- Coloboma displacing the macula
- High hypermetropia (relative temporal displacement)
Negative Angle Kappa → Pseudoesotropia
When the fovea is nasal to the posterior pole, the visual axis is directed slightly temporally, pushing the corneal reflex temporally — mimicking an esotropia.
Cause of negative angle kappa:
- High myopia — the elongated globe causes the fovea to be placed more nasally relative to the posterior pole
Clinical Significance
1. Pseudostrabismus
The most important clinical implication — angle kappa can create the false impression of a squint on Hirschberg, Krimsky, and prism reflection tests when no true deviation exists. The cover test (which is the definitive test) will show no movement, confirming the eyes are truly aligned.
2. Errors in corneal reflex-based tests
Angle kappa introduces error in:
- Hirschberg test — the reflex position may suggest deviation where none exists
- Krimsky test — an unjustifiably large prism may be required to centre the reflex
- Prism reflection test — same issue
3. Refractive surgery planning
Angle kappa is measured preoperatively for LASIK and phakic IOL implantation. A large angle kappa can cause postoperative glare/halos if the ablation zone is not centred on the visual axis.
How to Detect / Measure Angle Kappa
- Clinically: Hirschberg penlight test — observe where the corneal reflex falls relative to the pupil centre
- Corneal topography / Pentacam — measures the distance between the pupil centre and the visual axis (corneal vertex)
- Synoptophore — used to measure angle kappa more precisely in an orthoptic setting
- Confirmation of pseudostrabismus: Cover test shows no movement, confirming no true deviation despite reflex asymmetry
Summary
Angle kappa = angle between visual axis and anatomical axis
Normal = ~5°, positive (fovea temporal, reflex slightly nasal)
Large +ve = pseudoexotropia (e.g. ROP, temporal macular drag)
Negative = pseudoesotropia (e.g. high myopia, nasal fovea)
Key rule = Cover test normal → pseudostrabismus, not true squint
Source: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed., pp. 720, 751
This is a shared conversation. Sign in to Orris to start your own chat.